
Abstract
A paroxysmal stabbing or icepick-like headache in the multiple nerve dermatomes, especially involving both trigeminal and cervical nerves, has not been fully explained or classified by the International Classification of Headache Disorder, 2nd Edition (ICHD-II). Of patients with acute-onset paroxysmal stabbing headache who had visited the Hallym University Medical Center during the last four years, 28 subjects with a repeated stabbing headache involving multiple dermatomes at the initial presentation or during the course were prospectively enrolled. All patients were neurologically and otologically symptom free. A coincidental involvement of both trigeminal and cervical nerve dermatomes included seven cases. Six cases involved initially the trigeminal and then cervical nerve dermatomes. Five cases showed an involvement of the cervical and then trigeminal nerve dermatomes. The remaining patients involved multiple cervical nerve branches (the lesser occipital, greater occipital and greater auricular). Pain lasted very shortly and a previous history of headache with the same nature was reported in 13 cases. Preceding symptom of an infection and physical and/or mental stress were manifested in seven and six subjects, respectively. All patients showed a self-limited benign course and completely recovered within a few hours to 30 days. Interestingly, a seasonal gradient in occurrence of a stabbing headache was found in this study. A paroxysmal stabbing headache manifested on multiple dermatomes can be explained by the characteristics of pain referral, and may be considered to be a variant of primary stabbing headache or occipital neuralgia.
Introduction
A stabbing headache in the head and neck lasting a few seconds is one commonly encountered headache. According to the International Classification of Headache Disorders 2nd edition (ICHD-II) established by the International Headache Society (IHS) in 2004, such stabbing headache exclusively or predominantly in the dermatome of the first trigeminal nerve branch is defined as a primary stabbing headache (PSH) (1). However, a clinically encountered stabbing headache is more often observed in the extra-trigeminal nerve branches. Particularly, a headache may move to the cervical dermatome or occur coincidentally, or occur in the cervical dermatome and then move to the trigeminal dermatome. Accordingly, it is not uncommon to have a headache in more than one nerve branch (2–5).
Such a stabbing headache is not sufficient for classification with ICD-II alone. Furthermore, the mechanism through which a headache develops in various nerve branches has not been elucidated either. Thus, we analysed the clinical features of a stabbing headache that had developed in multiple dermatomes of the head and neck, and considered the mechanism of development and classification of such a headache.
Methods
The patients had a chief complaint of a paroxysmal stabbing headache, and had visited the Neurology Outpatient Clinic at the Hallym University Medical Centre for 4 years prior to July 2005. This prospective study included 28 patients who met the ICHD-II diagnostic standard for PSH other than the area of involvement and had a repeated stabbing headache involving multiple dermatomes at the initial presentation or during the clinical course.
All patients underwent not only a physical examination but also a medical history, along with an ENT and neurological examination. These patients also underwent blood tests, including Complete Blood Count (CBC), Erythrocyte Sedimentation Rate (ESR) and C-reactive Protein (CRP). Brain CT was performed for eight patients, including six who had experienced a similar paroxysmal stabbing headache in the past. This investigation examined the presence of an upper respiratory tract infection (URTI), flu or mental or physical stress before having such a headache as well as sex and age of a patient. The dates of onset of headache were also recorded in order to observe the seasonal distribution of such attacks.
The regions of headache were largely divided into 1st, 2nd and 3rd nerve branches of the trigeminal dermatome and upper cervical dermatome, which correspond to the 2nd and 3rd cervical nerve branches. The cervical dermatome was again divided into the lesser occipital nerve (LON), greater occipital nerve (GON) and the greater auricular nerve (Fig. 1).

Dermatomes in the head and neck. Modified from Haymaker W, Woodhall B. Peripheral Nerve Injuries. Philadelphia: Saunders, 1953.
The different types of headache were also categorized into unilateral and bilateral attacks. In addition, past medical history of primary headache, including experience of having similar headache, frequency and migraine headache, was examined. The severity of headache was assessed by using the Visual Analog Scale (VAS) (6). Drugs used for treatment were also recorded. This study also inquired into the frequency of attacks per day and the duration of recovery from having such attacks.
