
Abstract
The epidemiological and clinical literature identifies strong associations between adult headache, cervical and thoracic spine dysfunction and spinal posture. This paper reports on the prevalence and incidence of headache, neck and upper back pain which occurred in the previous week, in urban Australians aged 13–17 years. Commencing in 1999, we followed a cohort of South Australian students through 5 years of secondary schooling. Of our commencing cohort of students, 132 (30±) provided data on bodily pain every year. For both girls and boys, there was a significantly decreasing prevalence of headache over the study period, while neck pain and upper back pain increased. There was a significantly increasing trend over time for boys with upper back pain. Twenty percent of girls and boys consistently reported headache, neck pain or upper back pain over 5 years. The progression of early adolescent headaches to mid-adolescent neck and upper back pain potentially reflects the adolescents’ biomechanical responses to intrinsic and extrinsic imposts. This requires further investigation to understand the causes of adolescent headache, neck and upper thoracic pain.
Introduction
Adolescent headache has attracted a large body of research around the world in the past decade. Adolescents are defined as being between 13 and 18 years, a time period which encompasses the spurt in adolescent growth (1). The epidemiological and clinical literature identifies strong associations between adult headache, cervical and thoracic spine dysfunction and spinal posture (2–4), therefore it is plausible that adolescent headache may well be associated with pain in the neck and/or upper back and with both internal and external factors. Internal factors include hormonal influences, growth factors, diet and hydration, fatigue, standing and sitting posture, psychosocial and behavioural issues, while external factors could include load carriage, furniture use and sports participation (5–7). It is also plausible that regularly experiencing headache may predispose adolescents to experiencing pain in the neck or upper back with the passage of time, reflecting symptomatic adaptations associated with posture, biomechanics and pain pathways (8, 9).
Approximately half of the comparative literature on adolescent headache (sourced as background for this paper) specifically examined migraine headaches (typified by a headache description or specific medication use), whilst the remainder dealt variably with tension-type and ‘any’ headache, with or without concurrent neck pain included in headache descriptions. No paper described headache as a correlate of neck and upper back pain or charted its frequency related to pain over time in these areas. The majority of studies were cross-sectional and there are no Australian longitudinal studies that describe adolescent headache, neck or upper back pain occurrence. We also found a range of time frames over which headache occurrence was collected and ways in which headache were described were not standard. Eleven studies relevant or comparable to the research reported in this paper were identified, reporting on frequency of headaches of any aetiology occurring ‘in the past week’. The comparison research comprised nine cross-sectional studies (10–18) and five longitudinal studies (19–23). Table 1 presents an overview of the comparison literature. There was only one study (10) that examined the 1-week (31.4%) and point prevalence (8.9%) of adolescent headache. The remaining studies reported the prevalence of weekly, or at least weekly, headaches over the previous 6 or 12 months. The prevalence of weekly adolescent headache ranged from 5.4% (in 6-year-olds) to 38% (in 12-year-olds) (16). In general, the research reported increasing prevalence of headaches with increasing age. No reports of associated prevalence of neck and upper back pain were found.
Comparison of adolescent headache prevalence studies (the most relevant study is in bold)

HA, Headache; ES, elementary school; HS, high school.
This paper reports on the prevalence and incidence of headache, neck and upper back pain which occurred in the previous week, in each of five consecutive years of measurement of urban Australian adolescents from the period between 13 and 17 years of age.
Methods
The study had ethics approval from the relevant education and research institutions. Parents and students provided written consent to participate each year.
The study began in 1999, enrolling healthy consenting 13-year-olds (average age) entering the first year of high (secondary) school in metropolitan Adelaide, South Australia (year 8). No secondary school in this study enrolled adolescents with intellectual disabilities. Any enrolled student, irrespective of physical disability, was eligible for inclusion in the study provided that they and their parents consented to participate. Students were not excluded if they suffered severe illness or surgical procedures during the study period, although recent illness or injury were noted each year and taken into account during analysis. Four randomly selected metropolitan schools agreed to participate, providing access to a total of 526 eligible students who reflected the range of socioeconomic status of urban Adelaide (South Australian) adolescents.
