
Abstract
The objective of this study was to determine predictors of onset of new headache episodes and recovery from headache over one year. A population-based cohort study was conducted, comprising a baseline postal survey to a random sample of adults aged ≥18 years, with follow-up survey after 1 year. Risk factor data at baseline were compared with headache status at follow-up in two groups: (i) those free of recent headache at baseline and (ii) those with a recent headache at baseline. In respondents free of recent headache at baseline, previous headache [risk ratio (RR) 4.15], the presence of other pain at baseline (RR 1.43), severe sleep problems (RR 1.67) and drinking caffeine (RR 1.99) increased the risk of a new headache episode during the follow-up year. In respondents with recent headache at baseline, less severe headaches at baseline predicted recovery during the follow-up year, as did the absence of anxiety [recovery ratio (ReR) 2.84] and of sleep problems (ReR 2.77). Risks for increased headache-related disability reflected those for onset of a new episode and these risks increased in strength for large increases in disability. Sleep problems and caffeine consumption increase the risk of developing headache and thus provide targets for prevention. Low levels of anxiety, sleep problems and the absence of other pain improve the likelihood of recovering and remaining free from headache.
Introduction
Headache can limit activities and result in work absence (1, 2). Since headaches affect more than two-thirds of the UK population in a 1-year period (3–6), the resulting impact on public health and the workplace is considerable. Identifying causes of headaches has the potential to prevent or reduce this impact.
Headaches have been found to be associated cross-sectionally with anxiety and depression (7–10), sleep disturbances (11) and musculoskeletal pain (12). However most of these studies were of severe headache or migraine and less is known about influences on all headaches in the population. Previous prospective studies of specific headache types have identified a number of predictors of incidence. Lyngberg et al. (13) in their 12-year follow-up of a general population sample found predictors of migraine incidence were younger age, female gender, family history of migraine, existing frequent tension-type headache (>14 headache days per year) and having a high work load. Predictors of frequent tension-type headache incidence were again younger age and female gender and also sleep problems, inability to relax after work and poorer self-rated health. Scher et al. (14) investigated the onset and remission of chronic daily headache. Onset was associated with obesity and more frequent baseline headaches and remission with being educated to a higher level, non-white ethnic group, being married and having a diagnosis of diabetes. Depression has also been identified as a predictor of migraine but not of other severe headaches and this relationship is bidirectional, with migraine also predicting depression (15). Alcohol intake and caffeine withdrawal are also recognized causes of headache (16).
This paper reports a population-based cohort study designed to identify risk factors for onset of new headache episodes and recovery from headache.
Methods
Study population
Two population-based cohorts were identified and followed prospectively: (i) those with no recent headache (during the previous 3 months) and (ii) those with recent headache, using a population survey of 5000 adults, described elsewhere (17). In brief, random samples of 1000 adults aged ≥18 years were selected from the practice register of each of five general practices in North Staffordshire, UK and mailed the North Staffordshire Headache Survey. This contains questions about headache occurrence, characteristics and effects, general health and demographic information. Its development and testing have been reported elsewhere (18). One year after the initial survey, all baseline responders still registered at the practices who had given permission for further contact were asked to complete a further questionnaire, similar to the baseline but with additional questions about changes in headaches since baseline. Ethical approval for the study was obtained from the Local Research Ethics Committee.
