
Abstract
The four-point pain scale (none, mild, moderate, severe) and the 11-point pain scale (0 = no pain, 10 = pain as bad as it could be) have been used in migraine studies to assess treatment efficacy. The primary objective of this study was to investigate the validity and responsiveness of the 11-point pain scale using the four-point pain scale as a benchmark. Using data from 95 migraine patients recruited from headache clinics, this study found that 11-point pain scale scores were highly correlated with four-point pain scores. The correlations between the pain scales were significantly higher than the correlations with quality of life measures such as functional ability and emotional feelings. The 11-point pain scale was 55% more sensitive than the four-point pain scale in detecting clinically important differences. The strong linear relationship between the two pain scales allowed researchers to transform four-point pain scores to 11-point pain scores using regression weights.
Introduction
Although pain is a multidimensional phenomenon, the severity of migraine headache is usually characterized by pain intensity, frequency, duration and disability. In clinical trials, the effectiveness of treatment is often based on subject ratings of migraine pain intensity before and after treatment. Essentially, all triptan medications approved in the United States of America (USA) are based on evaluations of clinical efficacy using the four-point pain scale that asks subjects to indicate if their pain is none, mild, moderate and severe. Pain-free response, defined as a rating of no pain at 2 h or 4 h after treatment, is generally accepted as a stringent and desirable endpoint in migraine clinical trials (1). Despite the fact that the four-point pain scale is the most widely used method of measuring pain severity in the migraine literature, the 11-point numeric rating scale (where the patient is asked to choose one number from 0 to 10 that best reflects the intensity of their pain) is commonly used in research of other pain syndromes (2, 3). Recently, there is an interest in using the 11-point pain scale in migraine research. For example, the Chronic Pain Index (4, 5) and the Migraine Disability Assessment (MIDAS) Questionnaire (6) include an 11-point numeric rating scale for assessing headache pain intensity.
The primary objective of this study was to evaluate the validity of the 11-point scale by assessing its correlation and sensitivity as compared with the four-point pain scale in migraine pain measurement. Although the 11-point pain scale is commonly used in other chronic pain syndromes, the validity of the 11-point pain scale in patients suffering from episodic and self-limiting headache pain has not been evaluated. During the past decade, seven triptans in different formulations have been approved in the USA. Yet comparative-data on the effectiveness of these migraine medications remain limited. This study compared the sensitivity of the four-point and 11-point pain scales. Such information will facilitate the choice of a sensitive pain scale that can detect clinically meaningful treatment differences for clinical trials and inform evidence-based clinical decisions. The secondary objective of this paper was to develop an algorithm that allows the conversion of 11-point pain scale scores to four-point pain scale scores. A simple algorithm will be useful to researchers interested in comparing pain scores measured using the two different pain scales in different studies, and facilitate the conduct of meta-analysis of migraine studies in the future.
Methods
Study procedures
This prospective survey study was conducted at two specialized headache centres, one in Ohio and another in North Carolina, USA. Study subjects were at least 18 years old, willing to give informed consent to participate in this study, had been diagnosed with migraine with or without aura according to the International Headache Society (IHS) criteria 1.1 and 1.2 (7), had at least a 1-year history of migraine attacks, and were able to distinguish migraine attacks from other headache types. Subjects with tension-type headaches occurring on 15 or more days per month, or subjects who had cluster headache were excluded from the study. A total of 179 subjects participated in the study. Subjects who agreed to participate were asked to complete a study questionnaire at the time of study enrolment, and complete another questionnaire during the next migraine attack outside of the study clinic. Subjects were asked to return the second questionnaire by mail to study clinics in a preaddressed prepaid envelope. The clinic staff reviewed the returned questionnaires to ensure their completeness before sending them to researchers at Ohio State University for data entry and analysis. The study protocol was reviewed and approved by the Institutional Review Board.