Each year in March (1999–2003) data were collected during the school day on the school premises. Students were released from class to participate. In the final year of the study students completed their secondary schooling (year 12) (aged on average 17 years). Over 200 objective and subjective measures were collected each year. The objective measures included anthropometry, school bag weight and dimensions, motor control and planning, muscle strength and endurance, posture and flexibility, while subjective measures included participation in physical activity, time spent sitting and screen watching, reports of pain and self-image. This paper describes headache, neck pain and upper back pain in relation to age and gender. Other papers are in preparation to explore other study measures.
Relevant to this paper, any pain experienced ‘in the previous week’ was recorded by students on a body chart in a questionnaire. This paper reports only on headache, neck pain and upper back pain. Headache refers to pain experienced at the front or back of the head. Neck pain refers to the cervical spine and upper trapezium region on posterior body chart view, and upper back pain is pain experienced in the thoracic spine to the edge of the ribs on posterior body chart view. Pain reported in the shoulders or the lower back was specifically excluded from the analysis.
Data handling and statistical analysis were undertaken using SAS Version 8.2, SAS Institute Inc (2006). Prevalence was calculated as the percentage of subjects in each year reporting pain in these sites. Incidence was calculated as the number of new cases of headache, neck or upper back pain reported after the first year of the study (from 2000 to 2003). As an example, subjects who reported headache in 1999, but not neck pain, would have been considered as new cases (incidence of neck pain) if they reported neck pain for the first time in one of the following years of the study. Students who reported no headache in 1999 would have been considered as new cases (headache incidence) if they reported this symptom for the first time in the following years of the study.
This paper reports on the subset of students who provided bodily pain data in every one of the 5 years of the study (1999–2003). Thus, the sample has no missing data.
Results
Data were collected initially [first study year (1999)] from 436 adolescents, reflecting 83% of the eligible cohort. Not all students who enrolled in 1999 completed the study 5 years later. A number of adolescent subsets were identified within our sample, e.g. students who provided data consecutively for 3 years from 1999 to 2001 and then left high school to enter the workforce, students who provided only 2, 3 or 4 years’ data because they were absent on a day of testing, or students (or parents) who withdrew permission to participate during the study period. Moreover, not every student completed every study measurement, as, with our ethical constraints, students could choose not to participate in any aspect of the study in any 1 year.
Of the 1999 cohort, 132 students (30%) provided data on bodily pain every year (five yearly observations), providing 660 total observations for this subset of subjects [60 girls (300 observations) and 72 boys (360 observations)]. On average, these students were aged 13 years in 1999, 14 years in 2000, 15 years in 2001, 16 years in 2002 and 17 years in 2003. In each year the variability in age was the same (SD 1.6 years).
No severe illnesses or surgical procedures were reported during the study period, therefore no data were flagged for specific disability subgroup analysis. Usual recent illnesses and surgery involved colds, stomach upsets, broken bones and appendicitis.
Table 2 shows the prevalence of any bodily pain experienced in the previous week for each of the years of the study. There was considerable variability in year-by-year reporting, and neither boys nor girls in this sample demonstrated a significantly increasing prevalence trend over time. The percentage of bodily pain that was accounted for by headache, neck pain and upper back pain is reported in Table 3, where similar reporting patterns were observed for boys and girls. There was a decreasing percentage of headache reports after age 14 years, whilst there were increasing reports of neck pain and upper back pain after this time.
Yearly prevalence of any bodily pain

The contribution of headache (HA), neck pain (NP) and upper back pain (UBP) to reports of ‘any bodily pain’

The prevalence of headache, neck pain and upper back pain each year is reported for girls and boys in Fig. 1. There was a significantly decreasing headache prevalence over the study period for both girls and boys (χ2 for trend, respectively, 15.1, P < 0.01; and 11.2, P < 0.01). There were conversely increasing trends in neck pain and upper back pain for both girls and boys, although the only significant increasing trend over time was for boys with upper back pain (χ2 for trend 8.5; P < 0.05).

Prevalence of headache, neck and upper back pain (UBP) for boys and girls over the study period.
