
Abstract
The aim of this study was to evaluate olfactory hypersensitivity (OHS) between attacks in migraine patients. Seventy-four migraine patients and 30 controls were enrolled. The presence of OHS was evaluated using an oral questionnaire and a chemical odour intolerance index. Subjects had to rate the intensity and hedonicity of 12 odourants using a linear rating scale. Twenty-six patients (35.2±) but no control subjects reported an interictal OHS (P < 0.001). Logistic regression analysis showed that patients with OHS presented a greater attack frequency, a higher number of odour-induced migraines and visual hypersensitivity when compared with other patients. Disease duration, age, gender and auditory hypersensitivity were not associated with OHS. OHS patients judged odours less pleasant than did other patients and controls, whereas the intensity scores were identical in both groups. OHS between attacks was significantly associated with odour-triggered migraine and an alteration of hedonic judgement.
Introduction
Migraine attacks are characterized by hypersensitivity to visual and auditory stimuli (1). Intolerance to odours may also occur during such attacks, and was recently found to be very specific to migraine in the absence of nausea (2). Several studies have suggested that hypersensitivity to exteroceptive stimuli may persist between migraine attacks. Photosensitivity is the most studied form of interictal hypersensitivity (3, 4). Interictal olfactory dysfunction has also been reported in migraine patients with smaller olfactory event-related potential (ERP) amplitudes when compared with controls (5). However, a change in olfactory detection thresholds remains controversial. Whereas some authors have reported a decreased threshold for vanillin, suggestive of an interictal hyperacuity to odours (6), others have found an increased detection threshold for pyridine (7).
These discordant findings may partly reflect heterogeneous olfactory dysfunction in the population of migraine patients, since the latter are likely to include patients with and without interictal olfactory hypersensitivity (OHS). OHS can be referred to as chemical odour intolerance and has been described in patients with so-called multiple chemical sensitivity (MCS), a chronic acquired disorder characterized by the occurrence of reproducible somatic, cognitive or affective symptoms in response to exposure to low concentrations of chemicals usually well tolerated by the general population (8–10). Up to 70% of patients with MCS may suffer from odour-induced headaches (11).
Discrepancies regarding the olfactory detection threshold in migraine patients might also indicate that OHS reflects an altered supraliminal olfactory perception. Since migraine patients often complain of osmophobia, it could be expected that the subjective judgement of odour intensity and/or hedonicity would be affected. It has previously been shown that these judgements are based on specific processes different from those involved in familiarity and edibility judgements (12, 13) and that they may be selectively affected in various neurological diseases (14–17).
In this present study, we hypothesized that patients with migraine associated with OHS might suffer from more marked interictal olfactory dysfunction than migraine patients without OHS and controls, and specifically evaluated the odour intensity and hedonicity judgement in these three populations. We used a battery of everyday odorants as used in an olfactory judgement and identification test developed to assess various aspects of olfactory functioning in a clinical setting (14–16). In previous studies examining patients with either Alzheimer's disease, schizophrenia or Parkinson's disease, this test proved to be effective in detecting olfactory deficits, which varied as a function of the pathology.
Materials and methods
Subjects
Seventy-four migraine patients and 30 control subjects participated in the study from November 2001 to June 2003 (Table 1). Patients suffering from migraine according to the following criteria were consecutively selected from the out-patient clinics of the three investigators (P.G., G.C. and D.V.): migraine with or without aura according to the diagnostic criteria of the International Headache Society (IHS), disease duration ≥1 year and frequency of attacks per month ≥1. Patients using antimigraine and preventive treatments were accepted. All olfactory tests and evaluations were performed in the migraine-free interval, at least 72 h after the last attack. Control subjects neither suffered from migraine nor from other chronic or recurrent headaches. Exclusion criteria for all subjects included chronic daily headache, possible brain damage, current substance abuse, known anosmia, rhinal disorders (cold, active allergies, history of nasal-sinus surgery). Recruitment of patients and control subjects was performed after establishing inclusion and exclusion criteria. The subjects provided their informed consent to participate.