Measures
During study enrolment visits, subjects completed a questionnaire with questions on subject demographics, headache frequency, current migraine pain rated on a four-point and 11-point pain scale, a rating of how pain affected ability to function (normal, mildly impaired, severely impaired, bed-rest required) and a rating of how pain affected emotions (none, mildly, moderately, quite a bit, extremely). The purpose of the in-clinic study enrolment questionnaire was to allow researchers to train patients regarding the proper completion of the questionnaire to minimize errors on the questionnaire completed outside of the study clinic. With the exceptions of subject demographics, data collected at the study enrolment visit were not used for data analysis.
During the next migraine attack, subjects completed a questionnaire with items on (i) the date and time of attack; (ii) pain ratings on an 11-point pain scale before treatment, and at 2 h and 4 h after treatment; (iii) pain ratings on a four-point pain scale before treatment, and at 2 h and 4 h after treatment; (iv) ratings of how pain affected ability to function before treatment, and at 2 h and 4 h after treatment; (v) ratings of how pain affected emotions before treatment, and at 2 h and 4 h after treatment; (vi) drug treatment(s) and/or any non-pharmacological treatment used for migraine within the first 4 h of migraine pain; (vii) whether migraine condition improved, remained the same or deteriorated at 4 h after receiving migraine treatment; (viii) how much had migraine condition improved or deteriorated (slightly, moderately, greatly); and (ix) time until meaningful relief of migraine pain. Migraine treatments used by study subjects were at the discretion of study investigators and study subjects. No specific medications were required by the study protocol. In order to minimize possible bias that may result from the ordering of the four-point and 11-point pain ratings on subject responses, two formats of subject questionnaires, one with the four-point pain scale preceding the 11-point pain scale and another with the 11-point pain scale preceding the four-point pain scale, were randomly assigned to study subjects.
Data analysis
In testing validity, it is important to examine relationships between variables that should occur (i.e. evidence of convergent validity) and relationships that should not occur (i.e. evidence of discriminant validity). Specifically, we adopted the approach proposed by Campbell and Fisk in 1959 (8) and developed a correlation matrix of correlations among the pain scales, ratings of how much pain affected ability to function, and ratings of how much pain affected emotions. Because all four scales in the study questionnaire were completed using self-administration, the correlation matrix used in this study was essentially an estimation of a multitrait-monomethod matrix. Convergent and discriminant validity between the four-point and 11-point pain scales were determined by examining the correlations between the pain scales and their correlations with other measures. Because both the four-point and 11-point pain scales measure a similar phenomenon (i.e. pain), it was expected that the correlations between these two pain scales would be significant and higher than individual pain scales' correlations with ratings on how much pain affected ability to function and how much pain affected emotions. The multitrait-monomethod correlation matrix as described above was developed for data collected before treatment, and at 2 h and 4 h after treatment, to test these hypotheses.
While convergent and discriminant validity are important to demonstrate the usefulness of an instrument for cross-sectional assessment, responsiveness (or sensitivity) is an important characteristic for instruments used for measuring changes over time. The method proposed by Guyatt in 1989 was used to assess responsiveness (9). Mean change-from-baseline pain scores for subjects who reported migraine condition had improved/deteriorated were compared with those who reported migraine condition had remained the same at 4 h after treatment to determine how statistical differences corroborate clinically meaningful differences. It was expected that the change-from-baseline score for subjects who reported an improvement or deterioration would be greater than those who reported no change. In addition, effect sizes of the magnitude of change, calculated by dividing the change-from-baseline scores for subjects who reported their migraine condition had improved/deteriorated at 4 h after treatment by the standard deviation of the baseline score for those who reported their migraine condition as remaining the same at 4 h after treatment, were compared between the four-point and 11-point pain scales to determine which scale was more sensitive in detecting clinically important differences. To develop an algorithm that would facilitate the comparison of 11-point pain scale scores with four-point pain scale scores, 11-point pain scale scores before treatment, and at 2 h and 4 h after treatment, were regressed on corresponding four-point pain scale scores using random effects generalized least squares estimation while controlling for age, gender, migraine frequency, and whether pain rating is before or after treatment. All statistical analyses were performed using Statistical Analysis Software Version 9.1 (SAS Institute, Cary, NC). All tests were performed at α = 0.05.