Both questionnaires enquired about any headache in the previous 3 months (which was the definition of ‘recent headache’ for this study). In addition, the baseline questionnaire asked about headaches ever and the follow-up about headaches in the last 12 months. Those with a recent headache were asked about frequency, duration, pain, accompanying symptoms and actions taken to relieve the headache. Associated disability was assessed using the Migraine Disability Assessment (MIDAS) and categorized as mild (0–5), moderate (6–10), severe (11–20) or very severe (21+) (19, 20). The Hospital Anxiety and Depression Scale (HADS) (21) was included and respondents classified as: 0–7, no depression/anxiety, 8–10, possible and ≥11, definite. Respondents were asked to shade on a whole body manikin (front and back view) any aches or pains they had experienced for ≥1 day in the last month. The manikin was assessed for pain shadings in areas relating to neck pain (22), shoulder pain (23) and general bodily pain in six areas based on definitions for widespread pain (24). Average daily caffeine (none, one to two cups, three to five cups, six or more cups) and weekly alcohol (none, 1–3 days, 4–7 days) consumption were recorded. The level of sleep problems experienced over the last month was assessed based on work by Jenkins et al. (25) by asking whether they had experienced any of the following on some or most nights: trouble falling asleep, waking up several times per night, trouble staying asleep and waking up after the usual amount of sleep feeling tired and worn out. From this, sleep problems were classified into none (no problems reported), slight (minimum one question ‘on some nights’), moderate (minimum one question ‘on most nights’) and severe (all questions ‘on most nights’).
Analysis
Respondents were categorized according to headache at baseline and during the follow-up year into: ‘never’, no headache at either time; ‘new headache’, headache during follow-up but not at baseline; ‘recovery’, headache at baseline but not during follow-up; and ‘continuing’, headache at both times and frequencies and percentages calculated.
To investigate determinants of onset and recovery the main outcome was a report of headache during the follow-up year. The two cohorts were analysed separately: (i) in those with no recent headache at baseline, cumulative 1-year incidence of headache was used to explore predictors of new headache episodes; (ii) in those with recent headache at baseline, predictors of headache recovery were investigated. Survival analysis (Cox regression) was used, in each of the two cohorts, to calculate age and gender adjusted risk ratios (RR) for the associations between baseline characteristics and headache status during follow-up. In the second cohort this estimate is termed the recovery ratio (ReR) as it represents the ‘risk ratio for recovery’.
To investigate the extent to which headache severity confounds any link between general health and headache recovery, the associations were re-calculated adjusting for headache disability level, in addition to age and gender.
To investigate the effect of headache severity on the relationships presented, we investigated changes in headache-related disability by examining predictors of an increase in headache-related disability—from mild at baseline to at least moderate at follow-up. We first examined the relationship of these predictors in all relevant participants. Second, we assessed any change in the magnitude of these predictors in the subgroup of participants whose headache disability was at least severe at follow-up, i.e. removing those people whose headache disability moved from mild to moderate. This was done using survival analysis as described above. Statistical analysis was performed in SPSS version 10.0 (SPSS Inc., Chicago, IL, USA) (26).
Results
In the baseline survey 2662 completed questionnaires were returned, a response of 56%. Further details of respondents and their headache characteristics have been reported elsewhere (17). A total of 2225 (84%) consented to receive further questionnaires and, of those, 2141 were alive and still registered with the practices 12 months later. These were mailed the 12-month survey and 1589 (74%) returned completed questionnaires, of whom 56% (n = 892) were female and whose median age was 52 years (range 18–90).
Of the 1589 who responded to both surveys, 71% experienced headache in the 3 months prior to the baseline survey and 76% reported headache during the follow-up year. Of the 1134 reporting a recent headache at baseline, all but 73 reported a headache in the follow-up year (Table 1).
