
Abstract
This study, which is a part of the initiative 'Lifting The Burden: The Global Campaign to Reduce the Burden of Headache Worldwide', assesses and presents all existing evidence of the world prevalence and burden of headache disorders. Population-based studies applying International Headache Society criteria for migraine and tension-type headache, and also studies on headache in general and 'chronic daily headache', have been included. Globally, the percentages of the adult population with an active headache disorder are 46% for headache in general, 11% for migraine, 42% for tension-type headache and 3% for chronic daily headache. Our calculations indicate that the disability attributable to tension-type headache is larger worldwide than that due to migraine. On the World Health Organization's ranking of causes of disability, this would bring headache disorders into the 10 most disabling conditions for the two genders, and into the five most disabling for women.
Introduction
Headache is one of the most common disorders of the nervous system and several of its subtypes—tension-type headache, migraine, cluster headache and the so-called chronic daily headache syndromes—cause substantial levels of disability. Yet, throughout the world, headache has been and continues to be underestimated in scope and scale, and headache disorders remain under-recognized and under-treated everywhere.
In recognition of this global problem, the three major international headache non-governmental organizations, in collaboration with the World Health Organization (WHO), have committed to the initiative ‘Lifting The Burden: The Global Campaign to Reduce the Burden of Headache Worldwide’ (LTB campaign) (1). An important part of this work is to obtain a ‘clear and objective understanding of the scale and scope of headache-related burden’, which means bringing out all existing evidence of the burden of headache worldwide, translating prevalence and incidence data into disability data.
The worldwide epidemiology of headache disorders is only partly documented. Many studies have been performed on migraine, but data on tension-type headache (TTH), the most frequent, are relatively sparse. In addition, most epidemiological studies hitherto have been performed in countries in Western Europe and North America. The aims of this study were to provide a definitive update on what is known of the prevalence of headache and its most common subtypes worldwide and to extract population-based data needed to estimate the world's headache burden.
Methods
Case definitions
The Headache Classification Committee of the International Headache Society (IHS) in 1988 provided the first International Classification of Headache Disorders (ICHD-1) with relatively specific and unequivocal definitions of the various headaches (2). This classification was later incorporated into the International Classification of Diseases (ICD-10) (3). The ICHD-1 was revised in 2004 (ICHD-2) (4), but only minor changes were made with respect to the definitions of the most prevalent headache types.
In the present survey, we included population-based epidemiological studies that appeared after 1988 on migraine (ICD-10 diagnosis G43) and TTH (G44.2), the two types that affect the great majority of headache patients. We did not distinguish between migraine with (G43.1) and without (G43.0) aura, since this differentiation might be difficult in epidemiological studies and because the two types are probably not very different with regard to disability. In order to encompass all headache, we also included epidemiological studies that investigated headache in general, or headache not otherwise specified. In this case, since the term ‘headache’ is not defined in the ICHD-1 or -2, we included studies on headache prevalence that appeared before 1988. For TTH, the term ‘chronic’ is applied to the subtype occurring in patients on ≥15 days per month for ≥3 months (2). In many headache studies, a similar usage of this term has been adopted irrespective of whether the headache was of the tension type or not. We gathered data on ‘chronic daily headache’ (CDH) (i.e. any headache occurring on ≥15 days per month, or ‘daily’ headache) to assess the prevalence of this group of disorders, since patients affected by these are probably those most incapacitated by headache.
Literature search and data extraction
A comprehensive literature search identifying population-based studies of headache and migraine was conducted. Empirical studies published in English were identified through Medline using the search words ‘headache epidemiology’ or ‘migraine epidemiology’ or ‘headache prevalence’ or ‘migraine prevalence’. References listed in relevant publications were also examined.
All articles were first screened for various aspects of methodology and design, and type of content, in order to enable us to select studies of interest for our purpose (Table 1). Partly, it was also done to build up a resource database for later studies in connection with the LTB campaign. For the present study, we extracted the country of origin, year of publication, population characteristics, method of data collection and the prevalence estimates for headache, migraine, TTH and chronic headache, both overall and for each gender, and for various age categories, in addition to data on headache frequency, duration and intensity.
