
Abstract
The objective was to test whether exposure to radio frequency (RF) fields from mobile phones may cause head pain or discomfort and whether it may influence physiological variables in individuals attributing symptoms to mobile phones, but not to electromagnetic fields in general. Seventeen eligible individuals, who experienced these symptoms in an open provocation test, took part in a double-blind, randomized provocation study with cross-over design. Sixty-five pairs of sham and mobile phone RF exposures were conducted. The increase in pain or discomfort (visual analogue scales) in RF sessions was 10.1 and in sham sessions 12.6 (P = 0.30). Changes in heart rate or blood pressure were not related to the type of exposure (P: 0.30-0.88). The study gave no evidence that RF fields from mobile phones may cause head pain or discomfort or influence physiological variables. The most likely reason for the symptoms is a nocebo effect.
Introduction
Some people report symptoms in connection with mobile phone calls, and epidemiological studies indicate that the use of mobile phones may be related to occurrence of subjective symptoms (1, 2). Except from the heat sensations, headache is the most frequently reported symptom attributed to mobile phone use and the symptoms occur most often ipsilaterally to the exposure (3). Relevant to explaining these clinical and epidemiological observations are some physiological experiments on healthy individuals, showing that electromagnetic fields from mobile phones may induce alterations in the brain's blood flow, electroencephalographic wave pattern during rest (awake and sleep) (4) and excitability to transcranial magnetic stimulation (5). Conceivably, some sensitive subjects might react with headaches or other symptoms to similar physiological changes caused by electromagnetic fields from mobile phones.
Digital mobile phones, like the Global System for Mobile Communication (GSM) phones, which were used in the referred studies (4, 5) and in the present one, emit both high-frequency, i.e. radio frequency (RF), electromagnetic fields and low-frequency magnetic fields due to electrical currents from the battery. Some individuals claim to react specifically to mobile phones, whereas others attribute their symptoms to various sources of electromagnetic fields, including sources of only low-frequency fields (3, 6). The latter often regard themselves as ‘electromagnetic hypersensitive’ (6). Studies have indicated that such individuals may have abnormal autonomic nervous system regulation (7–9) and their sensory response to flickering light (7, 10) differs from that of controls. Some deviations have also been found in a group of individuals who were sensitive to mobile phones only, but these deviations are different from those observed among electromagnetic hypersensitive subjects (11).
In two previous provocation studies with mobile phones (12, 13), no evidence for a connection between the exposure and occurrence of subjective symptoms was found, but in these studies no differentiation was made between individuals with general electromagnetic hypersensitivity and those with specific sensitivity to mobile phone use. Also, Wilén et al. (11), who included only people attributing their symptoms exclusively to mobile phone use, found no statistically significant effect of RF exposure. However, the number of subjects reporting symptoms only after RF exposure was twice that reporting symptoms only after the sham exposure (8 vs. 4) and six individuals experienced symptoms after both RF and sham exposure. Possibly, a grading of the response, e.g. by registering the severity of the symptoms, or increasing the number of subjects, might have given a statistically significant difference.
In the present provocation study we wanted to include participants who experienced symptoms only during or after mobile phone calls, and not when using or being near sources of low-frequency electromagnetic fields. We were interested in the effect of the RF fields only (i.e. not the low-frequency field) and we decided to expose a relatively large area around the ear to increase the chance that a possible target tissue or organ would be affected. In order to increase the probability of revealing a possible relation between the RF fields from mobile phones and the symptoms we wanted to select participants carefully and do a study with a high estimated statistical power.
Since headache seems to be the most frequently reported symptom in connection with mobile phone calls, our main aim was to test whether exposure to RF fields from mobile phones would result in more head pain or discomfort than sham exposure in a double-blind provocation study. We also wanted to test possible effects on physiological parameters such as heart rate and blood pressure.
