
Abstract
Objective
To evaluate the psychometric characteristics of a previously validated electronic headache diary with automated algorithm for the purpose of identifying migraine days.
Methods
The psychometric properties of 13 variables in this e-diary were analyzed using item response theory (IRT) in migraine patients from the Leiden Headache Center. The included items were headache presence, duration, unilaterality, severity, pulsating, aggravation by physical activity, visual aura, aura duration, nausea, vomiting, photophobia or phonophobia and triptan usage. The added value to the end-diagnosis of an already validated migraine day of the individual items was assessed. A generalized partial credit model was used to evaluate the items. A discriminative value α ≥ 1.70 indicated an excellent discrimination.
Results
In total 1418 migraine patients were analyzed with a mean age of 43 years, 89% were women and 38% reported aura symptomatology. All items demonstrated excellent discriminative value [α: 1.82–54.1], except for aura duration [α:0.86], which was moderate. Cronbach's alpha was 0.91. The answers options of headache duration, photophobia, phonophobia, nausea and vomiting did not reach the probability threshold of 0.5.
Conclusions
The items in this e-headache diary demonstrated good overall psychometric performance, although certain items, particularly aura-related and multi-categorical items, may benefit from category merging or further refinement.
This is a visual representation of the abstract.
Introduction
Healthcare providers diagnose migraine and monitor treatment in migraine based on what patients report about their headaches and associated symptoms. The need for daily monitoring stems from the episodic nature of migraine, which leads to recall bias. A daily e-diary helps to accurately evaluate both the frequency and duration of attacks, as well as the characteristic symptoms accompanying them.1–3 Patients tend to underestimate their attack frequency when reporting <8 days per month and overestimate them when reporting >8 days per month. 1 Moreover, with the emergence of the new treatments targeting calcitonin gene-related peptide (CGRP) or its receptor, many countries require fulfillment of specific criteria for reimbursement, which often includes a certain decline in monthly migraine days.4,5 With increasing technological possibilities, numerous digital diary tools, primarily in the form of smartphone applications, are now accessible to patients with migraine.6,7 Unfortunately, most of these applications rely on self-reported migraine days (a person only indicates a day as a migraine day yes/no) and there is limited or no evidence regarding the validity of these electronic diaries (e-diaries).6,8–14 Although a migraine diagnosis is typically made by a medical professional, these e-diaries are self-reported by patients. This underscores the importance of assessing whether the items included in these e-diaries measure what they are intended to measure and evaluating their reliability and precision. In addition, the e-diaries are used to monitor the severity of migraine symptoms over time, which takes all symptoms into consideration and not just a dichotomous value of whether a day classifies as a migraine day or not.
To our knowledge, there are only two validated e-diaries available that use an algorithm to classify a day as non-headache day, headache day or migraine day rather than relying solely on self-report.1,15 There are limited data regarding the psychometric properties, such as adequacy, relevance, validity, and reliability of electronic diaries utilized for monitoring migraine. This information may be helpful as it shows whether the diaries are posing the appropriate inquiries. Item response theory (IRT) analyses may be helpful to improve a daily detailed questionnaire by assessing whether it is measuring the trait accurately, by identifying most informative items, and by assessing whether multiple choices for assessing severity of symptomatology are useful. This approach may help reduce the number of questions or answer categories. Items with insufficient sensitivity or specificity may be identified, requiring clinical interviews for confirmation.16,17 Simplifying e-questionnaires makes them more suitable for patients with less complex needs, such as those treated by general practitioners, and more accessible to individuals with limited health or digital literacy. By contrast, IRT may also show that additional items may be needed if fit indices show poor model performance or specific clinical needs are unmet.
In the present study, we aimed to evaluate the psychometric properties of a previous validated headache e-diary that is used at the Leiden Headache Center.1,2,18,19 The IRT analyses may offer more insight into the reliability and validity of the individual items included in the e-diary that is used for daily migraine monitoring, by estimating the information function of each item and combined items as a whole, and may provide information on how to improve or shorten the incorporated items and response options.
Methods
Design
To evaluate the psychometric properties of the Leiden Headache Center e-diary, we used e-headache diary data, collected between October 2018 and April 2022 from patients diagnosed with migraine at the Leiden Headache Center.1,20 Ethical consideration for this study was obtained from the Medical Ethical committee of the Leiden University Medical Center (METC: NL41600.058.12, Biobank: BB23.003), who identified no ethical concerns. Therefore, patients did not have to provide additional informed consent. All data were fully anonymized before analysis.