Variables considered in screening of studies
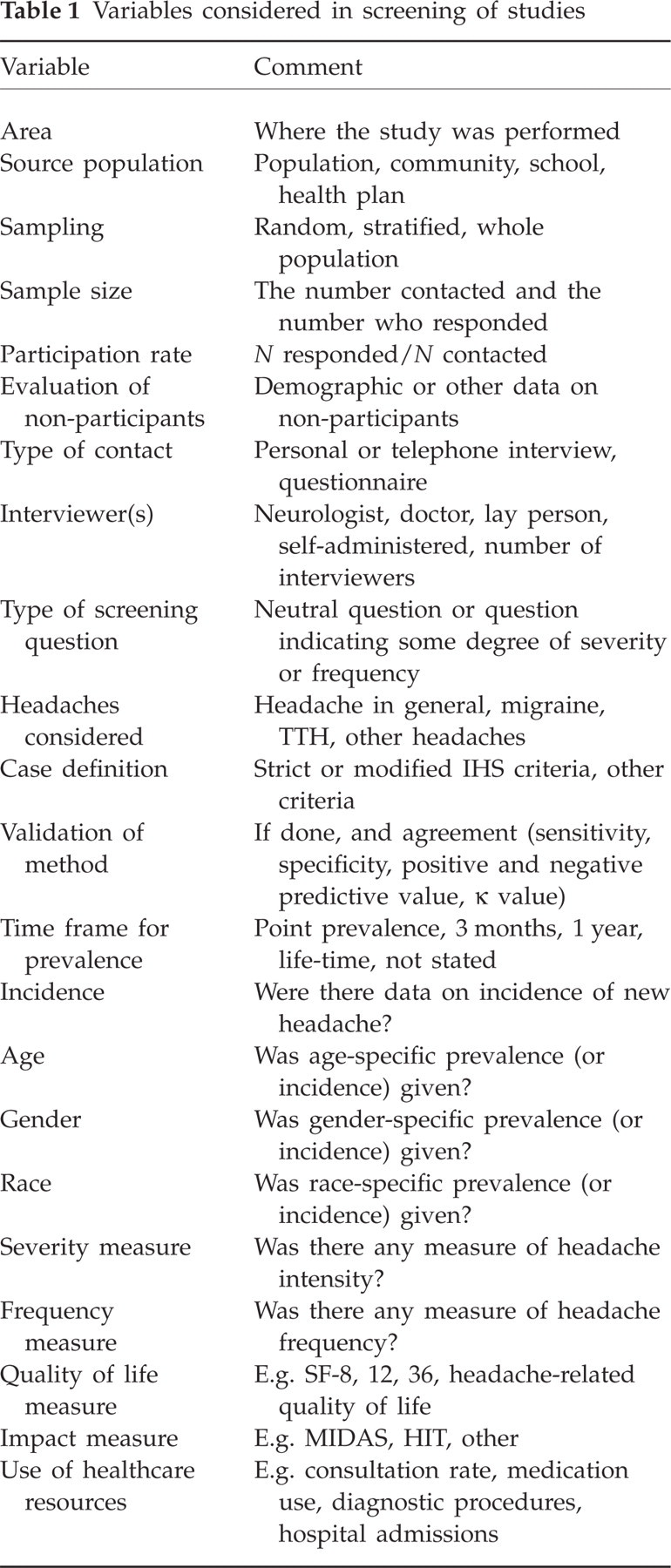
As to the source population, we included only studies performed on the whole population or a representative sample of the whole population within a certain age range in a community, town or country. Accordingly, we did not include studies based on selected populations (clinic-based, in workplaces, among university students, etc.). Since school attendance is obligatory in many countries, studies on headache in children and adolescents of school age based on school populations were included.