Results
A total of 179 subjects (114 from Ohio and 65 from North Carolina) completed study questionnaires during enrolment visits. Of these, only 110 subjects (59 from Ohio and 51 from North Carolina) returned the questionnaire for their next migraine attack to study clinics. Fifteen subjects had incomplete data on study questionnaires and they were excluded from data analysis. Data analysis was performed on the final sample of 95 subjects (50 from Ohio, 45 from North Carolina). Mean age of subjects was 44.5 years (standard deviation = 10.1 years, median = 45 years) and 94% of subjects were female. All subjects had high school education or above. On average, subjects experienced about one migraine headache (
To examine the presence of bias due to ordering of pain scales in the study questionnaire, the mean scores of the four-point pain scale and the 11-point pain scale for subjects receiving different formats of study questionnaires were compared. The mean scores for the four-point and 11-point pain scales between subjects receiving different formats of study questionnaire were similar and not significantly different (Table 1). Therefore, ordering biases were considered unlikely.
Comparison of mean pain scores for subjects completing questionnaires of different formats
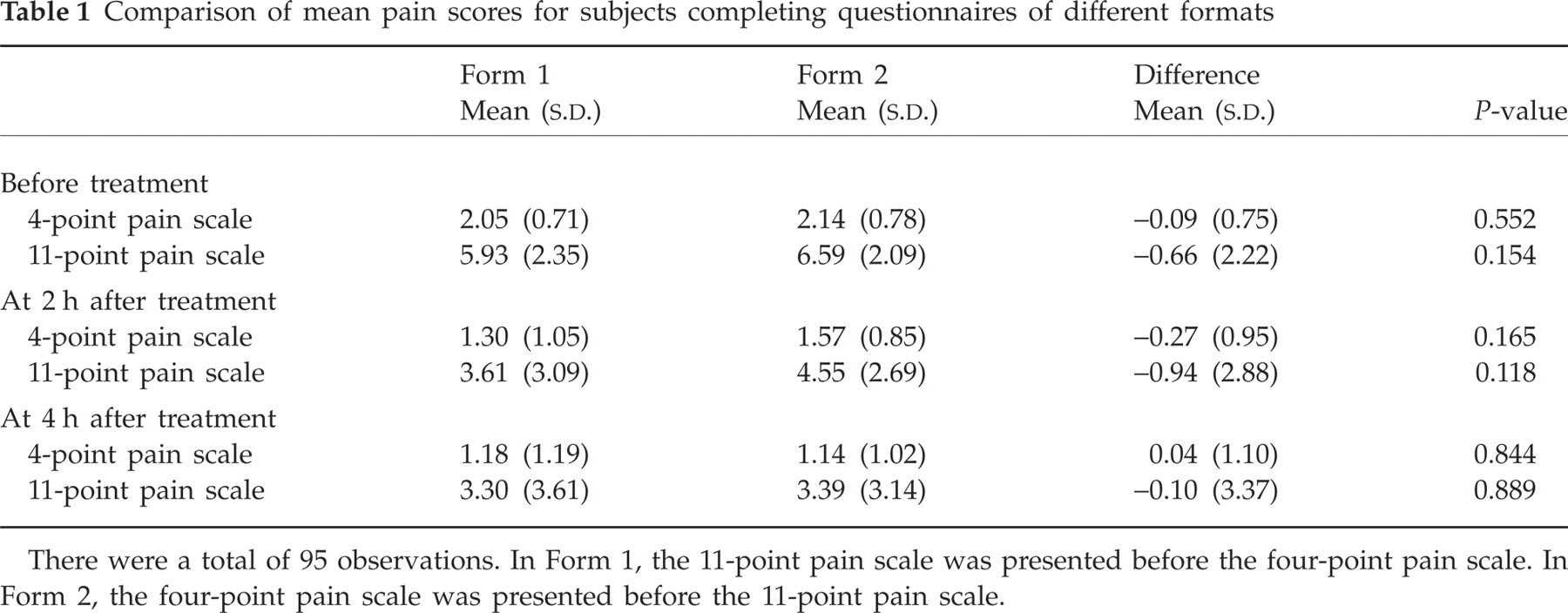
There were a total of 95 observations. In Form 1, the 11-point pain scale was presented before the four-point pain scale. In Form 2, the four-point pain scale was presented before the 11-point pain scale.