Subjects and methods
Selection of participants
The selection criteria aimed at identifying individuals who were between 18 and 65 years of age without other serious health conditions and who regularly experienced pain or discomfort in the head during or shortly after mobile phone calls lasting between 15 and 30 min. People with symptoms when using ordinary phones, visual display terminals or when being in the vicinity of other electric devices, i.e. indicating a general hypersensitivity to electromagnetic fields, were excluded. Possible masking of an effect of the RF exposure was avoided by excluding those who experienced frequent headaches (>2/week) not distinguishable from the pain/discomfort attributed to the use of mobile phones.
Invitations to participate in the study were by advertisements in local newspapers (Trondheim area) and by posters. Television and newspaper coverage of the project also facilitated recruitment to the study. Those who responded were first screened by a telephone interview performed by trained study nurses, and potential participants were then mailed a questionnaire to be completed at home. The authors selected individuals based on the questionnaires and in most instances an additional phone call was required to obtain specification of the information given in the questionnaire. As a last test to verify potential mobile phone hypersensitivity, eligible individuals who had given written consent were subjected to an open provocation test. Only those who developed symptoms similar to those reported when using the mobile phone were invited to take part in the double-blind study. The open test also helped the participants to get accustomed to the test environment and procedures. The participants were reimbursed for travel costs and inconvenience [€45 (£30) per completed trial].
Of 42 individuals who completed the questionnaire, 38 were eligible for the open provocation test. Two refused to participate. Based on the results from the open provocation test, 24 individuals were found suitable to proceed to the double-blind sessions. Of these, six declined to continue (three for health reasons) and one took part in only one single double-blind session. The results from this person were not used because at least one pair of tests was required for the statistical analyses. Hence, 17 subjects, five female and 12 male, were included in the double-blind study. The participants were recruited from February to September and the double-blind trials were conducted from March to November 2005.
The age of the participants ranged from 20 to 58 years (mean 39). Seven reported that they always experienced symptoms when a mobile phone call lasted at least 15 min, eight had symptoms at more than every second call, one at every third to second call and one less frequently than every third call. Fourteen of the participants reported that the symptoms usually started during the call and three that the symptoms started within an hour after the call.
Exposure
We used two exposure conditions, RF and sham. The exposure system was the same as used by Wilén et al. (11). The RF signal, 902.4 MHz in pulses with a rate of 217 Hz, a duty factor of 1/8 and a peak power at 23 dBm (∼0.2 W), was generated by a test GSM mobile phone. The level was adjusted with Radiall attenuators (−30 dB) and amplified (+50 dB) by an Ophir 5802064 power amplifier. A power divider (MCLI CI-20) directed a part of the signal to an HP 437B power meter and another part to either of two antennae (RF exposure) or to an ohmic load (Thermaline 8080) that absorbed the energy of the signal (sham exposure).
The antennae (wall-mounted base station antennae, see Hubert et al. (14)) were mounted symmetrically at the sides of the subject's head. Wooden bars restricted the sideways movements of the head and positioned the antennae 8.5 cm from the head. The specific absorption rate (SAR) was relatively uniformly distributed over a large area around the ear (see Wilén et al. (11) for illustration). The spatial peak SAR1 g (averaged over 1 g) was 1.0 W/kg and SAR10 g was 0.8 W/kg (11). The RF exposure was given on the side the person normally used the mobile phone. For those who did not have any preferred side, the side of exposure was selected by chance.
The exposure equipment, except the antennae, was placed in a control room next to the shielded exposure room. Therefore the low-frequency fields from the equipment and the low-frequency magnetic fields from the mobile phone were negligible. The maximum background level of RF signals from GSM base stations was −105 dBm in the exposure room. For an hour after the exposure the subjects were in an adjacent room. Here the maximum signal level was −78 dBm.
Study design and procedure
One test session with RF exposure and one with sham exposure constituted one pair of trials. Each subject was allowed to take part in a maximum of four pairs. Among the four pairs of trials assigned to a subject, the RF session came first twice. The order of pairs was randomized and a list specifying the order of RF and sham trials for each subject was prepared before enrolment by one of the authors (G.O.). When subjects were enrolled, they were assigned the next listed series of exposures that was not already allocated. To allow for full recovery, there was at least 2 days between test sessions.
