
Abstract
A randomized double-controlled trial involving 22 patients with Noonan syndrome (NS) and 22 normal individuals (control group) was carried out to determine the prevalence of migraine in patients with NS. The NS group consisted of 11 males aged 19.55 ± 6.11 years and 11 females aged 18.81 ± 5.47 years. The control group consisted of 11 males aged 19.55 ± 6.6 years and 11 females aged 18.81 ± 5.47 years. Seven NS-group patients reported migraine without aura (MO), and three reported probable MO (PMO). Taken together, these represent a prevalence of migraine in the NS group of 45.5%. Two control-group patients reported MO, a prevalence of 9.09%. The prevalence of migraine was significantly higher in the NS-group patients than in the controls (P < 0.005), suggesting a positive association between NS and migraine. Nevertheless, further studies are needed to confirm our findings.
Introduction
Noonan syndrome (NS) is a congenital disorder characterized by a normal karyotype and clinical features that resemble those of Turner syndrome. The majority of cases described are sporadic, but an autosomal dominant pattern is well established in familial cases. Tartaglia et al. and Jamieson et al. mapped the gene for NS to the long arm of chromosome 12(12q24.1) (1, 2). Mutations in the PTPN 11 gene were found in 50% of individuals with Noonan syndrome studied, and some of these did not have a family history of the disease (1). The incidence of this disorder varies from 1:1000 to 1:2500, and affected patients present multiple and systemic anomalies. The most frequent clinical findings are short stature, craniofacial dimorphisms, hypertelorism, ptosis and downslanting of the palpebral fissures, short or webbed neck, and cardiac anomalies (3). At least one-third of children with NS will have some degree of mental retardation or learning disabilities (4). Although neurological manifestations are said to be rare in this syndrome, recurrent seizures were reported in 13% of patients in one study (5), and cerebrovascular episodes, such as intracranial aneurysm (6, 7), cavernous angioma (8) and Moyamoya disease (9), have been described in some cases (7, 8).
Migraine is a common disabling primary headache disorder that peaks during the third and fourth decades of life. Epidemiological studies have documented a high prevalence of the disorder and shown that its prevalence is influenced by age, gender, race and environmental and socioeconomic status (10). Genetic studies of migraine have followed a number of lines: twin studies; family studies; study of rare genetic migraine variants and, recently, neurotransmitter transport protein or receptor genes; and association studies.
The identification of migraine comorbidities has become a common expedient as comorbidities can be used to improve knowledge of the physiopathology of migraine. After noting a number of index cases of male patients with NS presenting migraine, we decided to determine the prevalence of migraine in NS individuals in a search for a possible relationship between the two conditions.
Materials and methods
Twenty-two individuals from a population of 37 NS sufferers were recruited at the Paediatric Endocrine Outpatient Clinic of the Hospital de Clínicas, Universidade Federal do Paraná, Brazil. Another 22 normal individuals matched for gender and age were recruited from two state schools in Curitiba as normal controls. The controls were healthy and had no previous history of neurological, endocrine, cardiac or pulmonary disease.
All NS patients had been followed-up for at least 1 year. None of the patients had used growth hormone (GH) in the previous 12 months. Only five NS patients were submitted to ancillary investigation, which proved normal. The other NS patients or their relatives were interviewed by telephone mainly because they lived far from the medical centre. All the controls were interviewed face to face. The information about cognitive deficits in NS patients was collected from their families. Failure to characterize the headache features correctly led investigators to use the closest possible diagnosis (IHS 1.6.1 or 2.4) (11).
A questionnaire was applied to both groups, and the presence of headache in the previous 12 months was investigated. Patients with a positive history of headache in the previous year were asked about their premonitory symptoms, intensity of the attacks, duration, frequency, type of pain, lateralization, localization, aggravating factors, associated symptoms and use of analgesics. Family history and other characteristics of the headaches were determined for both groups. The headaches reported were classified according to the International Headache Society Criteria (Second Edition) (11).
The NS group consisted of 11 males aged 19.55 ± 6.6 years and 11 females aged 18.81 ± 5.47 years. The control group consisted of 11 males aged 19.55 ± 6.6 years and 11 females aged 18.81 ± 5.47 years (Table 1). The groups were matched for age and gender distribution.
Gender and age distribution for the Noonan syndrome group and control group

The study was approved by the Human Ethics and Research Committee at the Hospital de Clínicas, Universidade Federal do Paraná, Brazil.
The statistical evaluation was performed using the chi-square tests (chi-square and Fisher's exact test). The level of statistical significance used was P < 0.05.
Results
Headaches were reported by 17 (77.27%) of the 22 NS patients and 15 (68.1%) of the control group (Table 2). For statistical consistency, in our study we considered migraine to include both probable migraine and migraine. Probable migraine without aura is a condition in which a single criterion for the diagnosis of migraine is absent.