Population study: demographical and clinical data of the olfactory hypersensitivity (OHS) and non-OHS patients and controls

Subjective ratings of olfactory hypersensitivity
The presence of an OHS during the migraine-free period was evaluated by asking patients whether they regarded themselves as clearly hypersensitive to odours between attacks. These data were completed using a chemical odour intolerance index previously validated in patients with MCS (18). It is a five-item visual rating scale used to judge intolerance to five types of odorants: pesticide, paint, perfume, new carpet and car exhaust. Each scale ranges from 1 (almost never any symptoms) to 5 (almost always). An overall scale was obtained by summing the values of the five-item rating scales. It thus ranged from 5 (no odour intolerance) to 25 (maximal odour intolerance). OHS and the chemical odour intolerance index were also assessed in normal subjects. We finally asked the patients whether some or all of their migraine attacks were precipitated by odorants, provided that they could distinguish this phenomenon from an early ictal osmophobia.
Patients were also assessed to evaluate visual and auditory hypersensitivity using a numerical category scale including four discrete response alternatives associated with a number from 1 (not at all) to 4 (very strongly).
Odorants
Twelve odorants were chosen from 185 previously evaluated by a large number of subjects (12). The odorants were mushroom, pine, strawberry, smoked salmon, clove, lemon, lavender, ether, mint, citronella, vinegar and gas. Strawberry, lemon, lavender, mint and citronella are usually judged as rather pleasant, whereas the other odorants are usually rated as rather unpleasant (12). They were contained in 15-ml yellow glass bottles with screw lids in polyethylene (Fischer, Erlancourt, France). An odorous solution (10%) was obtained by diluting 0.5 ml of an odorant in 4.5 ml of odourless solvent (mineral oil). It was placed in the bottle and absorbed by compressed filaments of polypropylene. Due to the high potency of ether, vinegar and gas, concentrations of these products were limited to 1%. Odorants were kept in a refrigerator when not in use and were removed before the experiment began to reach room temperature.
Experimental procedure
Odorants were presented in both nostrils for 5 s, at a rate of one per minute. For each presented odorant, subjects had to successively rate intensity and hedonicity using linear rating scales segmented from 1 to 10. In order to indicate further the degree of each scale, their extremities were marked ‘very weak’ and ‘very strong’, ‘very unpleasant’ and ‘very pleasant’, for each judgement task, respectively.
Statistical analysis
We compared the prevalence of OHS between patients and control subjects from the chemical odour intolerance index values using a one-way analysis of variance (
For testing the olfactory performance during intensity and hedonicity judgements, two- and three-way
Results
Study population
The migraine population included 61 females (82.4%) and 13 males (17.6%) with a mean age of 41.9 ± 11.8 years. Their migraine attack frequency was a mean rate of 6.19 ± 4.40 days per month. The mean duration of the disease was 21.08 ± 12.65 years. Sixty-one patients suffered from migraine without aura, nine patients from migraine with and without a visual aura and four patients presented only migraine with visual aura. The control population consisted of eight males (26.7%) and 22 females (73.3%), with a mean age of 37.8 ± 12.1 years. There was no significant difference between the two groups of subjects in male/female ratio (χ2 = 0.84, P = 0.359) and in age [F(1,102) = 2.56, P = 0.113].
