
Abstract

The occurrence of abnormal movements during some migraine attacks has long been recognized but has seldom been reported (1–3). In fact, the appearance of abnormal movements is not included among the potential features of migraine attacks in the International Headache Society classification (4). Recently, the case of a woman having repeated episodes of concurrent hemifacial spasm (HFS) and migraine has been reported (5). We also describe here a patient with unilateral migraine associated with ipsilateral HFS and provide some additional findings that might point to possible pathophysiological mechanisms.
Case report
A 35-year-old woman began having episodes of headache at age 18. Her past medical history was not relevant, but there was a positive family history of migraine in first-degree relatives (mother and brother); otherwise, no abnormal movements had been recorded in her family. Headache episodes had migraine features (pulsating quality, severe intensity, photophobia, phonophobia and nausea) and were strictly left-sided. They always started in the left ocular region and extended progressively to the entire left hemicranium. The attacks of left-sided headache lasted for one to several hours and were responsive to common analgesics, although they were followed by ipsilateral cutaneous allodynia and a moderate occipital pain of pressing quality that lasted up to 3 days. Headache attacks recurred with a frequency of two to four per month and were often precipitated by emotional stress. She had never been on prophylactic treatment for migraine. Since she had begun having migraine, most attacks of left hemicrania—invariably all those attacks with the most severe pain—had been accompanied by involuntary twitching of the ipsilateral facial muscles. When headache pain reached maximum intensity, her left eyelid started to develop rapid movements that made the eye close, sometimes extending to all ipsilateral facial muscles with pulling of the cheek and elevation of the mouth corner. These symptoms were not associated with diplopia, nor with conjunctival injection or lacrimation. The twitches usually persisted for 30–60 min and normally abated when the intensity of headache started to reduce. There were no spontaneous twitches in the absence of headache. She had had no prior facial palsy or facial numbness.
Between attacks, the examination did not disclose any neurological deficit. However, on three different occasions separated by 2-week intervals the compression of the left trochlear area evoked both ipsilateral referred pain and ipsilateral facial movements. The pain appeared when compression was maintained for approximately 30 s and increased with contraction (downward-medial gaze) and stretching (upward-lateral gaze) of the superior oblique muscle (6). It was perceived in the retro-orbital and supraorbital regions and was described as moderate and tightening. The motor response appeared once the pain had reached maximum intensity and persisted for 2–4 min after the compression was withdrawn. It consisted of clonic jerks of the orbicularis oculi starting in the inner part and rapidly spreading to the whole muscle. On one occasion there was a clear progression downwards, until twitching of the entire left hemifacies and the left platysma was observed. The patient recognized these contractions as identical to those usually appearing during migraine episodes.
An electromyogram (EMG) of the left facial muscles and a motor conduction study of the left facial nerve were normal. Blink reflexes were also normal on both sides. Nevertheless, on two different occasions a repetitive electric stimulus of the left supraorbital nerve (headache side) induced involuntary movements in the left hemifacies. This motor activity was equal to that previously provoked by trochlear compression. At this point it could be recorded with needle electrodes in three different muscles and was consistent with HFS. It consisted of clonic and arrythmic contractions, occurring with a frequency of two to four per second and lasting 100–500 ms. The bursts of muscle activity started in the left orbicularis oculi and spread progressively to the left platysma and the left orbicularis oris until the three muscles contracted synchronously (Fig. 1). This activity continued after the electric stimulus had stopped and persisted for more than 2 min. A consensual response on the right side was not present. On the other hand, no involuntary movements were elicited by electric stimulation of the right supraorbital nerve (non-headache side). Wake-state and sleep EEG recordings, magnetic resonance imaging of the orbit and the brain and a magnetic resonance angiogram of the cerebral vessels revealed no abnormalities.