Distribution and types of headache for all patients in the Noonan syndrome group and control group (ICHD-2 criteria) (11)

The most common types of headaches in NS patients were migraine and probable migraine (10 patients, 45.4%), and in the control group, tension-type headaches (11 patients, 50%) (Table 2 and Figs 1 and 2). Migraine was reported by the same proportion of females and males in the NS group. Tension-type headaches, however, were reported more frequently by females in the control group (Figure 1).
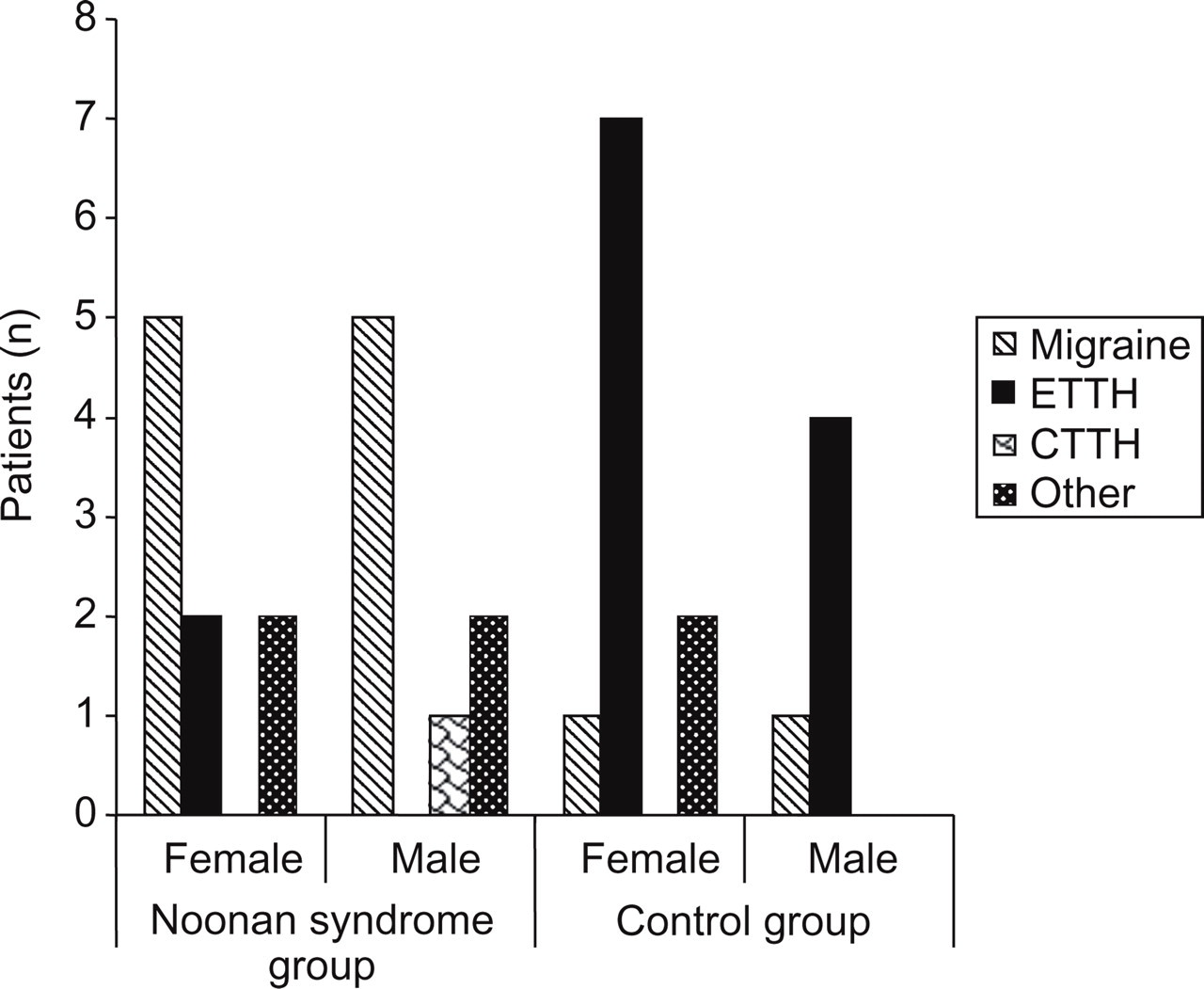
Prevalence of migraine without aura in the Noonan syndrome group and control group by gender. Probable migraine with aura was included with migraine with aura. ETTH, episodic tension-type headache; CTTH, chronic tension-type headache.

Prevalence of migraine∗ and other headaches in the two groups. Probable migraine with aura was included with migraine with aura. ETTH, episodic tension-type headache; CTTH, chronic tension-type headache.
If just those patients with headache are considered, migraine and probable migraine occurred in 58.7% of these patients in the NS group, and tension-type headaches occurred in 73.3% of the corresponding patients in the control group (Table 3 and Figure 2). The distribution of headaches between the groups and genders is shown in Tables 2 and 3.