Headache in the previous 3 months at baseline and during the follow-up year (n = 1589)

Predictors of new headache in respondents reporting no recent headache at baseline
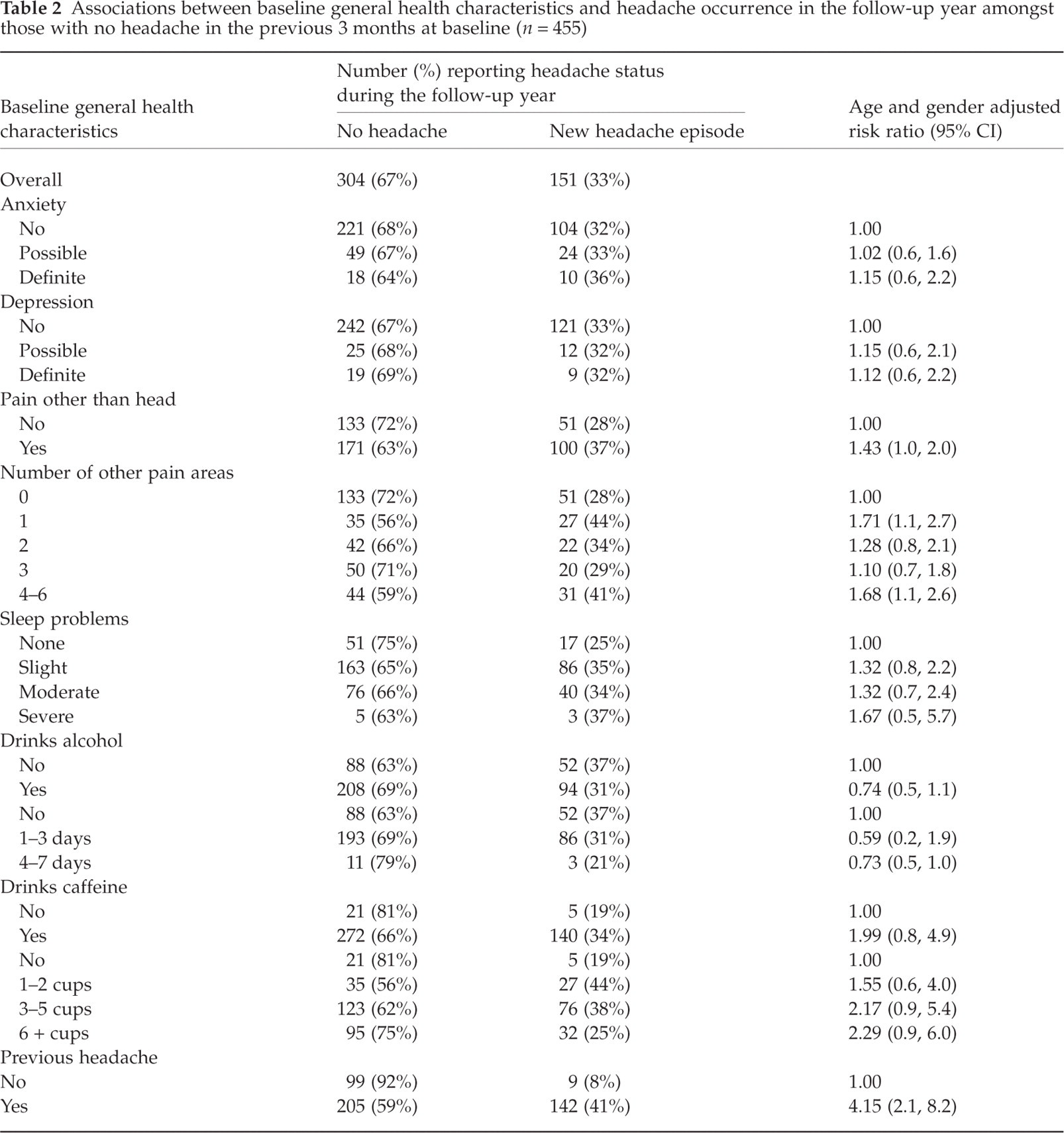
Of the 455 respondents who reported no recent headache at baseline, one-third (n = 151) reported a new episode of headache during the follow-up year. New incidence of headache during the follow-up year among those with no recent headache at baseline was associated with previous headache (prior to baseline 3 months free of headache) (RR 4.15), sleep problems and drinking caffeine. Dose–response relationships were seen when assessing the relationship of headache incidence to the severity of sleep problems and the amount of caffeine consumed daily. Pain at baseline other than in the head area marked on the pain manikin was also associated with new incidence of headache (RR 1.43), although there was no clear trend with the number of other painful areas shaded (Table 2). Moreover, when specific regions close to (shoulder and neck) and further from (legs) the head were examined, the increase in risk of incidence was similar (data not shown). Calculating the population attributable fraction for sleep problems suggests that, given a causal association, 25% of new headaches in those reporting a headache-free period of 3 months at baseline could be eliminated if sleep problems were addressed.