Correlation matrices of the four-point pain scales, 11-point pain scales, and ratings of how much pain affected ability to function and emotion are presented in Table 2. The correlations between the two pain scales were 0.75 before treatment, 0.89 at 2 h after treatment, and 0.94 at 4 h after treatment. Each of these correlations was significant at the 0.01 level. The magnitude and statistical significance of these correlations supported the convergent validity of the 11-point pain scale. In addition, correlations between the two pain scales and their correlations with ratings on how much pain affected ability to function and how much pain affected emotions were compared. For all assessment time points, correlations between the two pain scales were statistically significantly greater than the correlations between individual pain scale and ratings on how much pain affected ability to function and emotions at the 0.05 level (Table 3). These results provided evidence of discriminant validity for the 11-point pain scale in measuring migraine headache pain. Because the four-point pain scale was operationalized as four ordered categories (none, mild, moderate and severe), and the 11-point pain scale was operationalized as 0 (no pain) to 10 (pain as bad as it could be), the analyses were repeated using nonparametric Kendall's t correlation instead of Pearson correlations. Results based on Kendall's t were very similar to those based on Pearson correlations.
Pearson correlations of pain scales and ratings of how much pain affected ability to function and emotions

P < 0.01 for H0 : ρ = 0.
One-tailed t statistics for the comparison of correlations between pain scales and ratings of how much pain affected ability to function and emotions

There were a total of 95 observations; standard error σz = 0.104, 1.96σ = 0.204.
Significant at 0.05 level.
To test the responsiveness of both pain scales, the change-from-baseline pain scores for subjects who reported their migraine condition as improved or deteriorated were compared with those who reported their migraine condition as remained the same at 4 h after migraine treatment. For both pain scales, the change-from-baseline pain score for subjects in the ‘improved/deteriorated’ group was significantly higher than those in the ‘remained the same’ group, indicating that both scales were responsive in detecting clinically meaningful difference (Table 4). The effect sizes for the four-point pain scale and 11-point pain scale were 1.13 and 1.75, respectively. The ratio of these effect sizes was 1.55. This ratio can be viewed as a measure of relative responsiveness (RR) of the two scales in terms of effects size, indicating that the 11-point pain scale was 55% more responsiveness than the four-point pain scale in measuring migraine headache pain intensity.
Effect size comparison of the four-point and 11-point pain scales

Effect size was calculated as: Change-from-baseline score for subjects reporting that their migraine condition had improved/deteriorated at 4 h after treatment divided by the standard deviation of baseline score for subjects who reported that their migraine condition remained the same at 4 h after treatment.
The results of the regression analysis of 11-point and four-point pain scores are presented in Table 5. The model variables explained over 80% of the variances of the 11-point pain scores. As expected, four-point pain scale score was a significant predictor of 11-point pain scale score. Eleven-point pain scale score was not significantly affected by subject age, gender or migraine frequency after the four-point pain scale score was accounted for. However, the magnitude of 11-point pain score was significantly affected by the time of assessment. On average, 11-point pain scale score was equivalent to about 2.7 times four-point pain score. Eleven-point pain rating converted from four-point pain score that was assessed at 2 h or 4 h after treatment on average was 0.5 points lower than the rating that was assessed before treatment.
Random effects generalized least squares estimation of eleven-point pain scale scores

There were a total of 267 observations from 89 subjects.
Significant at 0.01 level.
