
Abstract

In the second edition of the International Classification of Headache Disorders (ICHD II) the entity of ophthalmoplegic migraine (OM) is no longer classified with migraine but as a neuralgia (13.17) (1), because in many cases of this rare condition signs of inflammation of the affected nerve have been found on gadolinium-enhanced magnetic resonance imaging (MRI) scans (2–7).
Neuromas (schwannomas) of the cranial nerves affect mainly the VIII and the V nerve, whereas all the other nerves are only rarely affected (8). Regarding schwannomas of the 3rd nerve, the usual clinical presentation is a painless deficit (9) and asymptomatic cases are occasionally discovered by chance (10).
We present a case of OM where the MRI findings are compatible with a schwannoma of the ipsilateral 3rd nerve.
Case report
A 14-year-old girl had a history of OM since the age of 2 years. Apart from OM she had had an unremarkable medical history and no family history of neurological diseases, including migraine.
The attacks usually started with a right periorbital headache of pressing and pulsating character without nausea, photo- or phonophobia and were not affected by head movement. The duration of the headaches was 4–7 days, by the end of which she developed a complete ipsilateral oculomotor lesion with dilation of the pupil lasting for 1–2 months with a slow complete recovery. The frequency of the episodes was between two to three per year and one every 1–2 years.
She was first seen in 2002 (aged 12), when she reported short episodes of incomplete right ptosis and diplopia accompanied by headaches lasting for several days and returning every 1–2 weeks over a period of 2 months. She then went into remission and was seen again in March 2004 with a headache lasting for 4–5 days, during which a complete 3rd nerve ophthalmoplegia developed from which it took 6 weeks to recover. She obtained oral steroids for a week starting during the headache phase under which the headaches disappeared within 24 h. She has had no relapse since that episode without any treatment.
The imaging results of the last episode are presented here.
On MRI imaging (Fig. 1) there was a nodular lesion of 7 mm diameter on the cisternal portion of the right oculomotor nerve with strong enhancement after gadolinium, fulfilling the MRI criteria of a schwannoma (11). A control MRI 4 months later, 2 months after complete clinical recovery, still showed the gadolinium enhancing lesion, although the intensity of the enhancement was weaker. On the heavily weighted unenhanced T2 sequence the lesion appeared less dense during the acute phase compared with the remission phase, suggestive of oedema while symptomatic.
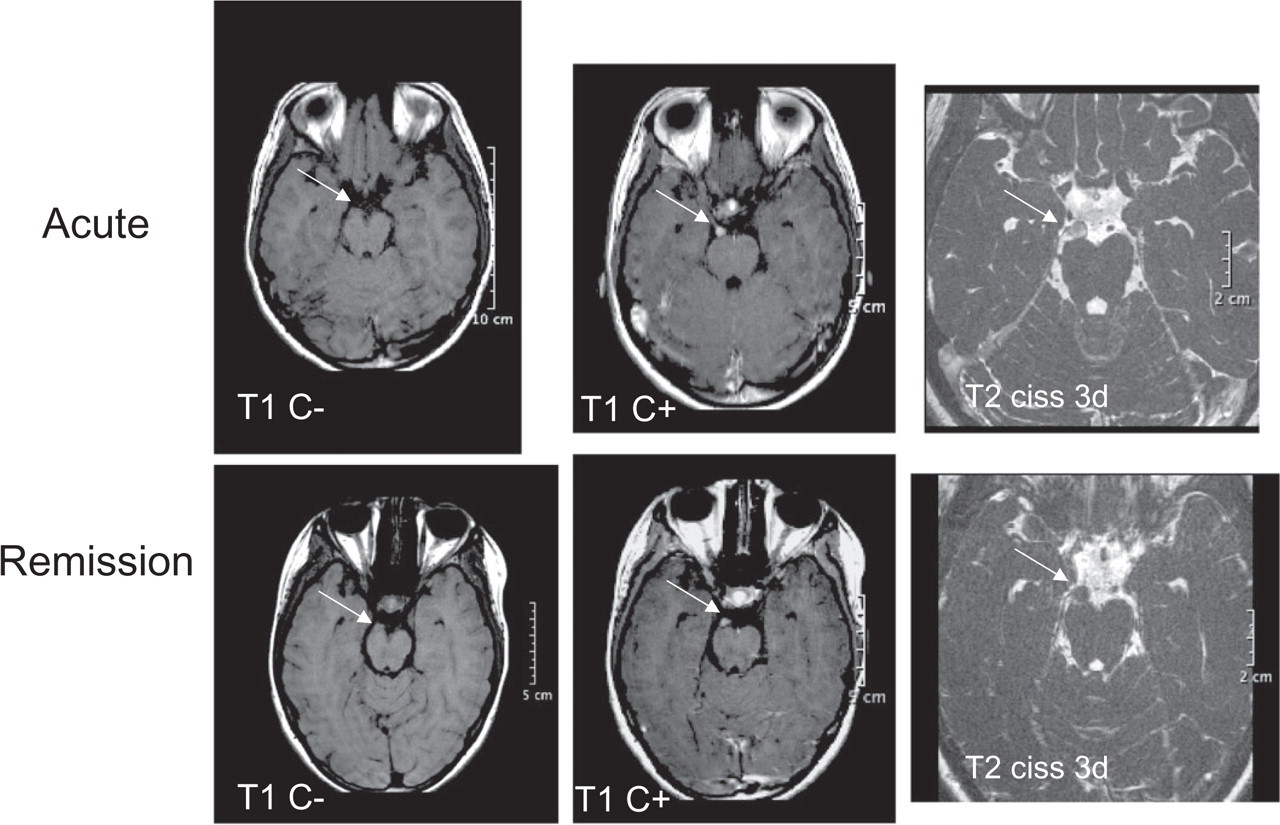
Magnetic resonance imaging images during the acute phase and 4 months later, 2 months after full recovery.