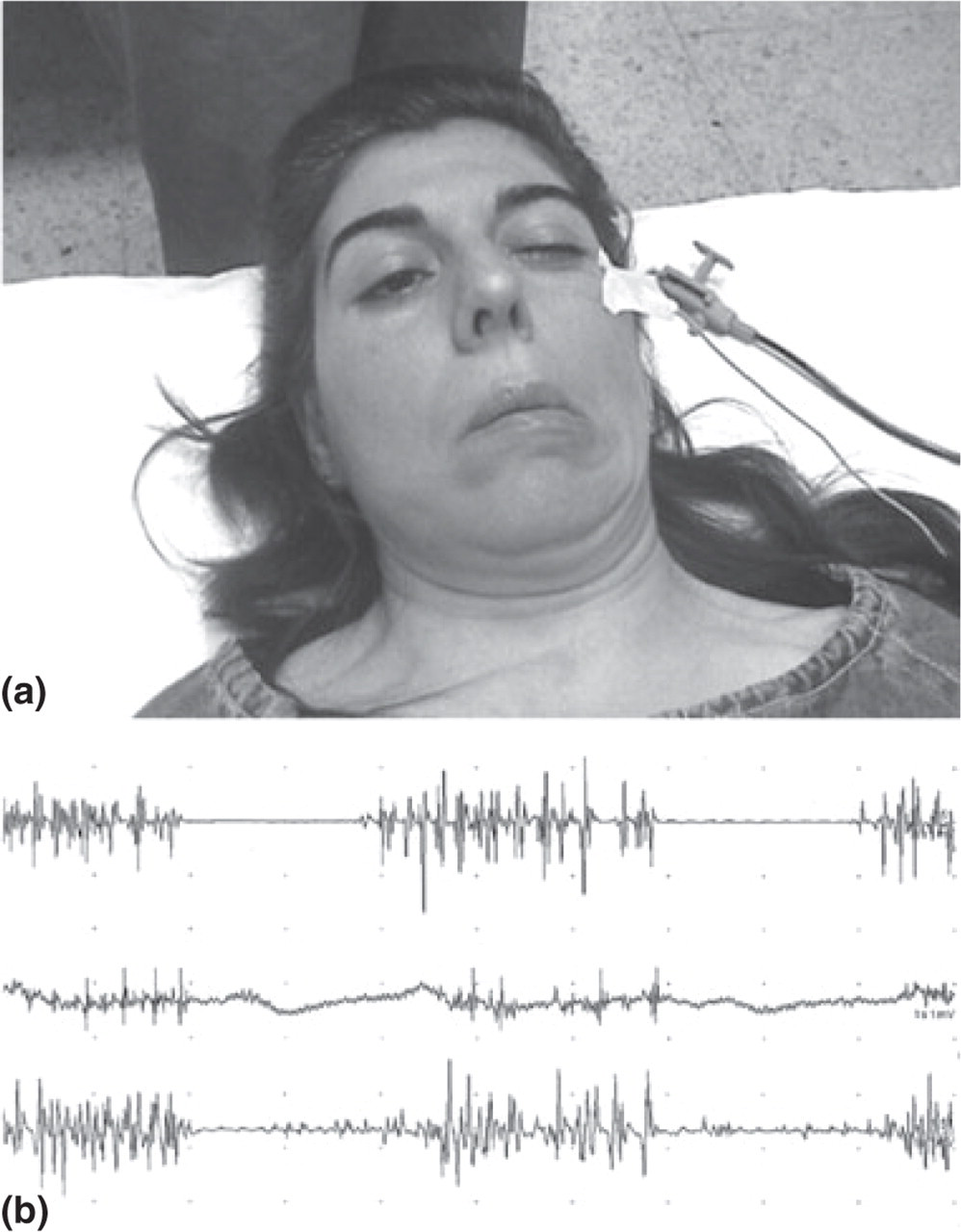
(a) Left hemifacial spasm induced by repetitive electrical stimuli of the left supraorbital nerve. The spasms became visible after 1 min and persisted for >2 min. They resembled the involuntary twitches that the patient usually experienced during ipsilateral migraine attacks. (b) EMG recording of the spasms appearing in the left orbicularis oculi (top), the left orbicularis oris (middle) and the left platysma (bottom).
Discussion
At least two patients with concurrent HFS and ipsilateral migraine have been observed: that reported by Husid (5) and the one reported here. A pathophysiological link rather than a coincidental co-occurrence seems likely, since both phenomena have been coupled for many years in each patient. Yet, the relationship between HFS and migraine is unknown. It is hardly conceivable that facial spasms represent an aura with positive symptoms, as they never precede the onset of headache and usually start once headache peaks. Indeed, migraine headache seems to be a trigger for HFS in both patients. A potentiation of certain trigeminofacial reflexes may possibly account for the appearance of facial spasms during migraine attacks. The incoming nociceptive impulses converging on the trigeminal nucleus caudalis could result in temporal and spatial summation, thus leading to increased activation of the trigeminofacial connections within the brainstem. A temporary enhancement of blink reflexes during acute migraine headache has in fact already been demonstrated (7). Our findings support this hypothesis, since we have elicited the same facial movements by both nociceptive and electrical stimuli within the V-1 region. Whatever may be connecting HFS and migraine, ‘spasmodic migraine’ might be eventually regarded as a new variant of migraine. Further research is needed and more cases should be found.