
Abstract
It has been previously shown from our laboratory that abnormal functioning of Na/K ATPase can cause spreading depression, the likely mechanism of migraine aura. We used lymphocytes to investigate whether or not membrane Na/K ATPase is altered in migraine with aura patients. Lymphocytes were prepared from such patients, aged 20-45 years, and from age-matched healthy volunteers (controls). The binding of 3H- ouabain was studied using increasing concentrations (0.5-25 nM) of this radioligand, specific for Na/K-ATPase. We studied 19 migraine with aura patients and 22 healthy volunteers, matched for age and sex. Bmax (fmol/mg protein) and KD (nM) were not different between patients and controls. However, their ratio (Bmax/KD) was higher in patients than in controls. Bmax was (mean ± SD) 270 ± 110 fmol/mg protein in controls, and 360 ± 230 in migraine with aura patients (P = 0.10, t-test). KD was (mean ± SD) 2.8 ± 1.5 nM in controls, and 2.9 ± 3.2 nM in migraine with aura patients (P = 0.88, t-test). Bmax/KD was (mean ± SD) 120 ± 78 in controls, and 210 ± 190 in migraine patients (P = 0.046, t-test). Moreover, no control patient had a Bmax/KD ratio greater than 398, while three migraine patients had ratios of 417, 572 and 722, respectively. Ouabain binding is affected by Na/K ATPase structure (KD) and expression (Bmax). While these parameters were not altered in migraine with aura patients, the difference in their ratio suggests an imbalance between the enzyme's ouabain affinity and its expression, with higher-affinity subtypes being more expressed than normal. Moreover, single patients had values quite different from the control population. Our data suggest that (i) ouabain binding to lymphocyte membranes may be a useful tool in the diagnosis of migraine with aura and (ii) Na/K ATPase abnormalities may be involved in migraine aura.
Introduction
The aura of migraine is commonly thought to be due to a wave of spreading depression (1, 2). The latter is a spreading depolarization of the cerebral cortex (3) that can be due to a number of causes (4). One of us, and others, has shown that functional inactivation of Na/K ATPase is sufficient to reliably reproduce a spreading depression-like depolarization (5). A mutation of this enzyme has been associated with familial hemiplegic migraine, a rare form of migraine characterized by transient neurological deficits (6). Although this specific mutation has not been found in an unselected sample of patients with migraine (7), the possibility exists that malfunctioning of Na/K ATPase (whether caused by this mutation or by other mechanisms) is indeed involved in the pathogenesis of migraine aura. If that was the case, such a malfunctioning could be detected by changes in the binding of ouabain to the enzyme. Therefore, we investigated ouabain binding to membranes prepared from circulating lymphocytes from controls and from migraine with aura patients, to investigate whether or not changes in the binding parameters could be detected in the patients' population. As age affects Na/K ATPase (8, 9), we limited our investigation to young adults, defined as 20–45 years old.
Materials and methods
Patients' selection. Outpatients aged 20–45 years old who met the diagnostic criteria for migraine with aura according to the International Headache Society [10] were enrolled. Healthy volunteers of the same age range were used as controls.
Preparation of lymph cells. Peripheral blood (PB) samples were diluted 1 : 1 in D-PBS (Dulbecco's phosphate buffered saline w/o Calcium/Magnesium Euroclone) containing 1% autologous serum and enriched for mononuclear cells (MNC) by centrifugation on Ficoll-Paque (Biochrom KG, Berlin, Germany). MNC were collected and washed twice using the same solution (D-PBS + 1% autologous serum). Then, MNC were incubated for 45 min at 37°C in a humified 5% CO2 atmosphere in D-PBS + 10% autologous serum to discard adherent cells. Non-adherent cells were collected and counted.
Ouabain binding. Lymphocytes were recovered as a pellet by centrifugation, resuspended in K+-free Krebs buffer (125 m

where B represents the specific binding, C the ligand concentration, KD the dissociation equilibrium constant and Bmax the density of ouabain binding sites. Specific binding data were normalized by protein content evaluated by the Lowry method.
Statistical analysis was carried out using the software Prism®, version 4.03, by GraphPad Software Inc., San Diego, CA, USA.
Results
1. Characteristics of the experimental groups
We investigated 22 controls and 19 migraine with aura patients. The patients' age was (mean ± SD) 31 ± 6 and the controls' age 34 ± 7 years (not significant difference, t-test). In the patients group there were eight males and 11 females; in the controls group the corresponding numbers were 8 and 14 (not a significant difference, Fisher's exact test).