For most individuals, headache is troublesome only in certain phases of life. For this reason, most headache epidemiological studies have provided 1-year prevalence estimates, i.e. headache occurring during the last year. However, some studies had estimated 3-month prevalences, while a number have given no definite time frame, only asking a question such as ‘Do you have/suffer from headache’. In some of the latter, it was explained that respondents would understand this as a question about complaints in the relatively recent past (e.g. (5)), so we assumed that such questions were answered by respondents having in mind the last 3 months or the last year. Hence, when summarizing the results, 1 year, 3 months and ‘time frame not stated’ were subsumed under one category called ‘current headache’. In other studies, participants were explicitly asked about headache during their whole life (life-time prevalence).
Calculations of disease burden
In an attempt to calculate the disease-related burden among adults with the two main headache types, migraine and TTH, we tried to detect all population-based studies providing data on the frequency, duration and intensity of headache among adult sufferers (i.e. covering at least age groups 25–60 years). As to frequency, some studies provided a figure on the mean or median days with headache per time unit (usually per month or year) per headache sufferer, whereas the majority of studies gave percentages of headache sufferers in different frequency categories (e.g. 1–7 days/month, 8–14 days/month). For the latter type of study, we calculated mean frequencies both by using the minimum figure in each category (e.g. 1 day/month for those having headache on 1–7 days/month) and by taking the mid point (e.g. 4 days/month for those with headache on 1–7 days/month). The number of days per time unit was then multiplied by the percentage of headache sufferers in each frequency category, and the figures for all frequency categories were summed. All mean frequencies were than recalculated as number of days per year and this figure was further multiplied by the population prevalence of the headache type in this particular study to obtain the number of days with headache (migraine or TTH) per year per person in the population.
Intensity was mostly registered on a scale of 0–3 (0, no headache; 1, mild; 2, moderate; 3, severe headache) and mostly as percentages of sufferers in each category. For a few studies using an intensity scale of 0–10, results were recalculated on a 0–3 scale. For studies using a scale of 0–4, the latter representing ‘excruciating headache’, intensities 3 and 4 were recoded as category 3. The mean intensity was calculated by multiplying each intensity degree by the percentage of sufferers reporting that degree, and then summing these products.
The main interest of our study was to estimate the headache-related disease burden, which implies some level of disability. Using intensity as a proxy for disability, a headache intensity of 1 (‘mild headache’ on the scale 0–3) was set as the zero point, since mild headache on this scale is usually considered to imply little or no disability. Thus, headache intensities 1–3 on this scale were equated with disability on a scale of 0–2.
Results
A total of 107 publications relevant to the present project were identified, eight from Africa, 20 from Asia, four from Australia/Oceania, 48 from Europe, 14 from North America and 13 from Central/South America. In Table 2, prevalence data on headache, migraine, TTH and CDH are listed, together with the main aspects of the method employed. Studies for each continent including adults of all ages are presented first, then studies restricted to children or adolescents (<20 years) and then studies on the elderly (>60 years). Some studies reporting both life-time and 1-year prevalences are listed twice in order to present both datasets. In studies giving prevalence data only for each gender, the total prevalence was computed as the mean of the two.
Headache epidemiological studies





N.s., Not stated; L.t., Life-time; P.i., Personal interview; T.i., Telephone interview; Q, Questionnaire.
With regard to the method of data acquisition, personal interview, telephone interview and self-administered questionnaires were used. The distinction between these methods is not always as straightforward as it may seem. Questionnaires filled in by interviewers were coded as ‘personal interview’, whereas questionnaires completed by the respondents were coded as ‘questionnaires’ even if research personnel were present during the completion of the forms. Furthermore, some studies used questionnaires to screen the population and screen-positive subjects were then subjected to personal or telephone interviews to confirm headache diagnoses. These were also coded as ‘questionnaire studies’, since the sensitivity of the method was dependent on the questionnaire part of the study.
