
Abstract
Cerebral venous thrombosis (CVT) has a large spectrum of clinical manifestations. Headache is the most frequent symptom of CVT and occurs in 70–90% of cases (1). The four main patterns of presentation are: headache with isolated intracranial hypertension, headache with focal signs, subacute encephalopathy and cavernous sinus thrombosis (2, 3). Unusual presentations have been reported in the literature. These include sudden, severe headache associated with evidence of a subarachnoid haemorrhage, postdural puncture headache, thunderclap headache and symptoms of migraine with and without aura (2, 4–7). We present two cases of CVT who presented with cluster headache symptoms.
Case reports
Case 1
A 47-year-old male had the onset of severe, sharp right-sided cluster headaches 9 years prior to presentation. Headaches initially occurred one to four times per day. The pain reached maximum severity in 5 min and lasted 30–120 min. Headaches were associated with ipsilateral ptosis, nausea and photophobia. Indomethacin, 100% oxygen at 12 l/min, valproic acid and propranolol were tried without success. Acute relief was obtained with sumatriptan nasal spray. Lithium carbonate and prednisone initially decreased the severity of his attacks.
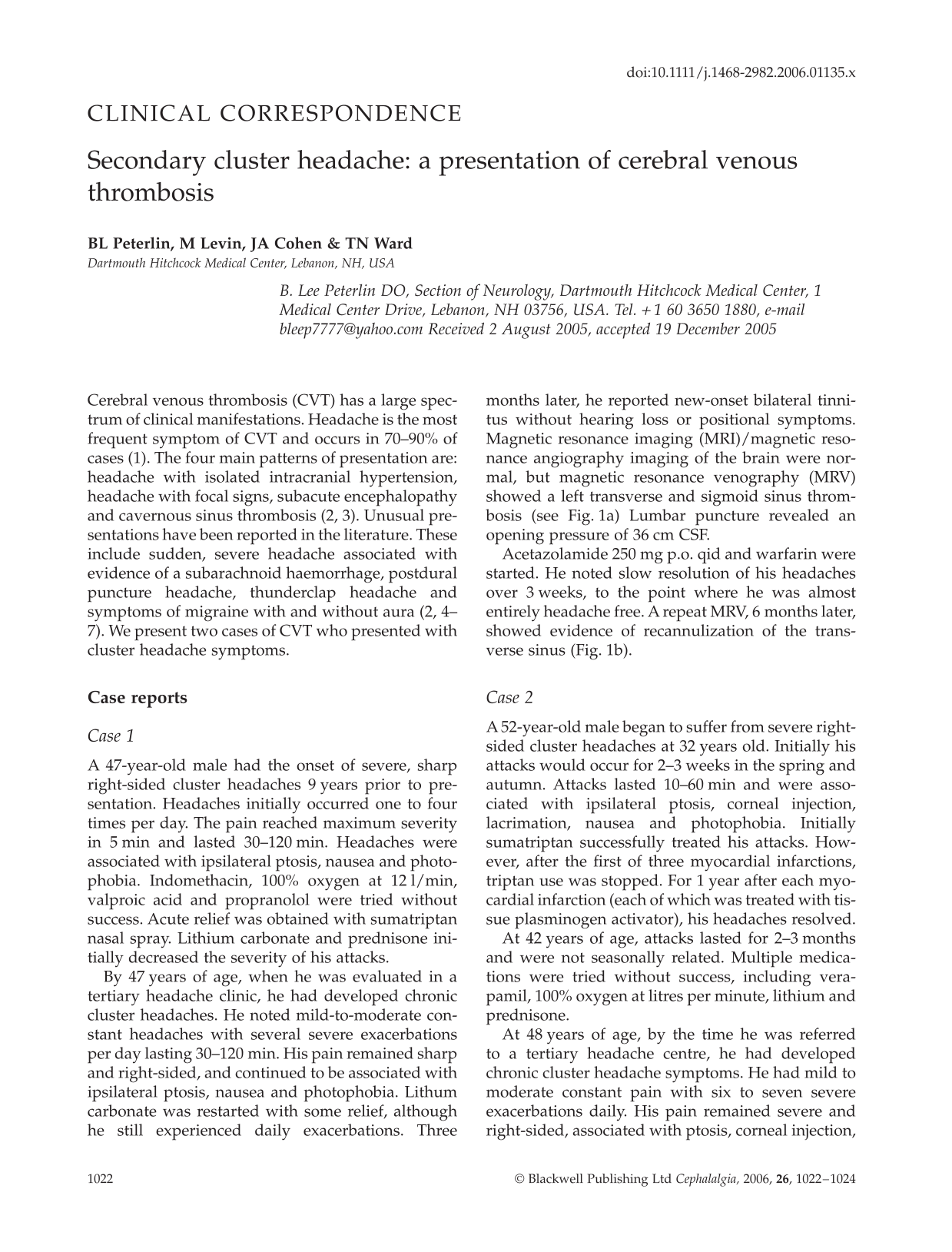
By 47 years of age, when he was evaluated in a tertiary headache clinic, he had developed chronic cluster headaches. He noted mild-to-moderate constant headaches with several severe exacerbations per day lasting 30–120 min. His pain remained sharp and right-sided, and continued to be associated with ipsilateral ptosis, nausea and photophobia. Lithum carbonate was restarted with some relief, although he still experienced daily exacerbations. Three months later, he reported new-onset bilateral tinnitus without hearing loss or positional symptoms. Magnetic resonance imaging (MRI)/magnetic resonance angiography imaging of the brain were normal, but magnetic resonance venography (MRV) showed a left transverse and sigmoid sinus thrombosis (see Fig. 1a) Lumbar puncture revealed an opening pressure of 36 cm CSF.
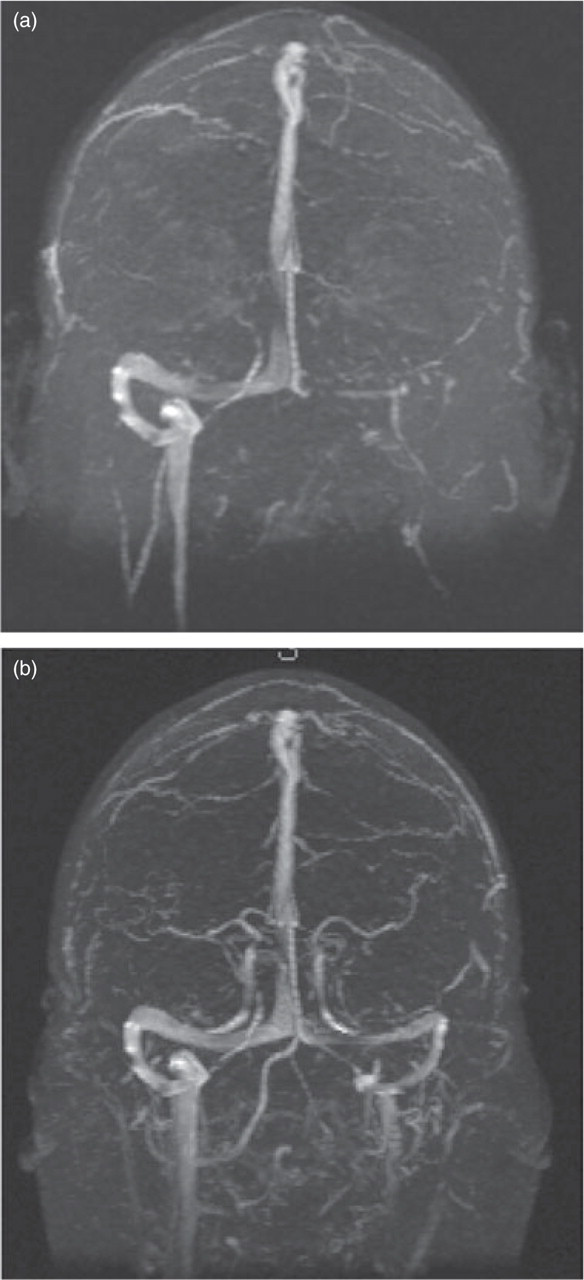
Magnetic resonance imaging of patient in case 1, demonstrating absence of the left transverse and sigmoid sinus (a) and recannulization of the left transverse and sigmoid sinus (b).