Patient population
All individuals aged ≥18 years with a confirmed migraine diagnosis were invited to complete a daily headache e-diary. The migraine diagnosis was verified by a neurology resident or a researcher with expertise in headaches, in consultation with a neurologist specialized in headache (GMT and NP). We also included patients who screened positively for a migraine diagnosis using two validated questionnaires and algorithms based on the International Classification of Headache Disorders, 3rd edition (ICHD-3) criteria.1,2,18 In previous studies from the Leiden Headache Center focusing on treatment efficacy or analyses involving repeated measurements with the headache e-diary, an 80% adherence rate was required for inclusion. However, because the present study examines the psychometric properties of the e-diary, all patients were included regardless of their adherence level to ensure that the evaluation reflects a representative clinical sample. For this psychometric analysis, we randomly selected one day in the follow up of each patient who stared an e-diary. This approach accounted for variations in follow-up duration across patients, ensuring a balanced assessment of the e-diary's psychometric properties.
Measurements
Patients were monitored with a daily e-diary during their treatment or research study participation at the Leiden Headache Center. Patients received a daily alert to complete the headache e-diary, which included 3–13 questions, depending on whether a headache, visual aura symptoms or acute medication use were reported. These questions covered detailed characteristics of the headache and associated symptoms (unilaterality, pulsating, moderate to severe pain, aggravation by physical activity, phonophobia, photophobia, nausea, vomiting). If a visual aura was experienced, additional questions captured its characteristics and duration. The diary also tracked the use of acute medication (both migraine-specific and non-migraine specific).1,20,21 The time required to complete the e-diary was approximately 1–3 minutes per day depending on whether it was a non-headache or headache day.
An automatic algorithm processed all data entries and classified each day either as a non-headache day, a headache day or a migraine day. A migraine day was defined as: (1) a typical migraine headache, defined by the presence of at least two of the following characteristics: unilateral pain, pulsating, moderate-to-severe pain, aggravation by physical activity, accompanied by at least one associated symptom such as phonophobia and photophobia, and/or nausea or vomiting, with a duration of ≥30 minutes; (2) the intake of triptan, regardless of effective triptan response, because patients may use triptans when the headache is still mild; or (3) the presence of visual aura symptoms lasting 5–60 minutes.1,2 The outcome assessed in this study is migraine severity of a day, defined by the number and intensity of migraine-associated symptoms reported by patients. It is important to indicate that severity is not defined by the number of monthly migraine days.
Notably, at the time of data collection for this study, only triptans were prescribed in clinical practice in the Netherlands. Therefore, in the present study, migraine days were defined solely based on triptan use and did not account for other acute medication treatments such as gepants, ergotamines or ditans.
Statistical analysis
Baseline characteristics were summarized using the mean ± SD, or medians with interquartile ranges (IQR), as appropriate. The primary analysis included a random selection of a data-entry per patient, and thus included both headache and non-headache days. A sensitivity analysis was performed, in a sample including a headache and non-headache day per patient, because it was expected that the primary analysis included more non-headache days than headache days.
The psychometric properties of the 13 variables (items) included in the e-diary were investigated with IRT, which refers to a family of mathematical models attempting to explain the relationship between the migraine severity and the items included in the e-diary.16,17 IRT focuses on the discrimination capacity of the included items, and it indicates where an item falls on the continuum scale of migraine severity. Migraine severity was defined as the number and intensity of migraine-associated symptoms This provides information on how well an item discriminates between different levels of migraine severity. We verified several key assumptions, including invariance, one-dimensionality, monotonicity and local independence to ensure that variations in responses were attributable to variation in the latent trait itself.16,17 First, invariance was addressed with a test information curve between females versus males and between individuals from the outpatient clinic and from previous research participation. Second, one-dimensionality was addressed with an exploratory and bifactor model, to examine whether a secondary latent trait existed. Third, monotonicity was assessed with the ‘mokken’ package, version 3.1.2 (https://cran.r-project.org/web/packages/mokken). Fourth, local independence was assessed with Yen's Q3. 22
Participants were classified based on their complete follow-up data. Chronic migraine was defined as ≥15 headache days and ≥8 migraine days per month. High frequent episodic migraine was defined as ≥8 monthly migraine days, whereas low frequent episodic migraine was <8 monthly migraine days. Medication overuse headache was defined as ≥15 days usage of over-the-counter analgesic use or ≥10 days of migraine-specific medication (triptans/lasmiditan) per month.