Olfactory hypersensitivity and chemical odour intolerance index
Twenty-six out of 74 migraine patients (35.2%), but no controls, reported an interictal OHS. The mean chemical odour intolerance indices found for the control and patients groups are given in Table 1 and Fig. 1. A one-way
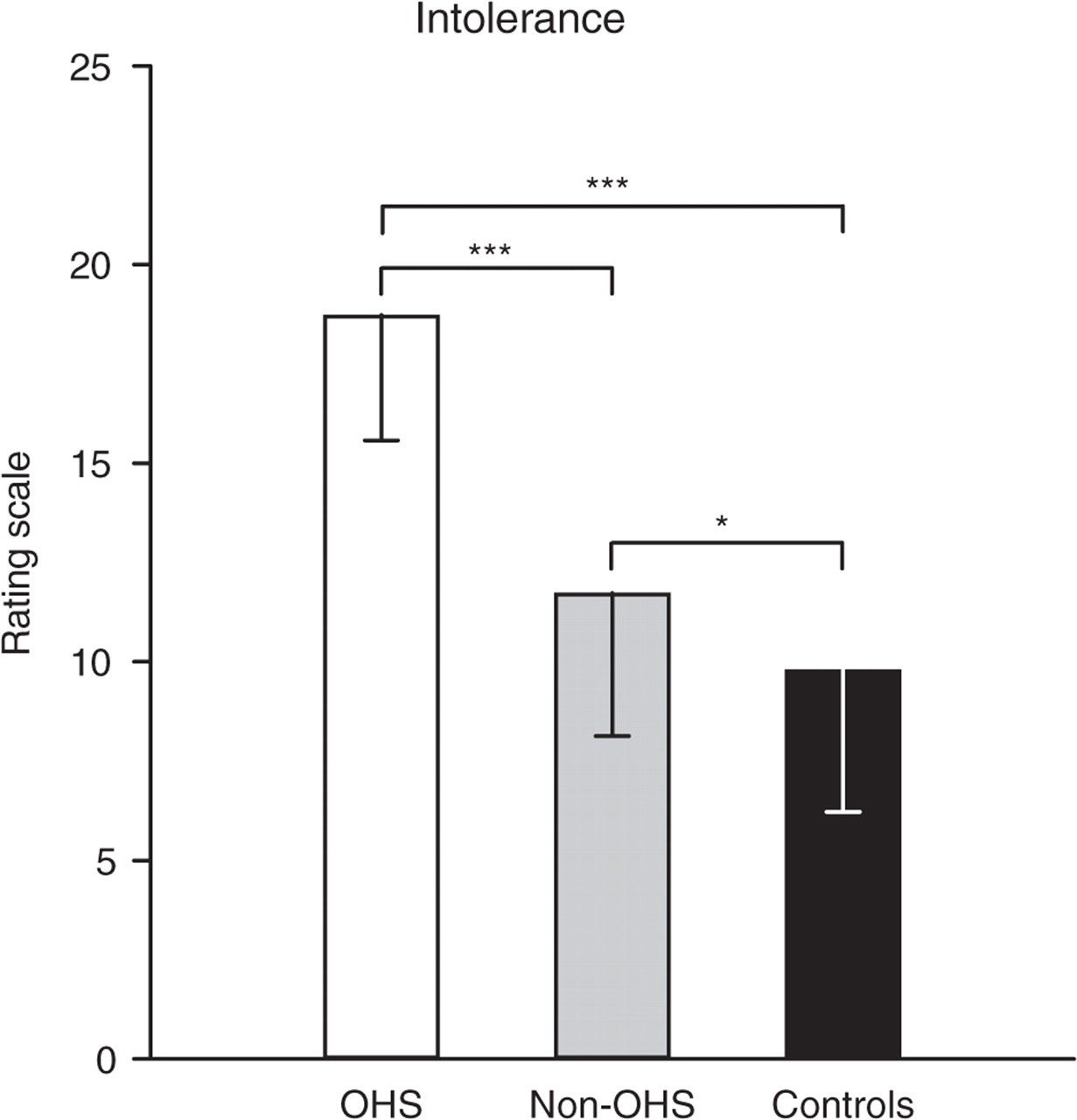
Mean chemical odour intolerance scores for both groups of patients [olfactory hypersensitivity (OHS) and non-OHS] and control subjects. Vertical bars, standard errors of the mean.
Among migraine patients, the logistic likelihood ratio tests performed from the logistic regression analysis showed that the variables regarding odour-induced migraine, attack frequency and visual hypersensitivity were significant (Table 2), with higher rates for each of these variables in OHS than in non-OHS patients (Table 1). The presence of an aura, disease duration and auditory hypersensitivity were not significantly associated with OHS.
Logistic regression analysis of variables of interest to characterize olfactory hypersensitivity (OHS) and non-OHS patients

OR, Odds ratio; CI, 95% confidence interval.
Preventive treatment distribution was comparable in the two groups. In the OHS group, 13 patients (50%) took one or several preventive treatment including β-blockers (n = 6, 23%), amitriptyline (n = 1, 4%), anticonvulsant (n = 1, 4%), serotonin antagonist (n = 1, 4%), flunarizine (n = 3, 11%) and selective serotonin reuptake inhibitors (SSRIs) (n = 3, 11%). In the non-OHS group, 22 (46%) had one or several preventive medication such as β-blockers (n = 14, 29%), amitriptyline (n = 2, 4%), anticonvulsant (n = 1, 2%), serotonin antagonist (n = 5, 10%), flunarizine (n = 3, 6%) and SSRIs (n = 3, 6%). The total number of patients with preventive treatment was not significantly different between the two groups (χ2 = 0.117, P = 0.732).