For both girls and boys, the odds were protective of suffering headache at 17 years old compared with when subjects were in the first study year (age 13 years). For girls the odds were significant [odds ratio (OR) 0.15, 95% confidence interval (CI) 0.1, 0.6], although not for boys (OR 0.3, 95% CI 0.1, 1.2). There was a non-significant risk of suffering neck pain as a 17-year-old compared with when subjects were aged 13 years for both girls (OR 2.5, 95% CI 0.5, 13.0) and boys (OR 2.1, 95% CI 0.5, 8.9). There was an increased risk of suffering upper back pain as a 17-year-old compared with when subjects were aged 13 years for both girls and boys, with significant risk for boys (OR 6.3, 95% CI 1.2, 43.0) but not for girls (OR 2.8, 95% CI 0.7, 11.4). The prevalence of headache over the entire (5-year) study period (on 660 observations) was 15.0% for girls and 9.2% for boys. The overall prevalence of neck pain was 11.3% for girls and 5.5% for boys, and for upper back pain it was 12.3% for girls and 7.8% for boys.
Headache was reported each year as occurring relatively similarly in the front and back of the head, by both boys and girls. Pain locations are often used to describe the possible causation of headache (i.e. migraine, tension-type, cervicogenic) (2, 3); however, in this study we classified both these pain sites as ‘any headache’ and we did not seek to identify headache by type or attribute causation or aetiology.
The incidence (new episodes) of headache for girls and boys identified only a small number of new headache sufferers after the second year of the study, with 100% of the new cases for girls and 75% of the new cases for boys occurring in the second study year. In each of the remaining 3 years of the study for boys, new headache sufferers comprised only 8.3% of all headaches reported.
Over the last 4 years of the study, when students were aged 14–17 years, the incidence of neck pain and upper back pain provided gender-specific characteristics. Girls showed an increasing incidence (new cases) of neck pain but a decreasing incidence of upper back pain, whilst for boys, the 14-year-olds demonstrated the greatest incidence of neck pain, while the incidence of upper back pain generally increased over the study period. The annual incidence (new cases) of neck pain and upper back pain for boys and girls from the age of 14 years is illustrated in Fig. 2.

Incidence (new cases) of neck (NP) and upper back pain (UBP) after 1999.
The percentage of subjects who consistently reported no pain over the entire period of the study is illustrated in Fig. 3 using a survival analysis graph. The percentage of girls and boys reporting no pain at age 13 years was similar (difference of 6.1%). The percentage of girls who continued to report no headache, neck or upper back pain decreased by the greatest amount in 2000 (age 14 years) and remained lower than the boys for the rest of the study. Girls were less likely than boys not to report headache, neck pain or upper back pain at any age (13 years OR 0.7, 95% CI 0.3, 1.7; 14 years OR 0.5, 95% CI 0.2, 1.1; 15 years OR 0.6, 95% CI 0.3, 1.3; 16 years OR 0.6, 95% CI 0.3, 1.2; 17 years OR 0.6, 95% CI 0.3, 1.3). However, none of these differences was significant.

The percentage of boys and girls who consistently reported no headache, neck pain or upper back pain over the period of the study.
Headache, neck pain and upper back pain did not always occur independently. Over the 5 years of the study, 16% of the total girls’ responses and 8% of total boys’ responses involved two or more sites of pain. Girls were 2.3 times more likely than boys to suffer two or more sites of pain involving head, neck or upper back over the entire study period (OR 2.3, 95% CI 1.1, 4.6). For girls, there was an increasing prevalence over the study period for neck pain and upper back pain to occur together, while for boys, pain in both these areas was reported only by the 16- and 17-year-olds. The prevalence of reporting of two or three sites of pain (headache, neck and upper back pain) in each year is reported in Table 4.