Results
There were 7 males and 21 females. The mean age was 52.5 ± 14.9 years old (ranging from 22 to 86 years old). Patients visited the hospital 1–20 days (with a mean duration of 5.8 days) after an attack of headache. ENT and neurological examinations showed no particular abnormal findings in any patient. Brain CT results from six patients were within normal levels. Seven patients (25%) had a history of URTI or flu before the onset of stabbing headache. The increase in ESR was investigated in five patients, four of whom had a history of URTI or flu before the onset of stabbing headache. Consequently, eight patients had either a history of a preceding infection or an increase in ESR. Most of them had attacks of stabbing headache during the winter season (two in December, one in January, and four in February) except for one (in August).
Six patients (21.4%) were found to have a present history of mental or physical stress. Thirteen out of 28 patients (46.4%) had a history of one or more similar headaches. Six (21.4%) of the female patients had previously had migraine headaches (Table 1). With respect to areas of an attack of headache, 21 patients (75%) had headache unilaterally but the remaining seven (25%) had a bilateral attack (Table 2).
Clinical characteristics of a stabbing headache in the multiple dermatomes

URTI or flu-like symptoms.
Increase in ESR, CRP or leucocytes on CBC.
Physical, mental or both kinds of stresses.
All of them were female.
Nature of stabbing headache in subgroups

T & C, coincidental involvement of both trigeminal and cervical dermatomes.
T → C, initial trigeminal and then cervical dermatome involved.
C → T, initial cervical and then trigeminal dermatome involved.
Multi-C, multiple cervical branches involved temporally.
VAS, visual analogue scale.
A total of 18 patients (64.3%) had headache that coincidentally involved both trigeminal and cervical dermatomes. Among them, seven patients (25%) showed a simultaneous involvement of both trigeminal and cervical dermatomes from the point of time of an attack. Six (21.4%) showed a shifting of their headache from the trigeminal dermatome to the cervical dermatome. Five (17.9%) showed a shifting of an attack from the cervical dermatome to the trigeminal dermatome. Ten patients (35.7%) showed a multiple cervical branch dermatome involvement, such as the lesser occipital nerve, the greater occipital nerve and the greater auricular nerve (Fig. 2).

Involvement patterns of stabbing headache in the multiple dermatomes. T & C, coincidental involvement of both trigeminal and cervical dermatomes. T → C, initial trigeminal and then cervical dermatome involved. C→ T, initial cervical and then trigeminal dermatome involved. Multi-C, multiple cervical branches involved temporally. Black bar, man; red bar, woman.
The majority of patients had ultra-short and sharp stabbing pain for a duration of 1–2 s, except for two cases, who had a longer duration of about 3 or 5 s. Nine patients (32.1%) showed clustering of recurrent stabs, which came in a burst and consisted of multiple single stabs, but not a cluster headache (Table 3).