A review of a former MRI done on a different machine in another hospital 10 years earlier, when the patient was age 4, revealed that the nodular, strongly gadolinium-enhancing lesion on the cisternal part of the oculomotor nerve was already visible and of similar size to that at the recent examination.
Discussion
This is a case of a 14-year-old girl with a 12-year history of right-sided OM, in whom a schwannoma of the ipsilateral oculomotor nerve was found. The presentation of OM was typical with right-sided periorbital headache episodes lasting for several days, during which a partial or complete oculomotor nerve lesion developed from which it took days to weeks to recover completely.
Oculomotor nerve schwannomas are very rare (8) and the clinical presentation is a slowly progressive partial or complete lesion, mostly painless (9). Chance discoveries of asymptomatic oculomotor schwannomas have been reported (10).
The reclassification of OM in the ICHD II from migraine to neuralgia (1) was based on its headache features atypical of migraine and the finding of swelling and stronger gadolinium enhancement of the oculomotor nerve during the acute phase as opposed to the quiescent phase, favouring inflammation (7).
In the index case the stronger gadolinium enhancement of the schwannoma during the acute phase compared with a few months after complete clinical remission as well as the higher water content seen on heavily T2-weighted images during acute phase also suggest an inflammatory component.
One case of the coexistence of OM and ipsilateral 3rd nerve schwannoma has been reported previously (12). The authors had an acute (from an episode 6 years earlier) and a follow-up MRI during a recovery phase and noticed no difference.
The coexistence of two rare conditions (OM and oculomotor schwannoma) suggests that a mere coincidence is unlikely. The clinical presentation of schwannomas is usually a slowly progressive deficit and not a series of acute deficits with complete remissions in between. As a potential mechanism for the thickening of the prepontine part of the oculomotor nerve observed in OM, it has been proposed that repeated inflammation could lead to a demyelination/remyelination process with Schwann cell proliferation and onion bulb formation (5). In the present and the single previously reported case of OM and an ipsilateral schwannoma, the Schwann cell proliferation could have taken a more nodular shape.
In the index case the size of the nodular lesion did not change in a 10-year follow-up and in the case reported by Kawasaki (12) there was no change in a 6-year follow-up. Therefore, in spite of repeated episodes of OM the schwannoma does not seem to be progressive. This observation and the complete clinical remissions between episodes would not justify surgical intervention.