A test session lasted almost 2 h, allowing for an adaptation and rest period before the start of registration of pulse and blood pressure and the exposure. The time schedule is shown in Fig. 1. The exposure lasted for 30 min, but the subjects could at any time indicate that they wanted the exposure to be terminated. In these cases the exposure and the registration of physiological variables were stopped immediately. During the period of physiological registrations and exposure the subjects were comfortably seated while looking at videos showing nature and wildlife films. They were observed with a web camera.

The time schedule of a test session, from arriving at time 0 until leaving the laboratory nearly 2 h later.
Registration of symptoms and physiological variables
The subjects indicated the degree of symptoms in a questionnaire at the times shown in Fig. 1 and every hour until 7 h after having left the laboratory. At the first registration after the exposure, they also specified the maximum degree of symptoms during exposure. The degree of headache and ‘other symptoms’ were indicated on two 100-mm visual analogue scales (VAS). They were asked to specify ‘other symptoms’. The scales were anchored at ‘no pain or discomfort’ and ‘unbearable pain’.
At the registration shortly after the exposure the subjects also indicated if they assumed that they had been exposed. If the answer was yes, they were asked to explain what made them believe so and to indicate whether they believed they had been exposed at the left, right or both sides of the head.
Heart rate and diastolic and systolic blood pressure were recorded continuously from 10 min before exposure until 5 min after exposure using a 2300 Finapres® Blood Pressure Monitor. The output data were given as running averages over four heart beats. The recordings of blood pressure were sensitive to the position of the cuff on the finger. The system had to be recalibrated when a presumed false decline in the recorded pressure occurred. Before breaking the code with respect to the exposure conditions, the physiological recordings were visually inspected. Periods with unreliable data due to the recording system, indicated by a change in blood pressure as a result of a recalibration, were excluded from statistical analysis. The heart rate recordings during the seconds of the recalibrations were also affected and therefore excluded from analysis.
Control of factors that might influence the symptoms
In order to ensure double blinding of the study, the list with the order of sham and RF exposures that were assigned to each subject was available only for the coworkers who controlled the exposure. These coworkers were not in direct contact with the test subjects or with the coworkers who were in contact with the subjects. Participants were informed that they would sometimes be exposed to fields from a mobile phone and sometimes not. They were not informed about which one of the antennae was used.
Electric wires and electronic equipment in the laboratory were shielded to avoid interference from the RF signals. The blinding of the system was tested by other individuals without reported sensitivity to mobile phone RF fields by subjecting them to a pair of trials (sham and RF exposure), some prior to the start of the study and some during the last weeks of the study period. After each exposure the subjects registered if they believed they had been exposed and they explained what made them believe so.
Subjects were instructed not to use mobile phones without a headset or wireless phones and to avoid mental or physical stress on the day of a trial before coming to the laboratory. On arrival in the laboratory, they had to fill in a questionnaire asking about use of mobile phones and other factors that might influence the symptoms, including the use of medications earlier the same day. The temperature in the exposure room was monitored with a mercury thermometer immediately before and after registration of the physiological variables.
Effect variables and statistical methods
The primary effect variable defined a priori was the maximum change in ‘pain/discomfort’ during and until 1 h after exposure, calculated relative to the degree of a symptom before the start of exposure. The degree of pain/discomfort at any time was defined as the maximal value on one of the two VASs, i.e. headaches and other symptoms. However, ‘other symptom’ was only taken into consideration if it was described as a localized pain or discomfort in the head, excluding symptoms such as nausea, vertigo, tinnitus and perceived hearing loss. Separate analyses were done for headache and other symptoms, as secondary effect variables. Paired t-tests were used for testing possible differences between RF and sham exposures with respect to the symptoms.