Associations between baseline general health characteristics and headache occurrence in the follow-up year amongst those with no headache in the previous 3 months at baseline (n = 455)
Predictors of recovery from headache in respondents reporting recent headache at baseline
Headache recovery was rare, with 6% of those with recent headache at baseline free of headache during the follow-up year. Less severe headache characteristics at baseline were associated with an increased likelihood of headache recovery in the follow-up year. Mild headache-related disability (ReR 13.14) and none or mild headache pain (ReR 11.44) at baseline were the strongest links with headache recovery in the follow-up year (Table 3). Recovery was also associated with not using medication to treat their headaches (ReR 2.64, 95% confidence interval 1.6, 4.3), the absence of anxiety (ReR 2.84) and of sleep problems (ReR 2.77), of depression (ReR 2.06) and of other pain (ReR 1.58), and the consumption of caffeine (ReR 0.48 for non-consumers) (Table 3). When examining this last relationship further by the amount of caffeine consumed, it was found that, compared with the heaviest caffeine drinkers (six or more cups per day), the reduced risk of recovery was confined to the non-consumers. All associations were reduced but persisted after adjustment for headache-related disability (data not shown).
Associations between baseline characteristics and headache recovery during the follow-up year amongst those with headache in the previous 3 months at baseline (n = 1134)∗
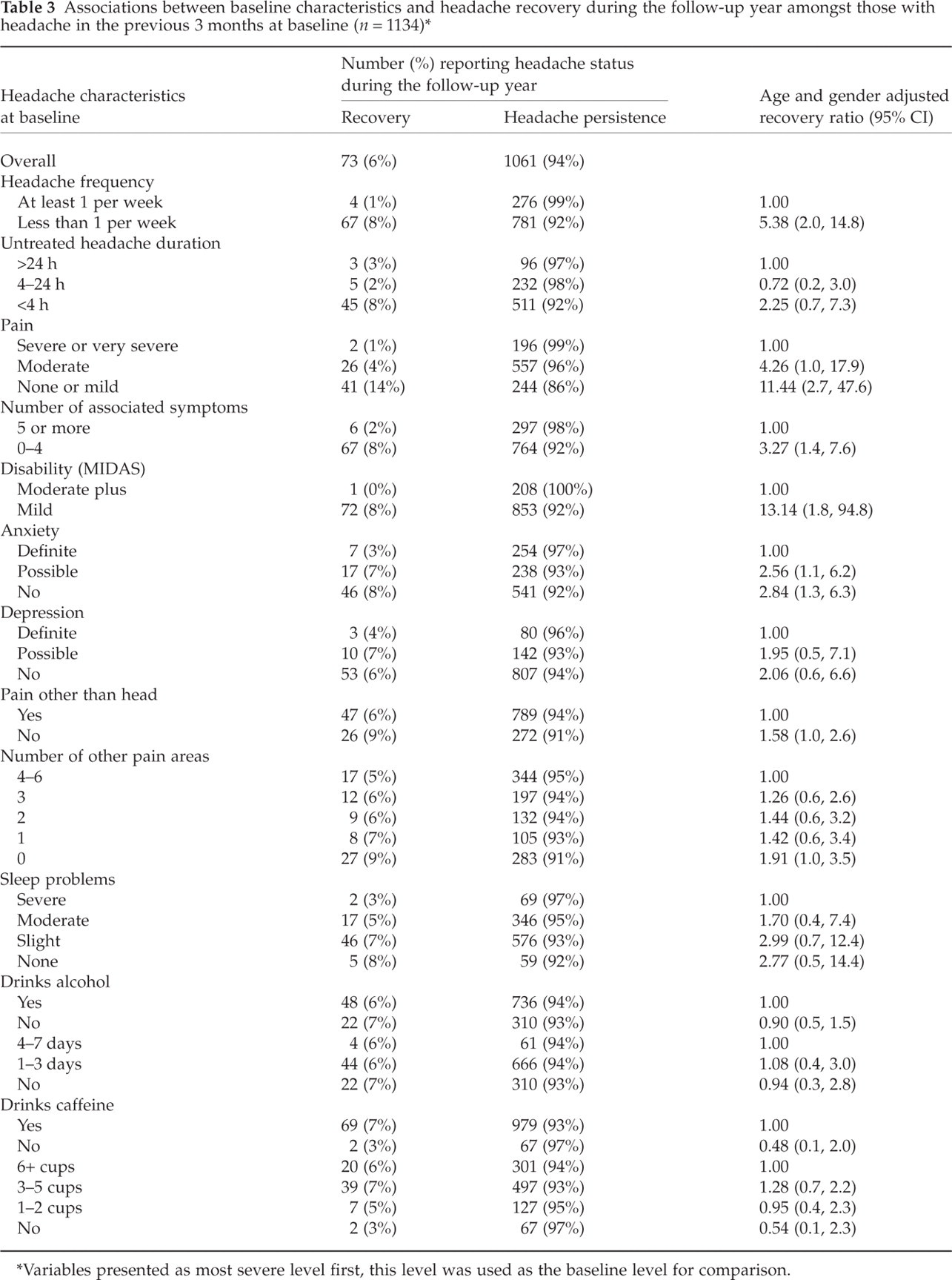
Variables presented as most severe level first, this level was used as the baseline level for comparison.
Effect of severity of headache disability on predictors of headache persistence
Anxiety, depression, at least three other painful areas and severe sleep problems predicted an increase in disability in those with mild disability at baseline. When focusing on the subgroup of participants whose headache disability increased from mild at baseline to either severe or very severe at follow-up, the magnitude of these relationships became greater (Table 4).
Associations of baseline characteristics in those with increased headache-related disability at follow-up in those reporting recent headache at both points—effect of disability severity

Discussion