Olfactory performance
Olfactory behavioural performances rated for patients with and without OHS were then compared with those of control subjects. For the intensity judgement task, a two-way

Mean hedonic judgement scores for both groups of patients [olfactory hypersensitivity (OHS) and non-OHS] and control subjects. Vertical bars, standard errors of the mean.
Discussion
We found that OHS observed in migraine patients between attacks was significantly associated with the presence of odour-triggered migraine and was associated with attack frequency, decreased hedonicity judgements of odours and visual hypersensitivity.
Characterization of OHS patients
We found a high prevalence of interictal OHS in our migraine population (35%), whereas no control subject presented such hypersensitivity. The fact that none of our control subjects described OHS is very likely due to our exclusion criteria and, more specifically, to the lack of any past history of headache, since the latter can be found in up to 70% of patients with OHS (11).
Only one other study has evaluated olfactory as well as other types of sensory hypersensitivity in migraineurs between and during attacks (22). Whereas 46% of patients complained of olfactory hypersensitivity during migraine, less than 5% reported such an interictal OHS, which was not significant compared with the control population. Several factors might explain the higher prevalence of interictal OHS in our population of migraineurs. First, our study was not population based and was not intended to determine precisely the prevalence of interictal OHS in migraine patients. In particular, we did not control for the likely bias resulting from patients with OHS being more interested in participating in our study than migraineurs without OHS. Second, the mode of assessment used to detect chemical odour intolerance has varied between studies. Whereas Vingen et al. (22) questioned patients about sensitivity to six odours, four of which were different from ours, we primarily assessed the presence of OHS by simply asking subjects whether they viewed themselves as clearly hypersensitive to odours, excluding osmophobia during migraine attacks. This assessment was completed by a five-item questionnaire previously validated in patients with chemical odour intolerance or MCS. The two evaluations strongly correlated, providing additional support to the validity of our findings.
A striking finding in the present study, as extracted from multiple logistic regression, was the significant association between the presence of interictal OHS and odour-triggered migraine. The phenomenology of odour-triggered migraine is still a matter of debate, with figures ranging from 1% to 60% of migraine patients (23, 24). This discrepancy may, in part, relate to the difficulty of distinguishing early occurring ictal osmophobia from true odour-triggered attacks (25). Regardless of the ongoing debate, one could hypothesize that both odour-triggered migraine and osmophobia-associated migraine might lead to a conditioning process following repeated association between odour and migraine. The significant association found between OHS and migraine attack frequency could be an argument for this hypothesis. Conditioning occurs when a neutral stimulus is paired with a stimulus that reflexively elicits a particular response (Pavlovian conditioning) or refers to the process of increased sensitivity to the effects of a stimulus following exposure to a noxious stimulus (sensitization). The development of migraine in response to odours (whether this link is accurate or inaccurate) could result in avoidance behaviour, whereby the patient seeks to minimize exposure to the trigger (26).
Olfactory performances in migraine patients
To test the hypothesis that migraine patients with interictal OHS suffer from an olfactory dysfunction, we investigated the intensity and hedonicity judgements of odours in both migraineurs and controls. We found no difference in intensity judgements between groups but an altered hedonic rating in migraineurs with interictal OHS when compared with healthy subjects and migraineurs without OHS. Specifically, migraine patients with interictal OHS rated odours as less pleasant than the two other groups, whereas the latter showed comparable hedonic ratings. One study has assessed odour hedonicity in migraineurs and, when compared with controls, found no differences in the rating of acetone (6), an unpleasant odorant known to activate the trigeminal system (27). The fact that these authors assessed only a single odorant and did not distinguish patients with and without OHS may well explain their negative findings.