The mean values of the physiological variables were calculated for each 5-min interval from 5 min before exposure (pre-exposure values) until 5 min after exposure. The effect of the exposure measured during the 5-min intervals of exposure relative to pre-exposure values was tested by repeated measures analysis of variance (
Fisher's exact test was used to test the association between exposure type and the subjects' own assumption of exposure (RF or sham) and the association between the side of exposure and assumed side.
A result was regarded as statistically significant when P ≤ 0.05. SPSS (version 13.0 and 14.0) packages were used for the analyses (SPSS Inc., Chicago, IL, USA).
Statistical power
When planning the study, estimates of the possible effects on head pain or discomfort of an exposure session and of the standard deviation for the test variable were not available. Therefore it was decided to use relative values for power calculations. We wanted to be able to detect a difference between sham and RF exposure that was half the standard deviation for this difference. Applying a significance value of 5% and assuming 60 pairs of trials, the estimated statistical power was 96% for a paired t-test (15) as described above.
Approval of the study
The criteria of the Helsinki declaration were followed. The study was approved by the Regional Committee for Research Ethic and the permission for the person register was given by Norwegian Social Science Data Services.
Results
Double-blind trials
Fifteen of the subjects completed all four pairs of trials, whereas one could participate in only two and one in three pairs of tests, both for practical reasons. In total, 65 pairs of trials were conducted. One subject had to interrupt one session due to nausea approximately 2 min after the end of the exposure, i.e. during the last 5 min of registration of the physiological data. The remaining registrations of symptoms were completed and the data were included in the statistical analysis. On two occasions, a subject heard a humming noise from the loudspeakers during the exposure. These sessions were replaced by new sessions (without the subject's knowledge). Except for these two events, no clues other than subjective symptoms could reveal the type of exposure.
Symptoms
In some instances the subjects reported having symptoms when arriving in the laboratory. With respect to head pain/discomfort this happened three times, once before sham exposure and twice before RF exposure. When comparing sham and RF sessions before exposure, the difference in severity was not statistically significant. This was the case for all groups of symptoms.
The subjects experienced an increase in pain/discomfort during most of the trials (in 68% of all, RF and sham). In general, the registered degree of symptoms was relatively low. There was no relation between the degree of symptoms and the order of trials (linear regression: slopes −0.10–0.024 degree/trial and P: 0.88–1.00 for the three symptom variables). When a symptom occurred, it started or increased before the first postexposure registration in 96% of the trials, and always before the subjects left the laboratory an hour after exposure. The maximal degree of pain/discomfort occurred in 57% of the tests during or within the 1-h period when the subject was in the laboratory. In some cases the symptoms disappeared before the subject left, but recurred later and sometimes with higher intensity. The time pattern was similar for headache and for other symptoms and was almost identical when RF and sham exposures were used.
The increase in severity was slightly higher with sham exposure than with RF exposure for pain/discomfort as well as for headache and other symptoms. For no symptom was the difference statistically significant. Among the pairs of RF and sham exposures, the sham exposure most often resulted in the greatest increase in symptoms (Table 1). Two participants experienced the greatest increase during RF exposures for all four pairs of tests, and two participants consistently experienced the greatest increase during the sham exposures within each pair.
Maximal degree of symptom in RF and sham sessions and number of pairs with different outcome

Maximal degree of symptom after subtracting the pre-exposure value (Mean). Number of pairs in which the degree of symptom was highest for the RF session (SymRF > SymS), equal for the two exposure conditions (SymRF = SymS) and highest for sham (SymS > SymRF). RF, Radio frequency. N = 65 pairs.
Perceived exposure
As indicated in Table 2, the subjects believed that they had been exposed in most cases, both after RF exposure and after sham exposure. They more often believed so when RF exposure had been used, but the correlation between the type of exposure and what they believed was not statistically significant (P = 0.27).
Relation between real and assumed exposure

One missing value.
After sham exposure the subjects equally often assumed that they had been exposed at the left and right side. When RF exposure had been used, they more often suggested the correct side of exposure than the wrong one (Table 3). However, the correlation between the side of exposure and the assumed side (when this was either left or right) was not statistically significant (P = 0.67).