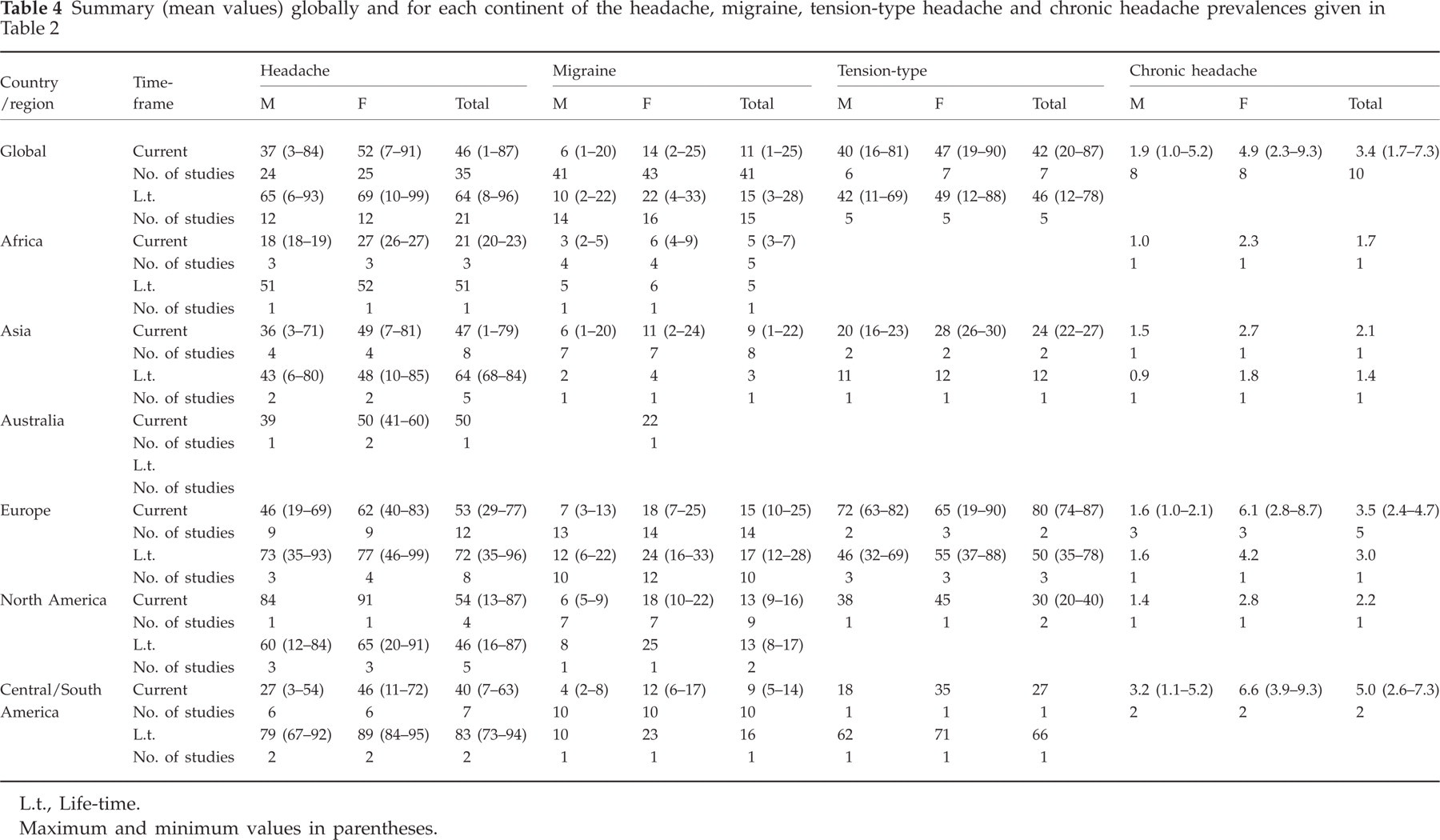
Table 3 summarizes the results for different age groups (adults or all age groups, children/adolescents and elderly) and Table 4 the results for each continent, among adults only, for current headache and for life-time headache. The figures for both genders (‘Total’ in these tables) do not always lie between those for males and females, since a number of studies give prevalence figures only for the whole population. The means of all studies were calculated without correction for numbers in each study since, generally, the mean in each study was extrapolated to the larger population that had been sampled. In this way, we found the global prevalence of current headache to be 47%, current migraine 10%, current TTH 38% and current CDH 3%. Considering studies restricted to adults gave similar results (46%, 11%, 42% and 3%). We found life-time prevalences, as expected, to be somewhat higher: 66% for headache, 14% for migraine, 46% for TTH. For CDH, however, the lower life-time prevalence of 2.9% was based on only two studies. Summary data on prevalences related to the various age groups are shown in Fig. 1. Migraine is most prevalent among adults, whereas CDH is less prevalent among children and adolescents. It seems inconsistent that headache in general is most prevalent in the youngest age group whereas TTH, which should outweigh other headaches, is most prevalent in adults. This inconsistency is probably due to the fact that few studies exist for TTH among children.