The items analyzed with IRT need to be categorical. For that reason the headache duration, a continuous item, was grouped into 0 minutes, <30 minutes, 30 min to 4 hours, >4 hours.
IRT model interpretation
The items included in the e-diary consist of seven dichotomous items and six ordinal items. Therefore, a generalized partial credit IRT model was used to analyze both item types. The analysis included evaluation of the strength of the relationship between items and migraine severity. It also evaluated the thresholds between response categories, which indicate the severity levels at which the probability of choosing one response over the next increases. Thresholds are the point at which a person has a 50% probability of selecting a higher response category over the next lower one, and in IRT should ideally exceed a 0.5 probability for items with multiple response options. Additionally, these response options should be sequential on the scale of migraine severity. Each response option should have a distinct peak without overlapping with the curve of another item, reflecting a specific range of severity where that response is most likely to be chosen. Ordinal response options that indicate more severe symptoms should have higher thresholds (b-values). This means that the plotlines should be more to the left on the x-axis, which corresponds with a higher migraine severity. For instance, pain intensity is scored on a four-point scale, with three thresholds: one between each pair of adjacent categories (e.g. between absent and mild, mild and moderate, etc.) The discrimination values are categorized as follows: ≥1.70 indicates excellent discrimination, 1.35–1.69 indicates good discrimination (little to no revision required), 0.65–1.34 indicates moderate discrimination (little to no revision required), 0.35–0.64 indicates marginal discrimination (revision required) and ≤0.34 indicates poor discrimination (revision or elimination necessary). 23 The Akaike information criteria (AIC) of the IRT models and the Cronbach's alpha of all the items were reported.
For the primary and sensitivity analyses, a test information curve (TIC) was plotted stratified by sex, to illustrate the precision of the test across different migraine severity for males and females separately. The TIC shows how much reliability the test provides at different levels of migraine severity. The higher the curve, the more precise the measurement at that level of migraine severity.
The recommended sample size for IRT analyses is n = 1000 patients. 24 The IRT analysis was used for scale construction and evaluation, and was conducted using the package ‘MIRT’, version 1.38.1 (https://cran.r-project.org/web/packages/mirt) for R statistical software (R, version 4.2.1; R Foundation for Statistical Computing, Vienna, Austria, 2016; URL: https://www.R-project.org).
Results
In the first sample, 1418 patients were included, of whom 67% visited the outpatient clinic and 33% participated in research. The mean age among the patients was 43 years, 89% were females and 38% were diagnosed with migraine with aura. The median follow-up time of the patients was 185 days (IQR = 105–587) with a median compliance of 98% (IQR = 90–100) (Table 1).
Baseline characteristics.

aCompliance is calculated as number of data entries divided by days of follow-up.
IQR = interquartile range.
The random sample of the 1418 patients that was taken over their entire follow-up period included 549 (39%) headache days, 357 (25%) migraine days and 47 (3%) aura days (Table 2). Based on their e-diary data, of the participants from the outpatient clinic 26% fulfilled the diagnosis chronic migraine, 25% high frequent episodic migraine and 50% low frequent episodic migraine, and 29% of the outpatient participants fulfilled the diagnosis medication overuse headache. For the research participants 6% fulfilled the diagnosis chronic migraine, 9% high frequent episodic migraine and 85% low frequent episodic migraine, and 18% met the criteria for medication overuse headache.
Classification of E-diary entries included in the primary analysis of 1418 patients.