Prevalence of reporting two or more sites of pain
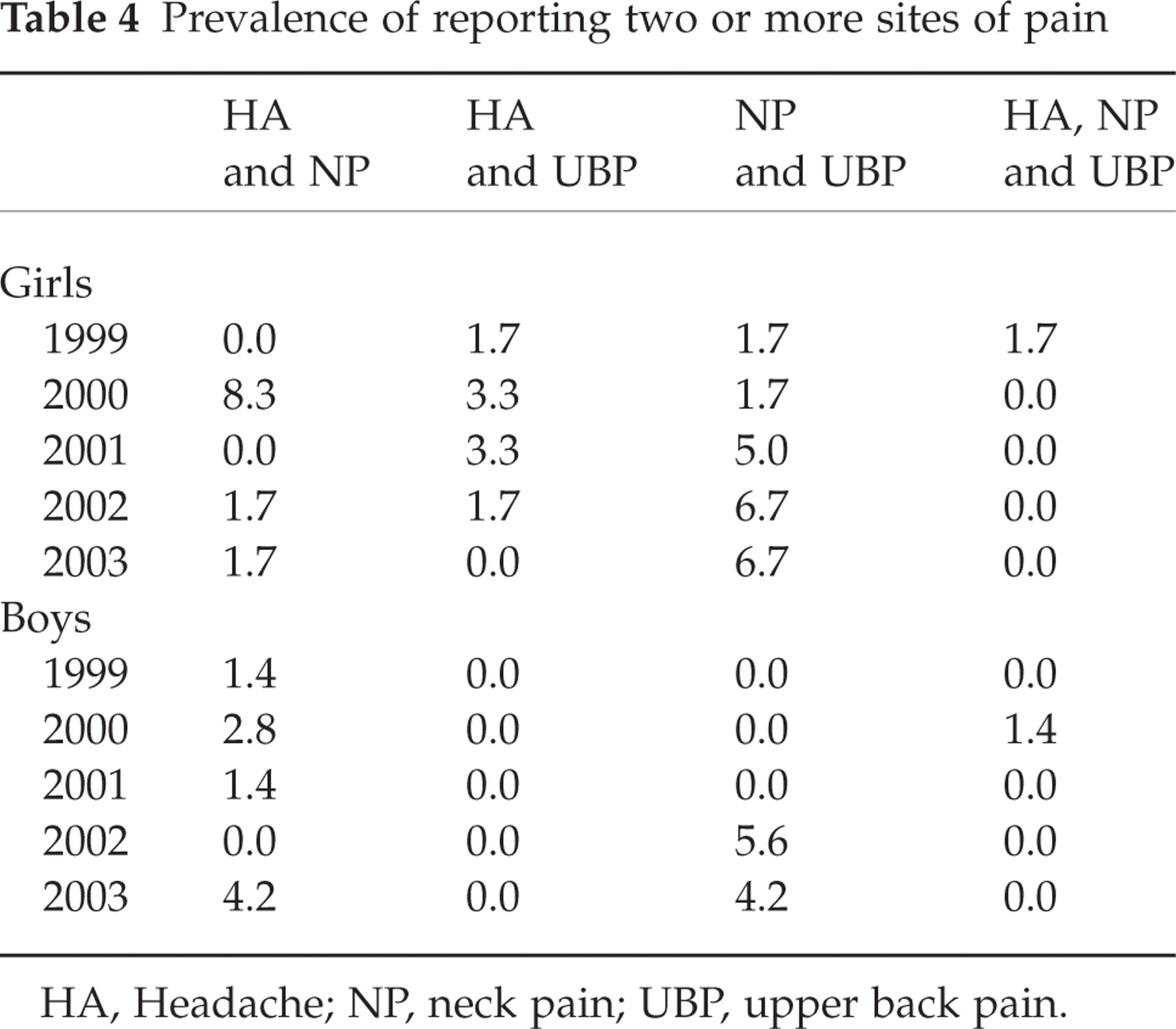
HA, Headache; NP, neck pain; UBP, upper back pain.
The number of students in each year reporting two or three sites of head, neck and upper back pain is reported in Fig. 4. A higher proportion of girls than boys reported multiple sites in pain in all but the final year of the study. However the prevalence of multiple sites for girls decreased after the age of 14 years, whilst the prevalence of multiple sites for boys generally increased over that study period.

Percentage of girls (h) and boys (s) who reported two or more sites of pain each year.
Of note, every subject who reported headache at age 13 years (13 girls, 11 boys) reported at least one other episode of headache, neck and/or upper back pain during the next 4 years. The per-person-year counts of pain (headache, neck and upper back pain) were considered as a percentage of the number of subjects and illustrated in Fig. 5, indicating an increase at age 14 for both genders, a decrease at age 15, and a steady rise thereafter. We undertook this analytical approach because headache related to cervical dysfunction (as in tension-type or cervicogenic headache) can often incorporate neck or upper back pain (2). To explore further the phenomenon of multiple sites of pain potentially related to the one biological aetiology, a cumulative count of headache, neck and upper back pain reports over the study period was calculated. Due to its abnormal distribution, this count was transformed into log values for statistical analysis. Table 5 reports the log transformed mean values (SD). Gender differences from paired Student t-tests were significant for the 14- and 15-year-olds (P < 0.01) (∗). In any 1 year the maximum non-transformed score was 3 and the minimum score was 0.