Significant at 0.001 level.
Discussion
This study has several notable findings. First, the results of this study showed that the 11-point pain scale is valid in measuring the severity of migraine headache pain. The 11-point and four-point pain scales were almost a linear transformation of each other. Both of them are pure measures of pain intensity that are distinct from quality of life measures such as the impact of pain on ability to function and emotions. Secondly, the significant linear relationship between the four-point pain scale and 11-point pain scale provides a simple method for researchers to convert pain scores from one scale to another scale using regression weights. Although the algorithm was not sensitive to subject age, gender and migraine frequency, a downward adjustment of 0.5 was needed when converting four-point pain scores that were measured after treatment. Thirdly, the results showed that the 11-point pain scale was 55% more responsive than the four-point pain scale. A more responsive pain scale may ferret out levels of differences between existing migraine medications that were not detected in previous studies. Hence, the 11-point pain scale provides a useful alternative to the four-point pain scale for measuring treatment differences in active comparator studies.
While this study focused on the validity and sensitivity of measures of pain intensity, it is important to note that pain intensity rating is limited in representing patients' pain experience. The detrimental economic and financial consequences of migraine for the patient and his/her family are well recognized (10–14). Despite the fact that post-treatment change in pain intensity ratings has been the standard method in evaluating treatment efficacy in migraine clinical trials, previous studies indicated that ratings of pain relief are more sensitive than pain intensity rating change scores in evaluating the effects of analgesics (15–17). Also, it has been shown that other treatment benefits that are beyond pain intensity, such as speed of onset, lack of associated symptoms, and lack of adverse events are important outcomes desired by migraine patients (18, 19). Previous studies also showed that correlations between pain scores and quality of life were moderate, suggesting that pain scores are limited in demonstrating the effects of treatment and the burden of migraine from the patient's perspective (20). Hence, while substituting the four-point pain scale with the 11-point pain scale may improve sensitivity in measuring pain intensity, future research should supplement pain scales with multi-attribute measures, such as disability and quality of life scales, to assess treatment outcomes more comprehensively.
The results of this study should be viewed in the context of its limitations. First, only 53% of subjects enrolled in this study returned questionnaires with adequate data for analysis. The low response rate is probably due to lack of incentive to complete the study. Subjects were not offered any monetary compensation, nor did they receive free study medications for participating in the study. It is unclear whether subjects returning study questionnaires were different from those who did not. Therefore, subject selection bias cannot be ruled out. Secondly, subjects were asked to rate their pain at appropriate time points (before treatment, 2 h after treatment, 4 h after treatment) during their next migraine attack outside of the study clinic. It is unclear whether patients have followed instructions to record their pain ratings at the exact time intervals. Completion of items after the migraine attack was over may introduce recall bias to subject responses. Thirdly, because subjects in this study were trained to complete the two pain scales, it is possible that they had rated their headache pain using the two pain scales together prior to recording their scores in the study questionnaires. This might have biased the correlation between the 11-point and four-point pain scales upwards, and limit the generalizability of study findings in comparing pain scores of the two scales across studies in which patients did not use the two scales simultaneously in rating their headache pain. Notwithstanding these possible limitations, the strong correlations between the 11-point and four-point pain scales observed in this study increased our confidence that the validity of the 11-point pain scale was not random. The inclusion of subjects taking various types of pharmacological and non-pharmacological treatment of migraine rather than a single medication increased the generalizability of study results. Future research is encouraged to utilize the two pain scales together to further evaluate their sensitivity in detecting changes in a clinical trial setting.
Acknowledgements
This study was supported by GlaxoSmithKline. The results of this study were previously presented at the American Neurological Association Neurology Outcomes Research: Current Science and Future Directions Meeting, Chicago, 30 September 2001. Appreciation is expressed to Dr Alice S. Batenhorst and Dr David W. Miller for their assistance in the initial design of this study and Dr Glen D. Solomon and Dr John Rubino for their assistance in patient recruitment.