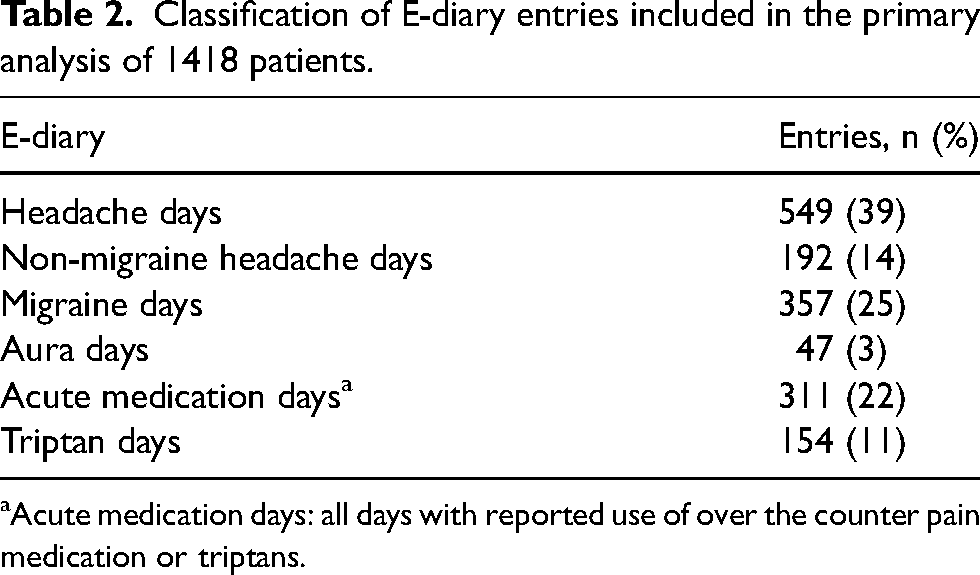
aAcute medication days: all days with reported use of over the counter pain medication or triptans.
Item characteristic curves (ICCs) were plotted per item to visualize how the e-diary items performed in differentiating between individuals across various levels of migraine severity (Figure 1). All items, except for aura duration, demonstrated excellent discriminative value, with alpha values ranging from 1.82 to 54.1. The aura duration item, showed moderate discriminative value, with an alpha of 0.86.

Item characteristics curves (ICC) for items assessing migraine severity, with a generalized partial credit model (GPCM). The horizontal x-axis represents the latent trait: migraine severity on a scale of −2 to +2 SDs. Higher values of x indicate more severe symptoms. The vertical y-axis represents the probability of endorsing specific response categories for a given level of migraine severity. The colors of the lines in the graph represent categorical response options. A single line represents a dichotomous item, while multiple-colored lines represent polytomous categories. The discrimination of each item is represented by the ‘a’-value and the slope, with higher values indicating better discriminative ability. The crossing point between two answer category represent the threshold: ‘b’-value(s). *Discrimination is classified as follows: low: 0.35–0.64, moderate: 0.65–1.34, good: 1.35–1.69, excellent >1.7.
The threshold values of all binary items were excellent and the items met the assumption of monotonicity (see supplementary material, Table S1). For the items severity, phonophobia and photophobia, the multiple response categories showed a sequential order. However, only the response categories of severity reached the 0.5 probability threshold. For the items headache duration, aura duration, nausea and vomiting, the response categories showed a non-sequential order, and did not reach the 0.5 probability threshold. Sequential thresholds are indicative of well-functioning items because they imply a consistent progression through the response options. This is illustrated in Figure 2, which shows where the threshold values, b1 to b3, can be located on the x-axis.

The threshold values (b1–b3) indicate the points on the x-axis (latent trait or severity level) where the probability of selecting one response category becomes equal to the probability of selecting the next higher category. The dotted lines mark these threshold values, showing that they are sequential, which confirms that this item allows one to differentiate clearly among patients between the response categories. The peaks of each response category curve exceed the probability threshold of 0.5, suggesting that patients with this level of migraine severity are more likely than not (more than 0.5) to choose this response category. This response category is preferred at that level of migraine severity.
Figure 2 also shows that each response option has its own peak, without overlapping with the line of another response options.
The test information curve has its peak around 0.5 on migraine severity, where zero mean represents the average level of migraine in this sample (where only 25% of the 1418 measurements where on a migraine day), and more than zero corresponds with and increased migraine severity (Figure 3(a)). When we included both a headache day and a non-headache day for each patient, the peak shifted to the left around 0.2, indicating that the test provides greater precision at slightly lower levels of migraine severity when considering both types of days, because now 50% of measurements where on a migraine day (Figure 3(b)). There was no difference between males and females because the plots largely overlapped. The test information curve of individuals who participated in previous research projects was slightly shifted towards the right compared to those from the outpatient clinic, suggesting a difference in the underlying trait distribution with lower severity in outpatients versus research participants, but no difference on measurement properties. The e-diary optimum for precision and information is mainly on the area of the latent trait that differentiates between migraine and non-migraine day. The AIC of the model was 11801, and Cronbach's alpha for the included items is 0.91.