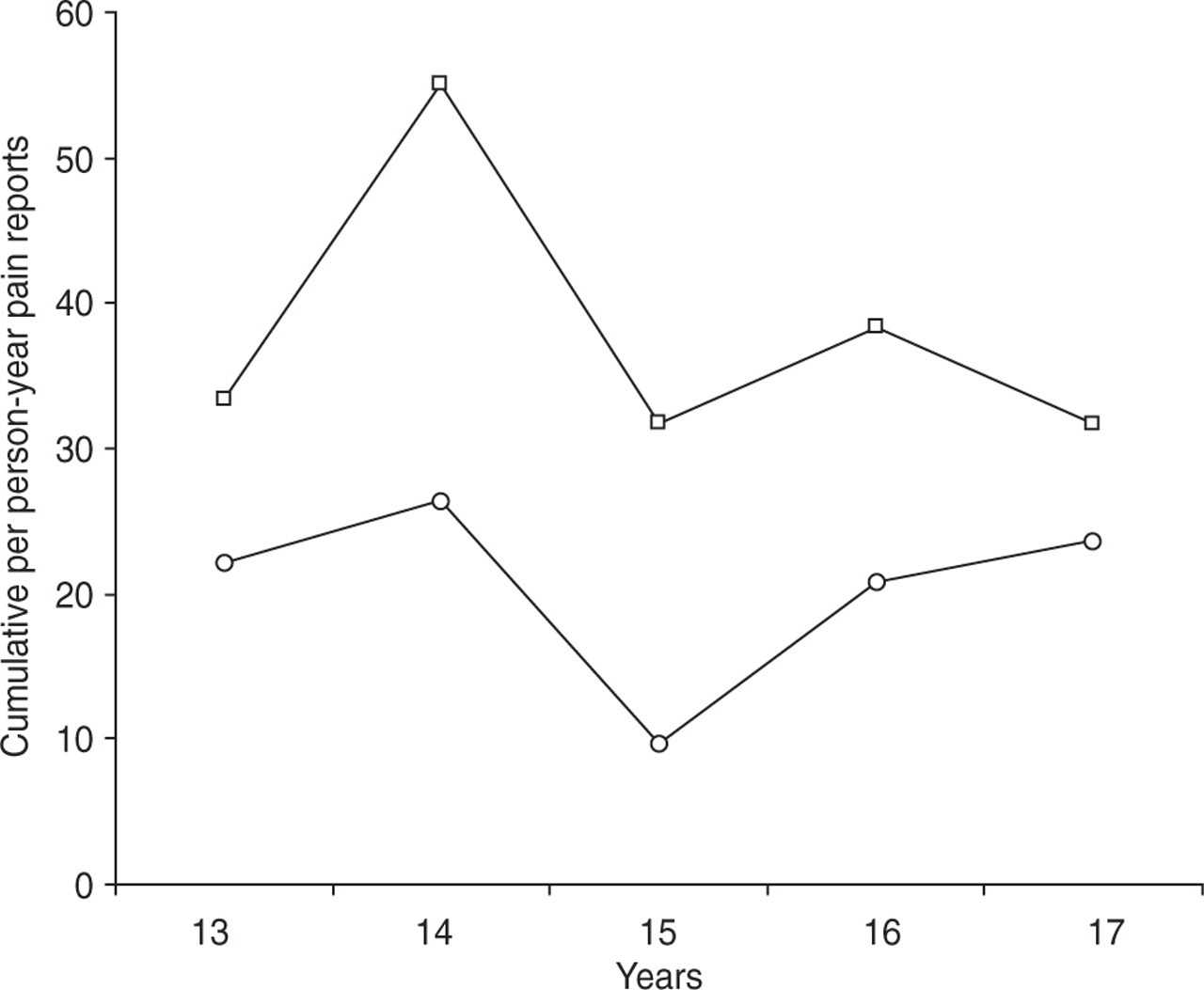
Cumulative per person-year headache, neck and upper back pain reports (total number of pain reports as a proportion of the sample of girls and boys each year).