A few studies of olfactory thresholds in migraineurs have been reported, but they show apparently discordant results. Hirsch (7) showed that odour thresholds to pyridine, a molecule also well known to stimulate the trigeminal pathways, were higher in 18% of patients, Snyder and Drummont (6) found unmodified thresholds for acetone, and lower thresholds for vanillin. More recently, Grosser et al. (5) found no differences for threshold values and identification of odourous (H2S) and trigeminal (CO2) stimuli between migraineurs and controls. However, using an electrophysiological approach and discriminant analysis, they demonstrated that olfactory event-related potentials discriminated between migraineurs and controls better than trigeminal event-related potentials, emphasizing the significance of the olfactory system in migraine. Overall, it is unclear whether migraineurs suffer from an increased sensitivity to either olfactory or trigeminal stimuli. In the present study, we tested bimodal odorants, i.e. odorants activating both sensory systems equally, but did not evaluate detection thresholds.
Although OHS migraine patients on the whole judged odours less pleasant than the non-OHS migraine patients, a significant group–odour interaction further indicated that this reduction in hedonicity rating was especially pronounced for ether. This odour was not previously described among incitant exposures implicated in MCS (28) and we may hypothesize that OHS patients judged ether all the more unpleasant as this odour is reputed to be easily identifiable. Several studies have thus demonstrated that cultural and cognitive information can modulate the hedonicity ratings (29–31). For example, it was observed that an ambiguous mixture of isovaleric and butyric acids is judged more unpleasant when labelled as ‘vomit’ than as ‘Parmesan cheese’ (29).
Olfactory dysfunction comparable to that observed in our migraine patients with OHS has been reported in patients who suffered from MCS (8). In MCS studies, several groups thus found that patients have normal detection thresholds and identification scores (32–37), but that odours were rated less pleasant (35, 37, 38). This suggests that OHS migraine patients could present common physiopathological bases with MCS patients. Nordin et al. (38) has further reported that pyridine was rated more intense and produced more sensory irritation in MCS patients compared with controls, but no difference in intensity scores were found between groups in our study. The discrepancy between these results could, however, be attributed to the fact that we used relatively low concentrations of stimuli, whereas Nordin et al. (38) found that the abnormal intensity rating was observed mainly for high pyridine concentrations.
Physiopathology of olfactory hypersensitivity in migraine patients
In the field of research on odour processing, the term hypersensitivity or hyperacuity usually refers to a decreased olfactory detection threshold. In the field of migraine and MCS, this term is used in a broader sense, reflecting the discomfort perceived by the patient as an inappropriate and excessive odour-induced response. A modification of hedonic judgement, as observed in the present study, could be one of the aspects of this form of hypersensitivity and so reflect a central dysfunction of the olfactory processes. What are the brain mechanisms/processes that can subtend OHS in migraine patients?
Interictal OHS may reflect the cortical hyperexcitability suggested in migraine patients, based on observations of higher amplitudes of visual (e.g. 39–41) and somatosensory (42, 43) evoked potentials, as well as on findings from magnetic resonance spectroscopy and magneto-encephalography (44, 45). A significant correlation is observed between the hyperexcitability and the frequency of migraine attacks in evoked potential and magneto-encephalographic studies (45, 46), a result which is consistent with the association observed in our study between OHS and migraine attack frequency.
OHS associated with an increased unpleasantness also suggests a dysfunction of the limbic system. Several functional imaging studies have indeed revealed the strong involvement of the limbic circuit, including the amygdala, orbitofrontal, cingulate and insular cortices, in emotional response and the hedonic judgement of odours (e.g. 47–52). We can hypothesize that all or part of this neural network might be hyperactivated in OHS migraine patients. Such hyperactivation might further reflect changes in the serotoninergic system, according to the suggested role of this system in the modulation of cortical information and pain processing (5) and migraine pathophysiology (53, 54). Specifically, low serotoninergic activity could result in high cortical reactivity (55).
In conclusion, we have identified a subgroup of migraine patients who complain of interictal OHS, demonstrate significant alteration of hedonic judgement and suffer from more frequent odour-triggered attacks than other migraineurs. Future studies of olfactory dysfunction in migraine should take into account these specific populations and further investigations are needed for a better understanding of the processes involved in olfactory dysfunction.
Acknowledgements
This work was supported by the Hospices Civils de Lyon and the Programme Hospitalier de Recherche Clinique (PHRC 2001 of the Rhone-Alpes Region).