Clinical characteristics of individual patients
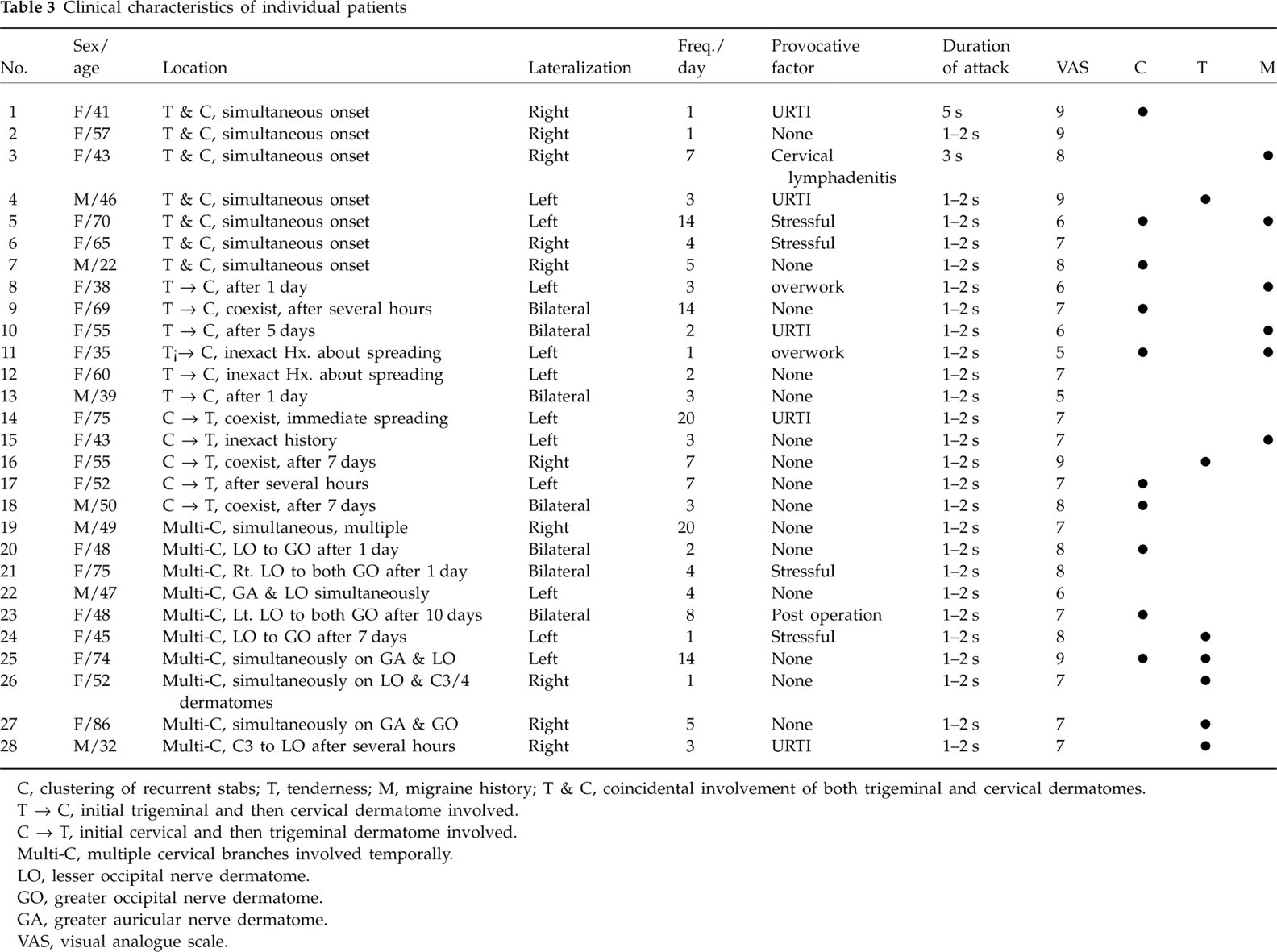
C, clustering of recurrent stabs; T, tenderness; M, migraine history; T & C, coincidental involvement of both trigeminal and cervical dermatomes.
T → C, initial trigeminal and then cervical dermatome involved.
C → T, initial cervical and then trigeminal dermatome involved.
Multi-C, multiple cervical branches involved temporally.
LO, lesser occipital nerve dermatome.
GO, greater occipital nerve dermatome.
GA, greater auricular nerve dermatome.
VAS, visual analogue scale.
The severity of headache using the VAS was 7.3 ± 1.2 (5–9) points on average and showed a headache of moderate to severe degree. Mean VAS of headache with simultaneous involvement of both trigeminal and cervical dermatomes was high (8.0 ± 1.2) and that of headache shifting from the trigeminal to cervical dermatome was low (6.9 ± 0.9) (Table 2).
The mean frequency of attacks of headache was 5.8 ± 5.6 times/day (1–20/day) on average until the time of recovery. This was most frequent in patients with headache shifting from the cervical to the trigeminal dermatome (8.0 ± 7.0). On the other hand, patients with headache shifting from the trigeminal to the cervical dermatome showed low frequency (4.2 ± 4.9) (Table 2).