Test information curves (a) primary analysis (b) sensitivity analysis, including a headache and non-headache day per patient. Both plots are stratified by sex.
Sensitivity analysis
The sensitivity analysis included a headache and a non-headache day of each patient. The ICC values of this sample are shown in Figure 4. The results of the ICC are similar to those of the primary analysis. The test information curve of the sensitivity analysis slightly shifted towards the left. The bifactor analysis indicated that the items visual aura and aura duration were strongly associated with a distinct underlying dimension (latent factor) separate from migraine severity (a2 = 25.56 and 8.35, respectively), whereas other headache-related items primarily loaded on the general factor, daily migraine severity (see supplementary material, Table S2). The multidimensional IRT model fitted significantly better to the data than the unidimensional IRT model. Yen's Q analysis revealed the highest correlation between visual aura and aura duration (0.82), followed by increase by physical activity and pulsating quality (0.28), and nausea and vomiting (0.17). The remaining items exhibit lower or negative correlations (see supplementary material, Table S3).

Sensitivity analysis: Item characteristics curves (ICC) with a sample including a headache and non-headache day per patient.
Discussion
The psychometric properties of the e-diary used at the Leiden Headache Center were evaluated using IRT in a sample of individuals with migraine from our outpatient clinic and research database. Overall, the e-diary items performed excellently, with the exception of two aura-related items. The IRT analysis demonstrated the reliability and measurement precision of the E-diary, further strengthening its validity as a psychometrically sound tool for assessing migraine severity.
To our knowledge, this is the first study to report the psychometric properties of a validated, algorithm-based headache e-diary. Existing e-diaries vary widely in their design, particularly among algorithm-based versions. For example, our algorithm incorporates triptan intake regardless of effective triptan response, aiming to minimize under0reporting. 2 Additionally, aura-related items in many other e-diaries are typically based on self-report and are not integrated into the algorithm. These differences, along with the limited availability of psychometric evaluation – especially regarding discrimination and the information density of individual questions and response categories – present challenges for direct comparison. Most existing headache e-diaries rely on self-reported migraine and headache days, yet their psychometric properties remain largely unexplored. Evaluating the psychometric aspects of these e-diaries, such as the validity of their questions and response categories, would be highly valuable. The present study offers unique insights of a robust psychometric validation and may guide the development of future headache e-diaries enhancing their use in monitoring migraine.
The strong performance of our e-diary items aligns with expectations because we already validated the questions in a previous study and made a proposal for the definition of a migraine day. 2 However, as we expected, the aura-related items showed lower discriminative value and factor loadings, indicating a weaker association with migraine severity. The findings suggest another underlying dimension (distinct latent trait) separate from migraine severity, for aura-related symptoms, as demonstrated by their strong specific factor loadings in the bifactor model. These findings align with the migraine with aura subgroup, separate but related to the migraine without aura subgroup in the ICHD-3 criteria. 25 It might be appropriate to address aura symptoms separately.
In previous studies, we have already shown that our e-diary effectively achieves its primary goal of distinguishing migraine days from non-migrainous headache days.2,26 In the present study, which focuses on the psychometric properties of this e-diary to access migraine severity, we found that all binary items performed excellently, whereas, for the items with multiple response categories, only the item on pain severity proved informative. The validation of this e-diary has been published elsewhere.1,2 Other items with multiple options, such as headache duration, photophobia, phonophobia, nausea and vomiting, showed lower utility because the response options in this E-diary showed little discriminative power. For these items, the response categories did not reach the 0.5 probability thresholds, which means that this response category was never the most probable choice for that level of migraine severity. These categories are therefore more neutral or less strongly endorsed categories, which is often reported in items with many response categories. This is in line with the ICHD-3 criteria for migraine diagnosis, which evaluate only the prevalence and not the severity of the characteristics: photophobia, phonophobia, nausea and vomiting. 25 The limited value of these items should be weighed against the desire to monitor severity of symptoms at the outpatient clinic, and the burden for patients to complete the diary on a daily basis.
Therefore, merging these answer categories into a binary format (presence/absence) may shorten the e-diary and may improve clarity and accessibility. For example, with binary outcome one may consider adding visual indicators (e.g. green and red buttons), which may enhance usability for individuals with limited literacy. With these simplifications the e-diary might become a valuable tool for remote tracking of migraine symptoms and supporting timely interventions, thereby facilitating remote care, which lessens the burden for patients and physicians and aids in delivering high quality care when medical resources are scarce for instance in underserved countries. However, these potential simplifications are only suggestions and require further evaluation in future research to determine whether they improve the psychometric properties of the e-diary.