In the migraine with aura group, duration of disease was 14 ± 10 years (mean ± SD, range 1–31 years). Frequency of attacks was 12 ± 11 attacks per year (mean ± SD, range 1–36). Duration of aura was 26 ± 20 min (mean ± SD, range 10–60).
2. Ouabain binding
Figure 1 summarizes ouabain binding parameters in the control and in the migraine with aura groups. Bmax was (mean ± SD) 270 ± 110 fmol/mg protein in controls, and 360 ± 230 in migraine with aura patients (P = 0.10, t-test). KD was (mean ± SD) 2.8 ± 1.5 n
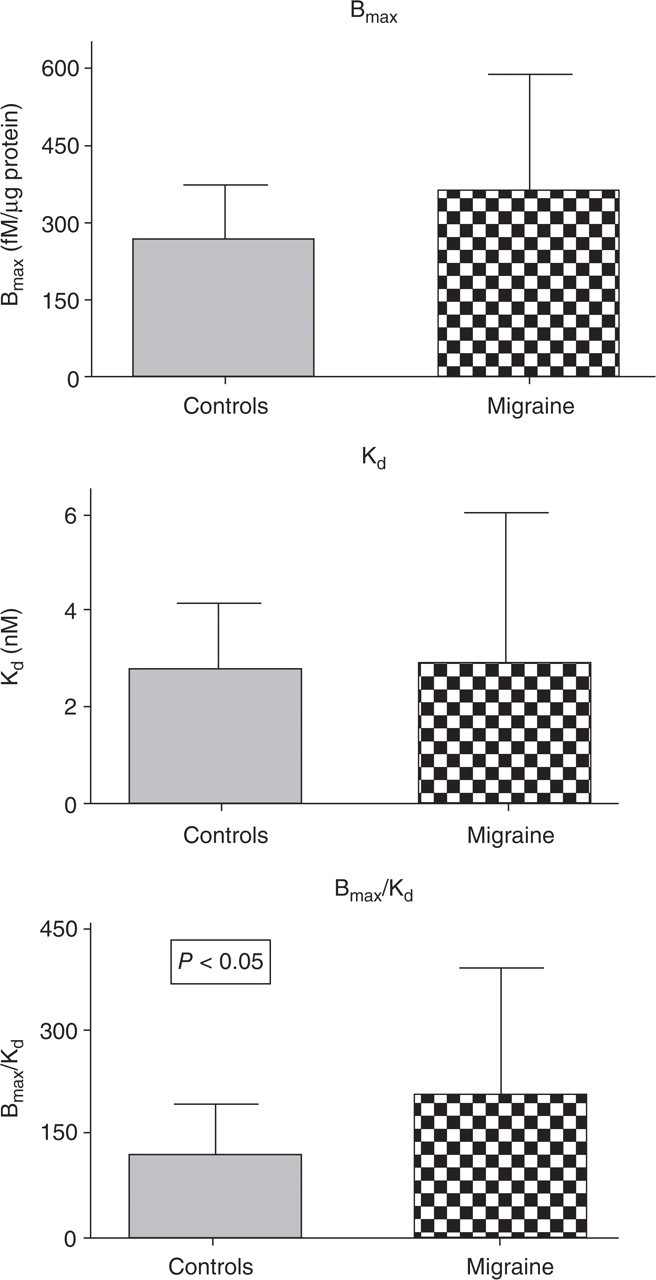
Ouabain binding parameters of controls and migraine with aura subjects. Bars indicate mean and standard deviation. n = 22 for the control group, n = 19 for the migraine with aura group. The probability shown is for the only statistically significant difference.
Table 1 shows distribution of the binding parameters in the different quartiles. To build these tables, the values of each parameter in the migraine and control groups were pooled. As it can be seen, Bmax and KD showed a rather symmetrical distribution between control and migraine subjects in the various quartiles. By contrast, the Bmax/KD ratio showed an asymmetrical distribution. In the lowest (first) quartile only two out of 10 values (20%) belonged to migraine with aura patients, while in the highest (fourth) quartile seven out of 10 values (70%) belonged to migraine with aura patients. This asymmetry was statistically significant (P < 0.03, χ2 for trend).
Distribution of the binding parameters by quartile in the two populations. Probability shown is for χ2 for trend

Moreover, no control subject had a Bmax/KD ratio higher than 398, while three migraine with aura patients (16%) had a ratio higher than this value. Thus, a Bmax/KD ratio higher than 398 had a capability, in this small series, to diagnose migraine with aura with a specificity of 1.0 (95% confidence interval: 0.29–1.0). When the mean of controls plus two times the standard deviation (i.e. 276) was used as a cut-off, one subject out of 22 (4%) exceeded this value in the control group, while four out of 19 (21%) exceeded this cut-off in the migraine group. Therefore, in this small population a Bmax/KD ratio greater than the means of the control group plus two standard deviations singled out 21% of the pathological cases and 4% of the normal ones. This corresponded to the following computed parameters: odds ratio 5.6 (95% confidence interval 0.57–55), sensitivity 0.58 (95% confidence interval 0.41–0.74), specificity 1.0 (95% confidence interval 0.29–1.0), positive predictive value 1.0 (95% confidence interval 0.85–1.0), and negative predictive value 0.16 (95% confidence interval 0.034–0.40).