Prevalence of different headaches in different age categories. TTH, Tension-type headache; CDH, chronic daily headache.
Summary (mean values) for different age groups of the headache, migraine, tension-type headache and chronic headache prevalences given in Table 2

L.t., Life-time.
Maximum and minimum values in parentheses.
Summary (mean values) globally and for each continent of the headache, migraine, tension-type headache and chronic headache prevalences given in Table 2
L.t., Life-time.
Maximum and minimum values in parentheses.
Figures 2–4 compare the prevalences for the different diagnostic categories across the continents. The prevalence of headache in general (Fig. 2) is close to 50% in Asia, Australia, Europe and North America, but markedly lower (20%) in Africa. Migraine (Fig. 3) is most prevalent in Europe (15%) and least prevalent in Africa (5%). TTH (Fig. 4) appears to be much more common in Europe (80%) than in Asia or the Americas (20–30%) (data from Africa and Australia/Oceania are lacking). Data on CDH are relatively scarce and therefore probably less reliable, but we found a global prevalence of 3.4%. This condition appears to be most common in Central/South America (5%) and least common in Africa (1.7%).
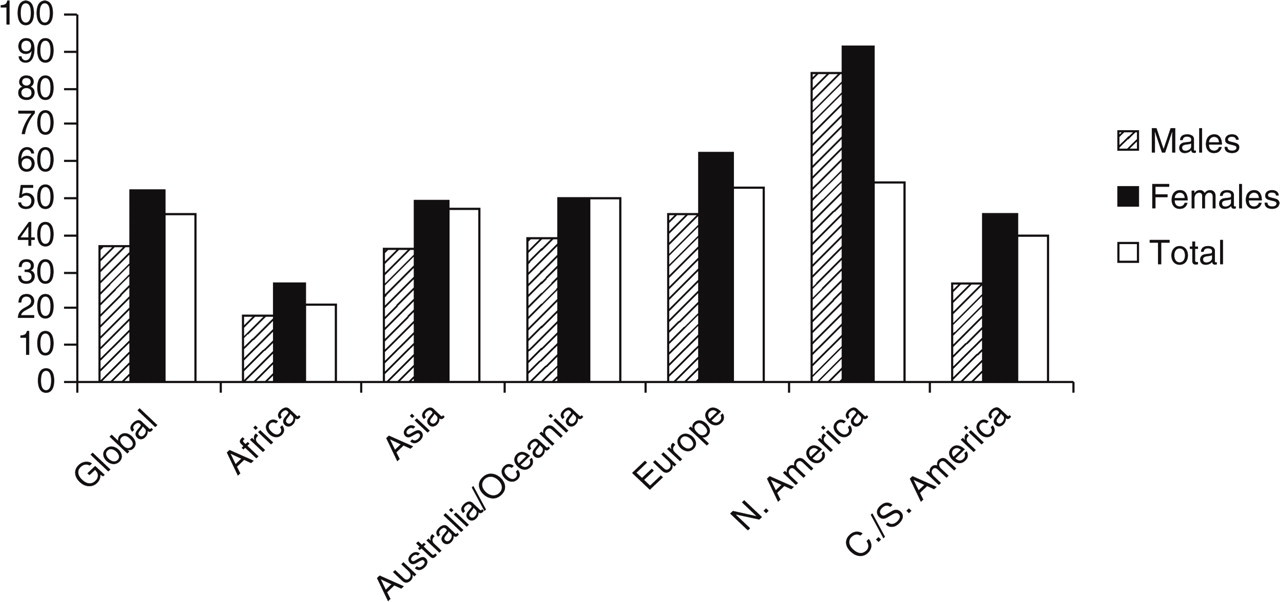
Prevalence of current headache in adults for the different continents. The fact that, for example in N. America, prevalence of Total headache does not lie between that of males and females is due to the much lower number of studies reporting prevalence figures for each gender than for both genders.