Mean (transformed) cumulative score of headache, neck pain and upper back pain

Indicates significance.
On testing the hypothesis that suffering headache in the first year of the study sensitized students to ongoing pain in the upper cervical spine region, we found that the 13-year-olds who reported headache in the first year of the study did not have significantly elevated risk of experiencing headache, neck or upper back pain when aged 17 years, compared with the 13-year-old students who did not report headache (boys OR 1.4, 95% CI 0.5, 4.26; girls OR 1.8, 95% CI 0.6, 5.3). However, for a subset of students, their 13-year-old experiences of headache appeared to manifest as ongoing pain experiences in head, neck or upper back, and thus from a clinical perspective this group was explored further.
Of the 13 girls reporting headache at age 13 years (21.6% of the total number of girls in the study), 53.8% reported headache in the following year (at age 14 years) and 15.3% reported neck pain. Of the initial group of 13-year-old headache sufferers, three (23%) continued to report headache at age 15 years, with a further three (23%) reporting neck pain or upper back pain. Two of these students reported pain in more than one site. At age 16 years, 30.7% of the initial sample of female headache sufferers reported headache and 38.5% of this sample reported suffering neck pain or upper back pain. Four of this subset overlapped (reported more than one pain site). In the final year of the study (age 17 years), headache was reported by one (8%) of the initial sample of female headache sufferers, whilst neck or upper back pain was reported by 23% of the initial sample, with two girls reporting multiple pain sites. Of the 17 girls who reported headache, neck or upper back pain when aged 13 years (28.3% of the total sample), one reported pain every year (6% of the initial headache, neck or upper back pain sufferers), five reported pain in four of the 5 years (29.1%) and three reported pain in three of 5 years (35.3%). Overall, 15 of the 17 girls who reported headache, neck or upper back pain in the first year of testing experienced pain of this nature at least twice over the 5-year study period.
Of the 11 boys in the initial sample who reported headache (15.3% of the total number of boys in the study), four (36.4%) reported headache in the following year (aged 14 years) and a further two boys in this year reported neck or upper back pain (18.2%) (one of these overlapping both groups). At age 15 years, one of the initial male headache sufferers continued to report headache (9.1%) and two of this group (including the headache sufferer) (18.2%) reported neck pain. While no boy who initially reported headache at age 13 reported ongoing headache at age 16 or 17 years, three of the initial headache sufferers when aged 16 years reported pain in both neck and upper back (27.3%) and four of them reported neck or upper back pain when aged 17 years (two reporting both sites). Of the 16 boys who reported headache, neck or upper back pain when aged 13 years (22.2% of the sample), one reported pain every year (6% of the initial headache, neck or upper back pain sufferers), four reported pain in four of the 5 years (25%) and three reported pain in three of 5 years (18.7%). Ten of the 16 boys who reported headache, neck or upper back pain in the first year of testing experienced pain of this nature at least twice in the 5-year study period.
Discussion
This paper presents rare longitudinal prevalence and incidence data on headache, neck and upper back pain experienced in the previous week by a sample of generally healthy young Australians over five consecutive years (from early to late adolescence). It presents an intriguing picture of decreasing headache prevalence and incidence over the 5-year period, with a concomitant increase in neck and upper back pain over this period. The sample is not constrained by missing data and therefore provides a robust longitudinal snapshot of adolescent headache, neck and upper back pain experiences. No comparative research from anywhere in the world has examined headache in combination with these two pain sites.
This study confirms that bodily pain in any site was experienced in the previous week by over half the adolescent sample each year. The contribution of headache to any report of bodily pain was high in the first 2 years of the study, whilst in the final 3 years neck and upper back pain reports increased to contribute up to 30% of bodily pain reports. This finding suggests that many adolescents are not pain free in a usual week and it highlights the need to understand further what pain experiences in adolescents mean for their healthy physical and psychological maturation into adulthood.