Relation between side of exposure and assumed side of exposure among those who believed that they might have been exposed
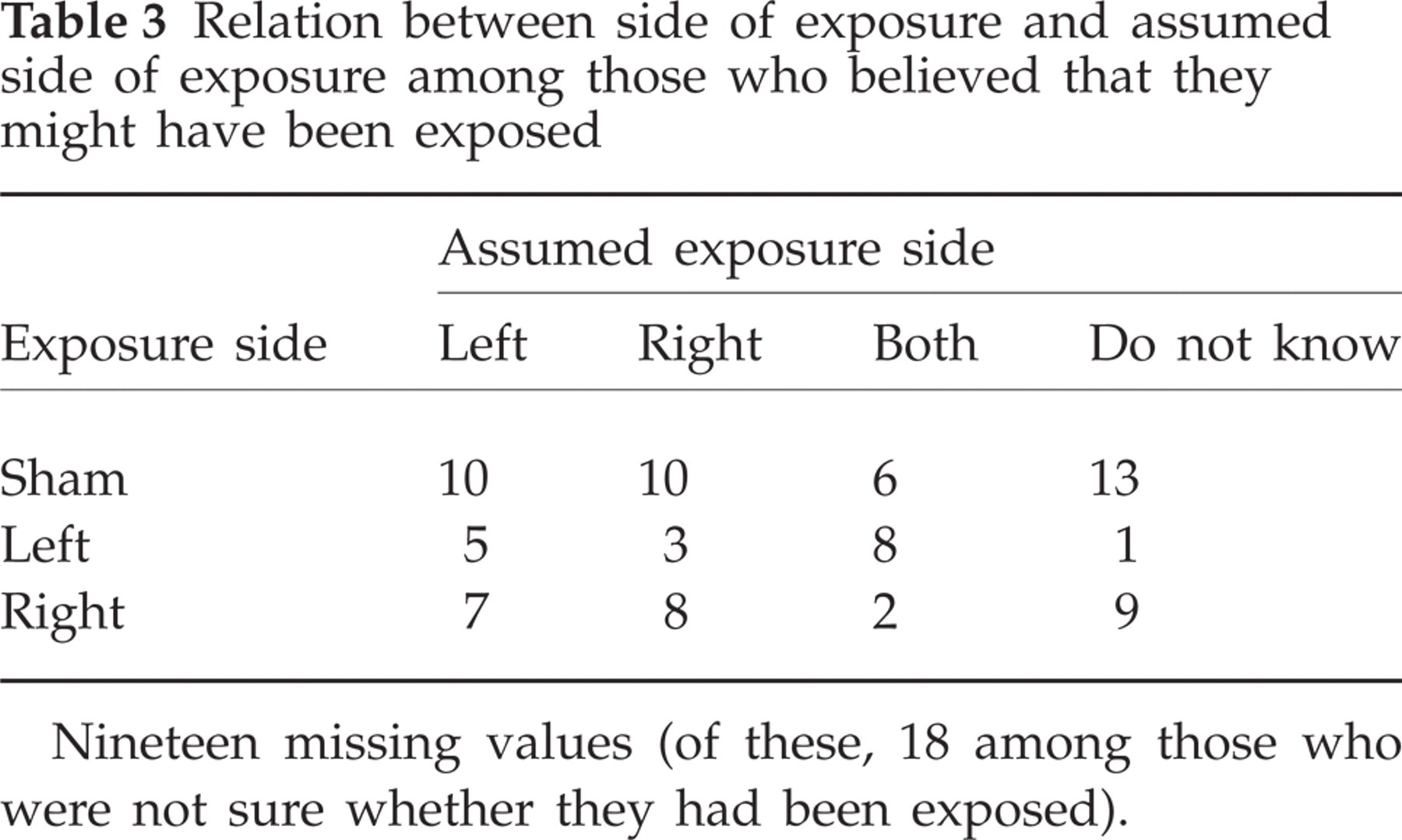
Nineteen missing values (of these, 18 among those who were not sure whether they had been exposed).