Among the patients with an involvement of the cervical dermatome, seven showed tenderness in the occipital area. However, only four patients had a stabbing headache that concurred with the ICHD-II diagnostic standard for occipital neuralgia, having an attack within the cervical dermatome. The remaining three had headache that shifted to the trigeminal dermatome or began as a stabbing headache in the trigeminal dermatome and then ended in the cervical dermatome.
Except for two patients who had recovered without any drug treatment, most patients (26) showed an excellent response on a regimen of amitriptyline or naproxen sodium. Additional indomethacin, gabapentin or carbamazepine was administered in a few cases.
Recovery time varied widely, from a few hours to 30 days. Twenty patients (71.4%) had a recovery time of 14 days or less. Nine (32.1%) had a recovery time of 7 days or less. The mean recovery time was 10.7 ± 7.7 days, showing a recovery phase lasting for 10 days or less (Table 1).
Interestingly, the characteristic feature is that there are seasonal differences in the occurrence of a stabbing headache. Fourteen patients (50%) had attacks of headache in the cold winter of December, January and February. Stabbing headaches occurred frequently during a change of season, especially in the spring and fall. However, the incidence of a stabbing headache was less during the summer (June, July and August) (Fig. 3).

Seasonal distribution of stabbing headache.
Discussion
According to the ICHD-II, appearance of a PSH should characteristically be limited to the first branch of the trigeminal dermatome.
In addition to a PSH, several other primary headaches may appear with a stabbing pain in the first branch of the trigeminal dermatome. These may include trigeminal neuralgia, cluster headache, paroxysmal hemicrania and short-lived unilateral neuralgic-nature headache attacks with conjunctival injection and tearing (SUNCT). However, these headaches may have a trigger area that induces pain or may accompany autonomic nervous system symptoms such as conjunctival injection, tearing and myosis, and may have a longer duration of pain. These features permit differential diagnosis to distinguish these headaches from a PSH (1, 7, 8).
Furthermore, headaches such as occipital neuralgia (ON), geniculate or nervus intermedius neuralgia, glossopharyngeal neuralgia and sphenopalatine ganglion neuralgia may appear as a stabbing headache outside of the trigeminal nerve branches (1). Except for the dermatome of a stabbing headache pertaining to the ICHD-II diagnostic standard, and despite similarities to the pain characteristic of a PSH, they have other features that distinguish them from a PSH.
Although occipital neuralgia may have a stabbing pain similar to that of a PSH, it may show tenderness in the lesser occipital nerve or greater occipital nerve (Tinel sign) and allodynia, for which a local anaesthesia could relieve the pain. Geniculate or nervus intermedius neuralgia may have otalgia within the ear rather than in the periphery of the ear. Glossopharyngeal neuralgia shows pain in the cervical area and tonsil, while coughing and swallowing may induce pain (1, 9–11). Sphenopalatine ganglion neuralgia is also limited to pain in the endonasal area or in the periphery of the nose, rather than having pain in the skin. It is differentiated from a primary stabbing headache by having a longer duration of pain (12).
However, clinically, paroxysmal stabbing headaches similar to that of PSH are often observed in the extra-trigeminal dermatome. It would be difficult to explain even with the various diagnostic standards mentioned above. The results of this study also showed diverse clinical courses through various dermatomes. Some initially involved a typical PSH, while the pain shifted to the extra-trigeminal nerve branches. Others initially involved the cervical dermatome, with a stabbing headache that concurred with occipital neuralgia, and the pain shifted to the trigeminal dermatome. Yet other cases involved multiple dermatomes of more than two. Cases of a stabbing headache in the cervical dermatome may be a subtype of occipital neuralgia. Nevertheless, only seven subjects experienced typical tenderness or allodynia. Diagnoses by the ICHD-II standard of cases with pain that shifts to the trigeminal dermatome would be ambiguous at best.