Acetazolamide 250 mg p.o. qid and warfarin were started. He noted slow resolution of his headaches over 3 weeks, to the point where he was almost entirely headache free. A repeat MRV, 6 months later, showed evidence of recannulization of the transverse sinus (Fig. 1b).
Case 2
A 52-year-old male began to suffer from severe right-sided cluster headaches at 32 years old. Initially his attacks would occur for 2–3 weeks in the spring and autumn. Attacks lasted 10–60 min and were associated with ipsilateral ptosis, corneal injection, lacrimation, nausea and photophobia. Initially sumatriptan successfully treated his attacks. However, after the first of three myocardial infarctions, triptan use was stopped. For 1 year after each myocardial infarction (each of which was treated with tissue plasminogen activator), his headaches resolved.
At 42 years of age, attacks lasted for 2–3 months and were not seasonally related. Multiple medications were tried without success, including verapamil, 100% oxygen at litres per minute, lithium and prednisone.
At 48 years of age, by the time he was referred to a tertiary headache centre, he had developed chronic cluster headache symptoms. He had mild to moderate constant pain with six to seven severe exacerbations daily. His pain remained severe and right-sided, associated with ptosis, corneal injection, lacrimation, nausea and photophobia. Verapamil was restarted for prophylaxis. Although he noted initial improvement, the verapamil dosage had to be escalated and ultimately became ineffective. He obtained relief with transnasal butorphanol. MRI of the brain showed several small subcortical white matter lesions. MRV revealed a left transverse sinus, sigmoid and internal jugular vein thrombosis. Lumbar puncture revealed an opening pressure of 20 cm CSF.
Acetazolamide 250 mg tid and warfarin were started. For the next 24 h he was headache free. Over the next week he had only two to three mild attacks per day. His acetazolamide was increased to 500 mg p.o. bid and he became headache free for 3 days. Over the next week he noted only two mild attacks. He died from a massive myocardial infarction 1 month later and repeat MRV imaging was not obtainable.
Discussion
Headache is commonly seen in CVT and may be due to the causes or consequences of venous occlusion (3). Cluster headache has not been described before as a presenting syndrome of CVT. Our cases suggest that CVT in some way may lead to cluster headache symptoms. It is not clear whether this is the primary aetiology for our patients’ headaches or not. If so, the CVT process would have had to be chronic and productive of little other than headache symptoms for many years. This is not inconceivable, as the development of CVT has been described as an ongoing process in which the balance of prothrombotic and thrombolytic processes is disturbed (1). Alternatively, our patients may have had primary cluster headache which was stimulated by CVT in some fashion.
Recent studies have implicated the posterior hypothalamic grey matter as the potential generator of cluster headache (3). With our patients this raises the question, is it possible that elevated and/or fluctuating intracranial pressure may affect the hypothalamus? Or, as CVT has been known to lead to infarction (1), is it possible that our patients had non-imageable ischaemia of the hypothalamus?
Alternatively, could our patients’ headaches be due to irritation of the intracavernous portions of the trigeminal nerve by local venous engorgement in the cavernous sinus? Finally, it is possible that both of our patients had both cluster headaches and CVT, unrelated to each other. However, the significant response of our patients’ headaches to treatment for CVT seems to suggest a stronger correlation.
Conclusion
Although there are typical patterns of presentations of CVT, the presentation can be quite heterogeneous. Our cases suggest that there may be a factor present in CVT that may induce or exacerbate cluster headache pathophysiology. Additionally, in patients with chronic cluster, a diagnosis of CVT should be considered.