Prevalence of current migraine in adults for the different ontinents.

Prevalence of current tension-type headache in adults for the different continents.
Medication-overuse headache (MOH), a potentially treatable and preventable headache type, is common among those with CDH. Possible MOH was found to occur in about 1% of the adult population in countries as different as Norway (6), Spain (7, 8) and Taiwan (9) and in close to 0.5% of adolescents in Norway (10) and Taiwan (11). In epidemiological studies it is not possible to ascertain whether all cases are really MOH since, for certain diagnosis, improvement within 2 months after discontinuation of medication is required.
For the severe but rarer headache types there are few properly population-based studies based on IHS criteria, and those that exist provide only life-time prevalences. For cluster headache, a study from San Marino found a life-time prevalence of 0.06% (12), whereas recent studies from Italy (13) and Norway (14), with presumably higher sensitivity, indicated prevalences as high as 0.2–0.3%. No good studies exist outside Europe.
The data used in disease burden calculations (see Methods) are presented in Table 5. Using intensity as a proxy for disability, we found global mean disabilities of 1.4 for migraine (i.e. 70%) and 0.6 for TTH (30%). The results displayed in Fig. 5 are based on burden calculations using this disability measure multiplied by the headache frequency (headache days per person in the population). In this formula we omitted duration because these figures vary considerably (Table 5) and are hard to interpret since some studies reported the usual duration of headache with treatment, others without treatment, and many studies did not give information on whether it concerned treated or untreated attacks. It appears that the burden of migraine is relatively evenly distributed across those continents where we have sufficient data to perform this calculation, whereas the results for TTH are much more variable. Taking the total headache burden to be the sum of the burdens of migraine and of TTH, we found TTH contributed 58% of it and migraine 42%. When duration was also included in the formula (figures not shown), TTH contributed 53% of the total burden and migraine 47%. For all other ways to calculate the relative burdens of migraine and TTH (using minimum frequency estimates and/or using the original intensity scale of 0–3), TTH was found to contribute >58% of the total burden.

Burden of headache (headache days/year per person in the population × intensity).
Frequency, duration and intensity of headache

Discussion
This review amply documents that headache is a major health problem on all continents. The global prevalence among adults of current migraine is >10%, of current TTH around 40%, and of current CDH 3%. Although TTH is generally less burdensome than migraine to the individual sufferer, the total societal burden of this headache type seems to be even larger than that of migraine because of its much higher prevalence.
Since a principal object was to bring out all population-based studies on the most prevalent headache types, we have been quite liberal when including different studies, in spite of great variations in size, methodology and quality. How methodological differences may influence results have been thoroughly discussed in connection with a similar undertaking on headache epidemiology and health economy in Europe (15). In a previous meta-analysis of headache epidemiological studies worldwide, the relative contribution to variations in the results of variations in methodology (compared with variations in age, gender distribution, race and continent) has been estimated at around 30% (16). In the present study, we have mostly taken the results at their face value and disregarded variations in methodology when summing the results, although we have distinguished between life-time and current headache prevalences and between very broad age categories when presenting the results. The reason for this is that there are so many differences in methodology between the included studies that it may be impossible to control for them all, particularly since the method in many of the studies is very incompletely described. Some prevalence figures based on very few studies may be less reliable. As an example, the prevalence of current headache among men and women in North America seems to be much higher than in the other continents (Table 4, Fig. 2), but these figures are based on only one study. With regard to total current headache, however, which is based on four studies, the prevalence in North America is not much higher than the global mean.