Among people in the general population free of recent headache, we have found previous headache, drinking caffeine, severe sleep problems and the presence of other pain at baseline to be predictors of a new headache episode during the following year. Although headache recovery during the follow-up year was unusual (6%), absence of anxiety, depression, sleep problems and other pain in those with recent headache increased the likelihood of recovery. In those with mild headache-related disability at baseline the characteristics that predicted an increase in disability were anxiety, depression, at least three other painful areas, severe sleep problems and more severe individual headache characteristics at baseline. In the subgroup who moved from mild headache-related disability at baseline to at least severe at follow-up these predictors were the same but stronger.
The follow-up proportion was 74%. The age and gender of responders and non-responders were no different: 56% female and a median age of 52 years. Moreover, the baseline 3-month headache prevalence was almost identical in those who responded to the follow-up questionnaire (71.4%) to that seen in the whole baseline sample (70.3%). Hence, we believe that although participants self-selected whether to complete the follow-up questionnaire, the effect any response bias will have either on the prevalence of incidence and recovery from headache or on the strength and direction of any association will be minimal, as the follow-up responders were, on the whole, very similar to the population they arose from.
We used a period of 3 months to define respondents’ headache status at baseline. Headache is a condition typified by recurrent episodes and we felt 3 months was a reasonable period of time to define whether or not a respondent was a current headache sufferer. Additionally, a period of 3 months enables respondents to remember and record the features of their headache accurately as demonstrated in the literature (27, 28).
The identification of a group of respondents who were free of recent headache at baseline means that characteristics identified at baseline were not affected by the presence of current symptoms. Whilst the confounding effects of age and gender have been allowed for, other confounders may have affected the estimates. However, we were interested in the effects of the specific factors considered here. Although, for example, it might be argued that multiple pain and poor sleep confound each other, these are both factors which might be addressed separately in order to prevent headaches. Moreover, it may be that medication may have played a role (particularly in reducing impact) in sufferers who find effective treatment.