Interestingly, research participants reported greater daily migraine severity, as defined by the number and/or intensity of migraine associated symptoms, compared to outpatient clinic participants. By contrast, as expected, outpatient clinic participants more frequently experiences chronic or high-frequent episodic migraine and medication overuse headache. The higher daily migraine severity among research participants may reflect the fact that patients at our outpatient clinic received appropriate acute and preventive care, whereas research participants were not under clinical care of our research center.
Similarly, test information curves of the sample including a headache and non-headache day per participant provided information on a lower latent trait, which might be explained by the larger inclusion of non-headache days.
The psychometric analysis of the Leiden Headache Center e-diary has several strengths. Including data from both research participants and outpatient clinic patients, regardless of their e-diary adherence level, enhances generalizability of the findings. The large sample size and the inclusion of sensitivity analysis further strengthen the reliability of the results. 23 Additionally, selecting a single day per patient from their follow-up period ensured a robust estimation of the psychometric properties, avoiding any imbalance caused by variations in follow-up duration. The assessment of psychometric properties strengthens the e-diary's existing validation.1,2 Our findings underscore the potential for digital monitoring in headache care because the e-diary reliably monitors migraine frequency and characteristics, suggesting that aspects of headache care may be effectively transferred to digital platforms. Certain limitations may impact generalizability. First, the sample was predominantly female, and selection bias may have occurred because only patients who started an e-diary were included. However, the TICs were largely identical among the sexes. Second, limited data on visual aura prevented reliable psychometric properties of aura-related items. Considering the unique symptomology of migraine with aura, a dedicated IRT analysis focusing on patients with this specific diagnosis might provide further insights, although the question remains if it is not better to have a clinical diagnoses of aura first and instruct patients for the aura questions after that.
The present study has limitations related to the IRT assumptions. First, the assumption of unidimensionality may be challenged by the inclusion of symptoms that are not psychometrically homogenous, due to some conceptual overlap. The bifactor IRT analysis indicated that, although two aura-related items formed a secondary factor, aligning with the clinical experience with this symptom, the remaining items loaded primarily on the general factor representing migraine severity. This supports in part the assumption of unidimensionality for the majority of the items. Second, the assumption of local independence may be violated, particularly among clinically related symptom pairs, such as nausea and vomiting. Additionally, Yen's Q analysis suggested local dependency between the visual aura and aura duration items, as well as potential dependence between physical activity and pulsation items. Such dependencies may lead to inflated discrimination values, although this is a known and often accepted limitation in clinical symptom scales. Although the bifactor model partially accounts for local dependencies, we acknowledge that residual dependence may remain. This limitation is important to consider when interpretating the psychometric output of the model, but they do not undermine the general utility of IRT in evaluating item functioning in clinical instruments. Due to the mix of binary, ordinal and continuous response options in the e-diary, IRT remains a valuable method for gaining insight into its psychometric properties.
Moreover, it is commonly used in the validation of symptom-based scales with similar underlying constructs, such as the validation of the migraine functional impact questionnaire. 27 It has also been successfully applied in the psychometric evaluation of pain measures and depression severity scales, where symptoms co-occurrence is inherent.28–30 The bifactor model showed a better fit to the data, but all variables loaded on the general trait and only the aura related items loaded on a different trait aligning with the clinical experience with this symptom. Second, the sensitivity analysis included withing-person correlated data, however, methods to adequately account for this correlation are not yet available. Because the psychometric properties are identical to the random uncorrelated sample, the influence of the underlying correlation is likely to be limited. The present study aimed to evaluate the psychometric performance of the migraine-related items from the e-diary, and not to create a validated migraine severity scale. Migraine severity was in this study defined by the number and intensity of migraine-associated symptoms, which differs from monthly migraine days or other established migraine or headache scales such as the Migraine Disability Assessment (MIDAS) or the Headache Impact Test (HIT-6).
In conclusion, the items included in the Leiden Headache Center's e-diary demonstrated generally strong psychometric properties in assessing migraine severity, particularly those related to core migraine symptoms. However, aura-related items showed lower values of discrimination parameters and may contribute less to the measurement precision of the underlying severity trait in general migraine populations. Additionally, items with multiple response categories provided limited incremental value and merging some into binary categories may be without substantial loss of information.