Several studies, including that of Martin et al., reported that stabbing headaches had been expressed in the extra-trigeminal dermatome (2,5), but it was not clear whether such stabbing headache had been a PSH or a subtype of another primary headache. Also, the clear mechanism through which multiple dermatomes such as the trigeminal and cervical dermatomes got involved has not been well elucidated yet.
Kerr and Olfson (1961) suggested the basic concept of the mechanism of a primary headache, namely, the convergence of afferent inputs between the trigeminal and cervical nerves (13). In a canine experiment, Kerr and Olfson demonstrated that the convergence of afferent senses from the trigeminal and cervical nerves occurred at the dorsal, intermediate and ventral horns of the upper cervical cord. Thereafter, numerous animal studies were carried out on the nociceptive convergence of pain sensations between the trigeminal and upper cervical nerves. This was thought to be the mechanism of pain referring to a primary headache such as migraine and cluster headaches (14–17). Also, Goadsby et al. confirmed experimentally that stimulation of the GON not only increased the excitability level of the afferent sense of the meninges, but also intensified the secondary pain response of the cervical nerve after a meningeal irritation. They also demonstrated by experiment that the afferent input of the trigeminal nerve branches and that of the cervical nerve had been affecting each other within the trigeminocervical complex (TNC) in the upper spinal cords, suggesting this as the pain referral mechanism for the primary headache and cervicogenic headache (Fig. 4) (15, 16, 18).

Schematic illustrations describing the convergence of various afferent sources from trigeminal and cervical. From Bartsch T, Goadsby PJ. Anatomy and Physiology of Pain Referral Patterns in Primary and Cervicogenic Headache Disorders. Headache Currents 2005; 2:42–48.
On the other hand, according to Piovesan et al
Summarizing the results of these studies, a stabbing headache in the multiple dermatomes, like the pain referral mechanism of another primary headache, could be expressed through the afferent convergence of a sensory input within the TNC, regardless of pain originating in the cervical nerves or in the trigeminal nerve. Thus, pain in the multiple dermatomes could be expressed by a reduction of the activation threshold by central sensitization of the second-order nociceptive neurone within TNC (18).
However, despite the hypothesis above, the classification of a headache by the ICHD-II standard would still have several problems. Except for cases of a primary stabbing headache originating in the trigeminal dermatome and referring to the cervical dermatome, there are difficulties in the classification of the headache type expressed in the cervical dermatome, which were referred to the trigeminal dermatome or dermatomes of the other nerve branches within the cervical dermatome. Such cases would not be easy to consider as an intracervical or an extracervical subtype of occipital neuralgia, because they would not largely satisfy three diagnostic criteria of the ICHD-II standard: (i) the tenderness over the affected nerve, (ii) the distribution(s) of the greater, lesser and/or 3rd occipital nerves, and (iii) reduction of pain by local anaesthetic block of the nerve as well as allodynia.
In addition, as allodynia could be expressed in accordance with the pain referral mechanism of a stabbing headache of the trigeminal dermatome and nerve blocking of the cervical nerve branches had been used as one of the treatment methods for other primary headaches, such as migraine and cluster headache, it would be difficult to have a clear classification of whether such an attack was caused by pain referral of a primary stabbing headache specified by the ICHD-II standard or if it was a subtype of occipital neuralgia (18, 22).
Another distinctive feature of this study was that many stabbing headaches were experienced in cold seasons or as the weather got colder, showing a seasonal gradient. No study has been conducted on the seasonal change of a stabbing headache and pathophysiology with respect to seasonal change has not been clearly researched yet. Cold weather or changes in external temperature may act as a stress factor; precipitate nerve inflammation supported by an increase in ESR/CRP correlates with the fact that URTIs tend to increase during a change of season. They might be related to seasonal changes in stabbing headache, and further investigations should be carried out regarding this issue. On the other hand, having been related to inflammatory markers and history of URTI, it is possible that the causes of a stabbing headache might be associated with inflammation and infection.
Accordingly, a prospective study involving more patients would be necessary in order to find an appropriate method of classification of a stabbing headache and to inquire into the pathophysiology and causes of stabbing headache.