Physiological variables
Of the 130 trials conducted, systolic and diastolic blood pressure data from 21 trials were excluded from the statistical analyses due to unreliable recordings (see Subjects and methods). The heart rate data from all trials were used.
The changes occurring during the exposure using the pre-exposure values as baselines and the changes after the end of exposure using the values of the last 5 min of exposure as baseline are illustrated in Fig. 2. No effect of exposure was found either for changes occurring during exposure (P = 0.49 for heart rate, P = 0.88 for systolic and P = 0.31 for diastolic blood pressure) or for changes after the end of exposure (P = 0.30 for heart rate, P = 0.53 for systolic and P = 0.55 for diastolic blood pressure).

Changes in physiological variables during exposure (0–30 min) (after subtracting pre-exposure values) and changes after termination of exposure (30–35 min) (after subtracting values of the last 5 min of exposure). All data are averaged over 5-min intervals. ×, RF; □, sham.
Effect of other factors
Sham and RF exposure sessions were compared with respect to various factors that might influence the symptoms and/or physiological variables. The average difference between the RF and sham conditions with respect to the room temperatures was <0.1°C both immediately before and after exposure (t-tests, P = 0.47 and P = 0.77, respectively). On average, RF exposure sessions were performed 22 min later during the day than sham sessions (t-test, P = 0.67) and subjects had one mobile phone call more on the days of the RF sessions than on days with sham sessions (prior to the tests). Likewise, they used medication once more on RF exposure days compared with sham exposure days. There was no such difference in the number of times they used a cordless phone or experienced other events that might have influenced the symptoms.
Discussion
The present study demonstrates that exposure to RF fields from GSM 900 mobile phones does not cause pain or discomfort in the head or other symptoms, even in individuals carefully selected according to the criterion of a specific sensitivity to mobile phone use. In the majority of pairs of RF and sham exposures, sham resulted in the most severe symptoms. This excludes the possibility that only a few subjects with substantially more severe symptoms after sham exposure than after RF exposure were responsible for the negative results obtained from the paired t-test. Lack of evidence of an effect of the RF exposure on symptom severity also accords with the finding that subjects were unable to indicate whether or not they had been exposed. Neither could they indicate at which side they had been exposed.
In accordance with the negative results concerning the subjectively registered variables, there was no indication that the RF exposure influenced the heart rate or systolic or diastolic blood pressure. Wilén et al. (11) was also unable to identify any effect on various physiological variables (heart rate, heart rate variability, respiration, local finger blood flow, electrodermal activity and sensitivity to flickering light) from a similar exposure. This lack of effect was seen both among subjects attributing symptoms to mobile phones and among controls. If previously reported physiological alterations (4, 5) are real, the present study indicates that such alterations do not give rise to head pain or other discomforts associated with mobile phone use.
A strength of the present study is that the participants constituted a highly selected group of individuals potentially hypersensitive to mobile phone RF fields, yielding a high probability of revealing an effect, if such exists. Of particular importance was the requirement that the open test prior to the double-blind trials should elicit typical symptoms, documenting that the exposure situation was adequate, even when the low-frequency magnetic fields and the skin heating caused by holding the phone towards the ear (16) were absent. Another strength was the high statistical power of the study, due to a high number of tests and the use of measurements with graded responses. In addition, strict control of the experimental conditions reduced the chance that other factors could have masked a possible effect of RF exposure. Therefore, the probability of a false-negative result is low. Due to technical problems some blood pressure data had to be discarded. However, to avoid bias all data reduction was done without knowing the exposure situation.