The relationship between headache and sleep disturbances is complex, with sleep disturbances thought to be both a cause and an effect of headache. Sleep disturbances may also be associated with headache because both are common, other conditions give rise to both, and there is a circular effect of reinforcement (‘vicious circle’) (11). Sleep problems predicted incidence of frequent tension-type headache but not migraine in a Danish study (13), which also found that the absence of sleep problems was associated with improvement in headaches in those with tension-type headache (29). Our prospective finding that, for those with no headache at baseline, sleep problems predicted headache occurrence during follow-up is important as the sleep problems occurred before headache onset. Additionally, severe sleep problems predicted an increase in headache-related disability and slight or no sleep problems predicted recovery from headache. This, together with the finding that 25% of new headache in those free of recent headache at baseline might be attributable to sleep problems, confirms the potential of addressing sleep problems as part of the management of headache.
There was no association between baseline anxiety or depression and the incidence of new headache during the follow-up year, which contrasts with findings from our cross-sectional study (30), where there was a strong association with psychological factors. This suggests that headaches may cause anxiety but not vice versa and contrasts with other pain syndromes where psychological distress has been identified as a predictor of pain, such as abdominal, neck and low back pain (22, 31, 32). Breslau et al. (15) have previously shown that depression increases the risk of developing migraine but not other severe headaches. However, our study did find that these psychological factors were linked with worsening of headache disability during follow-up in those who reported headache at baseline.
The finding that other pain predicts both headache onset and persistence parallels studies of other painful conditions where the presence of pain in one area increases the risk of pain occurring in another (22, 31, 33). The finding that headache is related to the presence of painful areas in the rest of the body has been reported in previous cross-sectional studies (12, 34). Hagen et al. (12) has also shown that the likelihood of reporting other concurrent pain is stronger for those reporting more frequent headaches and Hasvold and Johnsen (34) showed strong relationships specifically with concurrent neck and shoulder pain. However, neither of these studies was able to show that the pre-existing pain outside of the head region can predict the future occurrence of headache.
Headache is a well-recognized symptom of caffeine withdrawal (35) but the association with being a caffeine consumer has been less clear, with cross-sectional studies finding no overall link between headache and caffeine consumption but an association with headache for heavy caffeine consumers (30, 36, 37). We found that caffeine consumption predicted both the onset of new headache and recovery from headache, but had no association with changes in headache disability over 1 year. We also found a dose–response relationship with headache incidence but not for recovery from headache. These rather surprising findings may possibly be explained by a selection bias in those with more severe headache opting not to consume caffeine and also the fact that the relationship between caffeine consumption and headache is a more immediate one.
Sleep problems and caffeine consumption were found to be predictors of subsequent headache and thus provide a potential opportunity to reduce headache occurrence, particularly in view of the high levels of caffeine consumption in the general population. Low levels of anxiety, depression, sleep problems and the absence of other pain were influences on recovery from headache, and eliminating or reducing levels of these factors in current sufferers may lead to recovery.
Headache can cause disability and result in time off work and thus is a considerable public health problem. The strong associations of headache with sleep problems, heavy caffeine consumption and anxiety raise specific challenges for preventative policies. For secondary prevention, such factors should be considered in consultations for headache and these problems addressed together with other help for headaches. However, at a societal level, the high levels of sleep disturbance and stress carry a range of potential negative effects on health, among which headache is likely to be one of the most common. The results presented here may suggest the need for an intervention which could result in an important, but somewhat unexpected additional benefit, namely that reducing sleep disturbances and anxiety may lead to reductions in headache frequency and disability.
Acknowledgements
We thank the North Staffordshire GP Research Network for their assistance with the study. We also thank the network team and administrative staff of the Primary Care Sciences Research Centre and administrative staff of the Department of Medicines Management, Keele University, for their help and support with the study. Baseline survey costs were funded by the Proprietary Association of Great Britain and the costs of the follow-up surveys were funded by the North Staffordshire Primary Care Research Consortium.