Discussion
Our data show that in an albeit small population of migraine with aura patients the parameters (Bmax and Kd) of ouabain binding to circulating lymph cells are within normal limits, while their ratio is abnormally high.
KD is a gauge of ligand affinity and is mainly affected by the Na/K-ATPase subunit composition and structure (11–14). In our migraine with aura population this parameter was superimposable to controls, thus affinity of ouabain to Na/K ATPase and, presumably, its subunit composition were not different from controls. It is known that a genetic mutation of Na/K ATPase is the cause of familial hemiplegic migraine, a rare form of inherited migraine with accompanying motor symptoms (6). However, our finding of a normal KD of migraine with aura patients is in agreement with investigations showing that variant of Na/K ATPase is not responsible for most cases of more common migraine (7). The other major binding parameter, Bmax, is a gauge of the number of available binding sites, and therefore correlates with enzyme expression. In our migraine with aura population, only a non-significant trend towards higher Bmax levels in migraine patients was observed.
The ratio Bmax/KD has a less straightforward meaning in terms of biological regulation or structure of the enzyme. Nevertheless, a statistically significant difference was found between migraine with aura and control subjects, this ratio being higher in patients. Expression of the Na/K ATPase gene is affected by environmental factors including hormones, developmental stage, ionic composition and mechanical stimuli (15–20).
It is likely that a balance exists between enzyme structure and expression. Our data indicate that in migraine with aura this balance is disrupted, in such a way that enzyme isoforms with higher ouabain affinity (and thus relatively lower KD) tend to be over-expressed, thus causing higher than normal values of the Bmax/KD ratio. As a higher affinity for ouabain appears to imply a higher Na pump activity (14), the finding of an overall increase of the Bmax/KD ratio for ouabain binding suggests that patients tend to reach an equilibrium point implying a higher Na pump capability.
This is a preliminary finding that should be corroborated by more extensive investigations. However, and whatever its biological meaning may be, it carries in our opinion important implications concerning two aspects.
First, it could lead to the identification of a biological marker of the disease. Diagnosis of migraine with aura has been so far based only on data from the clinical history. If a biological marker could identify at least some of the migraine with aura patients, setting them apart from controls, the way we diagnose this disease could be deeply affected. Our results are from a small population, therefore they can not lead to normative data; however, they do suggest that a Bmax/KD ratio higher than 400 could have an acceptable specificity in identifying migraine with aura patients, and that a Bmax/KD ratio higher than the mean of controls plus two standard deviations (276 in our data) may be strongly associated with a diagnosis of migraine with aura. If our present findings were confirmed in a larger series, they could lead to a diagnostic marker of migraine with aura, something that is now completely absent from the clinician's armamentarium.
Secondly, it is likely that changes in Na/K ATPase play an important part in the generation of migraine aura. This is in agreement with previous findings by one of us, and others [5], showing that inhibition of this enzyme is sufficient to reproduce a spreading depression-like depolarization. The latter is thought to be the basic change leading to aura symptoms (1). It has been shown that during aura, but not in common migraine, brain phosphorylation potential is decreased (21), possibly indicating decreased Na/K ATPase activity due to lack of substrate. Thus, it is possible that a malfunctioning of Na/K ATPase plays a role in generating migraine aura, at least in some patients.
Finally, we should underline that our data refer to a Na/K ATPase that was derived from circulating lymph cells. However, such Na/K ATPase has been used before as a tool for investigating the function of this enzyme in neurological diseases (22, 23).
Thus, our data show a significant difference between normal controls and migraine with aura subjects concerning the Bmax/KD ratio of ouabain binding. They strongly suggest that in migraine with aura the equilibrium between expression and composition of Na/K ATPase, an enzyme whose inactivation causes spreading depression (5), is altered. Moreover, they provide the rationale for a larger study to investigate if this statistically significant difference may be exploited as a biological marker of migraine with aura. Our data are from a rather small population, therefore this study should be considered preliminary. In our opinion, more research is warranted on this subject, to more definitely elucidate the role of Na/K ATPase in the diagnosis and pathogenesis of migraine with aura.