A relatively large area around the ear of the participants was exposed to include potential target organs or tissues. The peak SARs, however, were lower than the maximal permissible exposure levels (SAR1 g = 1.6 W/kg (17) and SAR10 g = 2.0 W/kg (18). In consequence, some mobile phones when operating with maximal output power may exceed the exposure level used in this study. The output power depends on various physical factors, among them the distance to the base station. A Swedish study has indicated that when GSM phones are used in cities they operate at the maximal output power only 25% of the time and at the minimal power (∼1% of the maximal) 22% of the time (19). These data, indicating that the exposure levels in real life may sometimes exceed the values given in the present study, are probably relevant also for our study, since almost all participants lived in cities. However, this fact does not invalidate our conclusions, since the subjects in our study frequently had typical symptoms both with and without (sham) RF exposure.
Evidently, symptoms occurring during both the sham and RF exposure must have other causes than RF fields. Previously, factors such as muscle strain by keeping the phone or stress by the calls and/or by the interruption caused by the calls have been suggested as candidates to explain mobile phone-attributed symptoms (2). However, in the present series of trials, these factors were not present in either of the exposure conditions. In addition, the background levels of RF fields were very low and participants did not report having symptoms in the vicinity of sources of low-frequency fields. Therefore, electromagnetic fields from other sources are not the likely reasons for the symptoms.
Remaining possible explanations of the reported symptoms are other unknown physical environmental factors present in the laboratory or psychological factors associated with the tests. The effect of environmental factors would probably have increased with the time spent in the laboratory. Evidence against this explanation is the fact that symptoms were usually more intense during rather than immediately after exposure while the participants still were in the exposure room. A similar argument can be raised against psychological stress caused by the test situation, which would presumably be reduced from the first to the last session due to habituation. However, symptoms were not found to be related to the order of the eight trials. A more likely explanation is that the test situation engenders negative expectations which, in turn, cause the headache and discomfort, i.e. a nocebo effect (20). This effect has previously been investigated in a provocation study with electric and magnetic fields from visual display units by conducting both open and double-blind tests (21). The sham exposures caused significantly fewer symptoms than the real exposures in open tests where the participants were informed about the exposure conditions, but not in the double-blind tests. In the present study, we could not properly study the effect of nocebo since occurrence of symptoms in the open RF trial was an inclusion criterion for the double-blind test and we did not conduct any open trial including sham. However, lacking other plausible explanations, we believe that this is the most likely mechanism in the present study also.
While the present study included only highly selected individuals considered to be particularly sensitive to mobile phones, other provocation studies have included both sensitive individuals and non-sensitive controls (11, 13). The controls reported no symptoms (11) or significantly less intense symptoms during or after the exposure than did the sensitive group (13), but no statistically significant difference was observed between real and sham exposures in either group. Similarly, almost no difference between mobile phone exposures and sham exposures was seen in two experiments with non-sensitive subjects only (22). In these tests some symptoms increased, but only slightly, during the exposures. Since the controls never had attributed headache or other symptoms to mobile phone use, most of them presumably did not expect to be affected by the exposure in the test situation, which would eliminate or at least reduce the nocebo effect. For individuals who attribute symptoms to mobile phone use, however, the nocebo effect is probably an important cause of the pain and discomfort in the head, not only in test situations but also in everyday life in connection with the use of the mobile phone.
Conclusion
In this study we included a highly selected group of individuals who frequently experienced headache and other discomfort when using their mobile phone, but not when near to or using sources of low-frequency fields. All experienced typical symptoms during an open provocation with RF exposure. However, the results of the double-blind provocation tests did not give any evidence that RF fields from GSM mobile phones were the cause, and there was also no effect of RF exposure on heart rate or systolic or diastolic blood pressure. The most likely explanation for our results is that the symptoms are due to negative expectations, i.e. a nocebo effect.
Acknowledgements
The National Institute for Working Life, Umeå by Kjell Hansson Mild generously lent us the exposure equipment. The project ‘Electromagnetic fields and biological effect’ which included the present study was supported by The Research Council of Norway (project 146523/310), Norwegian Post and Telecommunication Authority, Statnett, Telenor, Norsk tele- og informasjonsbrukerforening (NORTIB), Netcom.