In order to estimate disease burden, the percentage of the population with active disease (i.e. current headache) is more relevant than life-time prevalences, which are also less reliable because of recall problems. Furthermore, for the burden calculations, we have used only those studies that cover a wide age range, including the most productive years (at least 25–60 years). The burden of migraine has been assessed previously using the Disability-Adjusted Life Year (DALY), which is the burden measure favoured by WHO (17). This compound measure is the sum of Years of Life Lost to premature mortality (YLL) and Years Lived with Disability (YLD). The latter is calculated by the formula (Incidence × Duration × Disease Weight] (18). The disease weights for various disorders assigned by WHO place severe migraine in the highest category (0.7–1.0 on a scale from 0.0 to 1.0) (19). However, no weight has been assigned by WHO for TTH. Our calculations, which assigned to migraine a disability of 70% (i.e. 0.7 on a scale of 0.0–1.0), accords very well with WHO's disease weighting, and this lends credibility to our calculation of 30% (i.e. 0.30) disability for TTH.
We have tried to calculate the relative disease burdens of migraine and TTH by using similar formulas [Headache days/year/person in the population × (Duration of headache episodes) × Headache intensity]. The data on duration were considered to be relatively unreliable. However, all our calculations, using various combinations of these variables in our formula, and even omitting duration in the formula, gave the result that TTH caused a greater burden than migraine in the population. Furthermore, our assumption that the intensity measure can be used as a proxy for disability weight may seem unwarranted. However, in a carefully conducted study using different validated measures of both headache intensity and disability, it has previously been shown that there is a robust relation between these two parameters (20). The relation was present also for the milder headache intensities, but admittedly, it was investigated only among migraine sufferers. Hence, our use of pain intensity as a proxy for disability among TTH patients may seem speculative, but our conclusion, that TTH causes at least as much disability as migraine, is supported by population-based studies on work absence due to headache. One study from the USA demonstrated that both chronic and episodic TTH cause a high number of workdays lost (21) and in one study from Europe the number of workdays lost due to TTH was three times higher than that lost due to migraine (22). Therefore, the YLD for all headache is almost certainly at least twice that of migraine. Although other headache disorders such as cluster headache undoubtedly impose a great burden on individual patients, the total societal burden of this and other severe but relatively rare headaches is probably quite small compared with that of the common headache types. WHO ranks migraine 19th in all causes of disability, and 12th in women, based on YLD (23). Doubling the YLD would bring headache disorders collectively into the 10 most disabling conditions overall, and into the five most disabling for women.
Although one can conclude that the burden of headache is large on all continents, headache prevalence and burden are poorly described in large and populous regions. No studies exist in the former USSR countries, including Russia, and there are relatively few studies from elsewhere in Eastern Europe, from Australia/Oceania or from Africa. In India, a good headache epidemiological study has been performed only among adolescents; a study on adults concerned all neuroepidemiology and provided data only on headache in general. In China, studies on adults have been performed only in Hong Kong, which may not be very typical of the rest of the country. Hence, at least half of the world's population lives in countries where headache prevalence and burden are not or only very incompletely known.
Possibly, headache burden varies considerably between different parts of the world, owing to differences in genetic background, climatic and socioeconomic conditions, life-style, other disease spectrum and general health. Although the studies published until now suggest important differences with regard to headache prevalence, it is hard to evaluate how much of the variation is due to differences in method or to cultural attitudes related to the reporting of headache complaints between different studies. It is a priority to start new studies in those parts of the world that are poorly described. Before this is done, in order to enable meaningful comparisons of studies performed in different settings, we strongly recommend that some common standards for how to perform these studies are established.
Acknowledgements
This study was part of, and supported by, ‘Lifting The Burden: The Global Campaign to Reduce the Burden of Headache Worldwide’. Lifting The Burden is a formal collaboration between the World Health Organization, World Headache Alliance, International Headache Society and European Headache Federation.