Distribution and types of headache for those patients with headache in the Noonan syndrome group and control group (ICHD-2 criteria) (11)

Although analysis of all the headaches in the NS group and control group showed the same prevalence of headache in both groups (P = 0.498), individual analysis of headache types showed different results. Migraine and probable migraine together were more prevalent in the NS group than in the control group (P = 0.007), whereas tension-type headaches were more prevalent in the control group than in the NS group (P = 0.010) (Table 2 and Figure 2).
Although we identified headache types other than migraine, probable migraine and tension-type headaches (Tables 2 and 3), we did not carry out a statistical analysis of these because of the small number of cases.
Discussion
Noonan syndrome (NS) is a congenital disorder. A probable gene for NS has been mapped to the long arm of chromosome 12(12q24.1) (2). Mutations in the PTPN11 gene were found in 50% of individuals with NS studied, and some of these patients did not have a family history of the disease (1). PTPN11 was considered the candidate gene for NS because of its location and the protein that it encodes (SHP-2) (12). Studies carried out with 119 individuals with NS to detect mutations in the PTPN11 gene found mutations in 45% of the patients, of whom 49 were familial cases and 70 sporadic. Mutations were found in 45% of the patients and were more frequent in the familial cases (13). Phenotypic features varied, and the most common neurological symptoms were mental retardation (14), intracranial aneurysm (6), cavernous angioma (8) and Moyamoya disease (9). To our knowledge, the prevalence of headache in patients with NS has not been previously described.
Migraine is a common disabling primary headache disorder. Epidemiological studies have documented a high prevalence of this condition, but this may be influenced by age, gender, race and environmental and socioeconomic status (10). Prevalence peaks during the third and fourth decades of life among men and women (10). At this age, prevalence is lower in Asian-Americans (9.2% in women and 4.8% in men), intermediate in African-Americans (16.2% in women and 7.2% in men), and highest in Caucasians (20.4% in women and 8.6% in men) (15). Although the mean age of our patients was lower (19 years), the prevalence of migraine in the NS group was much higher than expected. A longitudinal cohort study of this group may even disclose a more pronounced prevalence of migraine in older patients.
In each of the three patients in this study diagnosed as having PMO in the Noonan group, only a single criterion was not met, mainly because the patients did not report it or did not remember all the features of their migraine headaches. It is important to remember that many of our patients had cognitive impairment and that in several instances information about their headaches was very difficult to obtain. Other family members often had to be asked for further information.
Even excluding NS individuals suffering from probable migraine without aura (PMO), our results showed a high prevalence of migraine without aura (MO) in the NS group compared with the corresponding figure for the control group (9.09%). The difference in prevalence of migraine in the previous year between the control group and the NS group was significant and remained so even when NS patients with PMO were excluded.
As in the literature, recurrent seizures were reported in 13% of patients with NS (5), suggesting that epileptic diathesis may decrease the threshold for cortical spreading depression. This association could explain the high prevalence of MO and probable MO in the NS group, although our patients have no history of epilepsy attacks or cognitive oscillations, and no clinical symptoms that might suggest headache secondary to epilepsy (ICHD-II code 7.6) were observed during the interview.
Craniofacial dysmorphism, which is a common feature in this syndrome, is another abnormality that might also contribute to headache generation. In the second edition of the International Classification of Headache Disorders (ICHD-II), headaches attributed to disorders of the teeth, jaws and temporomandibular joint, as well as to other disorders of the cranium, neck, eyes, ears, nose, sinuses and facial structures, were listed under codes 11.6, 11.7 and 11.8. Headaches attributed to teeth, jaws or related structures (11, 6) were found in only two of our cases (Table 3). We believe that our patients with MO and probable MO were not influenced by craniofacial dysmorphism as these disorders would induce a continuous reduction of the pain threshold, whereas our migraine patients showed manifestations of episodic pain. Clinical investigations also failed to show active disturbances in the jaws or related structures that could justify the pain symptoms in MO and probable MO patients.
One limitation of our study was that we used phone interviews for some Noonan patients. There are a number of difficulties associated with use of the telephone to obtain epidemiological data for patients with migraine, although the method has been used in other studies (16). The telephone is used when information cannot be obtained face to face because of the distance between the patient's place of residence and the investigating medical centre, as was the case in our study because of the locations involved. Telephone interviews were only carried out for those patients who had been examined in our medical centre and all of whose data had been recorded on their medical charts. The aim of the telephone interview was to obtain more precise information about headaches in order to classify them according to the International Headache Society criteria (second version).
Our results suggest a positive association between Noonan syndrome and migraine, but further studies are needed to confirm this. Such confirmation may lead to the search for other migraine genes in chromosome 12. The reason for the failure to detect migraine with aura in our NS group could not be determined from our results alone, which may have been affected by cognitive influence or the lower age of our patients.