Evaluating the psychometric properties of headache e-diaries is crucial for improving their reliability, validity and clinical potential. As digital health tools continue to evolve, the emphasis on comprehensive validation becomes increasingly important, to ensure accuracy, reliability and clinical relevance, aiming to optimize treatment strategies.
Key findings
Psychometric evaluations create insight in the reliability, validity and measure precision of individual items of validated tools or questionnaires.
Strong psychometric performance: The e-headache diary demonstrated good overall discriminative values for migraine characteristics and moderate values for aura-related items.
Supplemental Material
sj-docx-1-cep-10.1177_03331024251359222 - Supplemental material for The psychometric properties of an e-headache diary in migraine
Supplemental material, sj-docx-1-cep-10.1177_03331024251359222 for The psychometric properties of an e-headache diary in migraine by Nancy van Veelen, Nadine Pelzer, Britt W.H. van der Arend, Natasha Waslam, Daphne S. van Casteren, Erik J. Giltay, and Gisela M. Terwindt in Cephalalgia
Supplemental Material
sj-docx-2-cep-10.1177_03331024251359222 - Supplemental material for The psychometric properties of an e-headache diary in migraine
Supplemental material, sj-docx-2-cep-10.1177_03331024251359222 for The psychometric properties of an e-headache diary in migraine by Nancy van Veelen, Nadine Pelzer, Britt W.H. van der Arend, Natasha Waslam, Daphne S. van Casteren, Erik J. Giltay, and Gisela M. Terwindt in Cephalalgia
Supplemental Material
sj-docx-3-cep-10.1177_03331024251359222 - Supplemental material for The psychometric properties of an e-headache diary in migraine
Supplemental material, sj-docx-3-cep-10.1177_03331024251359222 for The psychometric properties of an e-headache diary in migraine by Nancy van Veelen, Nadine Pelzer, Britt W.H. van der Arend, Natasha Waslam, Daphne S. van Casteren, Erik J. Giltay, and Gisela M. Terwindt in Cephalalgia
Supplemental Material
sj-docx-4-cep-10.1177_03331024251359222 - Supplemental material for The psychometric properties of an e-headache diary in migraine
Supplemental material, sj-docx-4-cep-10.1177_03331024251359222 for The psychometric properties of an e-headache diary in migraine by Nancy van Veelen, Nadine Pelzer, Britt W.H. van der Arend, Natasha Waslam, Daphne S. van Casteren, Erik J. Giltay, and Gisela M. Terwindt in Cephalalgia
Supplemental Material
sj-pdf-5-cep-10.1177_03331024251359222 - Supplemental material for The psychometric properties of an e-headache diary in migraine
Supplemental material, sj-pdf-5-cep-10.1177_03331024251359222 for The psychometric properties of an e-headache diary in migraine by Nancy van Veelen, Nadine Pelzer, Britt W.H. van der Arend, Natasha Waslam, Daphne S. van Casteren, Erik J. Giltay, and Gisela M. Terwindt in Cephalalgia
Footnotes
Author contributions
NvV, EG and GMT designed the study. NvV, NP and NW are responsible for drafting the manuscript. NvV and EG are responsible for analyzing the data. GT is the principle investigator and supervised this study. BvdA and DvC provided feedback during drafting the manuscript. All authors read and approved the final version of the manuscript submitted for publication.
Data availability
The data that support the findings of this study are available on reasonable request from the corresponding author. Trial results will be communicated to participants, healthcare professionals, the public and other relevant groups through publication.
Declaration of conflicting interest
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: G. M. Terwindt and N. Pelzer report consultancy support from Abbvie/Allergan, Lilly, Lundbeck, Novartis, Pfizer and Teva, and independent support from the European Community, Dutch Heart Foundation, Dutch Research Council, Dutch Brain Foundation, Dioraphte and the Clayco foundation. N. van Veelen, BMH vd Arend, D. S. van Casteren and E. J. Giltay have no conflicts of interest to report.
Ethical statement
The study is performed in accordance with the Declaration of Helsinki Ethical Principles and Good Clinical Practices and was approved by the local and national ethics committees.
Funding
This study was funded by the Dutch Research Council, ZonMw, project number 10960102310009.
Supplement material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.