Our headache prevalence data are marginally higher than any other reports of headache for 13- and 14-year-olds in the comparison studies (see Table 1), although consistently across studies more girls than boys reported headaches. The time frame of data collection for the comparison studies differed from the one used in our study, which potentially contributes to our higher prevalence figures. Most studies collected information over the past 6 months or year, specifically in relation to headache frequency (not occurrence). The term ‘at least weekly’ was often used to describe frequent headaches, which is a different measure than weekly prevalence, or pain experienced in the previous week. Not only could recall over 6 months or a year be likely to be poorer than for the ‘last week’, but a focus on frequent headaches in the comparison studies (rather than any headache occurrence) would produce lower figures, as it potentially excludes subjects with occasional symptoms who do not perceive themselves as being frequent headache sufferers.
The lack of standardization in research reports regarding the most appropriate and sensitive time frame(s) for collection of information on headaches suggests the need for consensus before a clearer understanding can be reached of the social and occupational implications of adolescent pain. A limitation of our study is the lack of information collected in the first year (1999) on lifetime or 12-month prevalence, and in any year of the study regarding severity and frequency of headache. To capture this information would have required more intensive data, such as pain diaries, interviews or information on regular medication use, which was not feasible given our study time frames and constraints on access to subjects. An alternative approach, which would have required greater data collection time and specific consent, would be to examine physically each student each year to assess the neuromuscular integrity of their cervical and thoracic spines. These data would have assisted us to assess whether reports of pain were associated with neuromuscular dysfunction (2–9). To our knowledge, this investigation has not been reported longitudinally in a group of symptomatic and non-symptomatic adolescents. Given the consistent (two or more), headache, neck and upper back pain reports over the 5 years of the study by 19% of the total sample (15 girls and 10 boys), repeated information on the neuromuscular integrity of cervical and thoracic spine throughout the adolescent period would add much to international understanding of headache, neck and upper back pain causation and progression. However, such an examination would need to take account of day-to-day variability of symptom presentation and should consider the validity of proposed causal mechanisms of muscle tension, shortening and spasm, with associated postural changes, with pain (2–9).
The comparative literature highlights conflicting reports about adolescent headache. Some studies report a decrease in frequency of headache as young people aged (14), while others have found it increases for girls up to adult frequency by late adolescence (15). A marked increase in headache in the early teenage years has also been demonstrated, followed by a decrease in middle adolescence, then a steady rise into late adolescence, especially for girls (24). These findings highlight the importance of defining age ranges of data collection and understanding the underlying biological and environmental influences when reporting on adolescent pain. Our data collection commenced at an average age of 13 years, thus we were unable to capture prepubescent headache experiences, such as reported in the literature (10, 11, 16). Moreover, our study did not demonstrate an increase in headache frequency with older adolescence, perhaps indicating that we did not capture data for a sufficiently long period to demonstrate an established preadult headache pattern. Our dataset may thus have captured only a mid-adolescent decrease in headache prevalence reported by Sillanpaa et al. (24), and not the late adolescent headache patterns. However, late adolescent/early adult headache prevalence has been variably reported, with studies suffering from the same reporting anomalies as we identified in the adolescent research. There is also a lack of longitudinal research following adolescents into adulthood, making it difficult to establish a pattern of headache occurrence during this important transition phase. However, the cumulative count of headache, neck and upper back pain reports per person-year in our study indicates a pattern similar to that reported in the comparative studies, where pain peaks at early adolescence, declines in mid adolescence and then steadily rises.
The causes of headache in adolescence are complex (5, 6, 10–23). The literature suggests that early adolescent (13–14-year-old) headache reports may be strongly related to their social and structural environment (18–22). In Australia a dramatic change occurs for most 13-year-olds moving from primary school (one classroom for all subjects, a small number of text books and a controlled campus) to secondary school (a larger campus with multiple classrooms, carrying text books for up to eight lessons per day and use of a variety of school furniture and equipment). In particular, use of computers increases significantly in the Australian secondary school environment, so that postural imposts may also be challenging young spines which are in the throes of the adolescent growth spurt (1, 7).
Conclusion
This study suggests that bodily pain is a regular event for approximately 50% adolescents in any 1 year at secondary school. Boys and girls demonstrated similar patterns of behaviour. Headache prevalence was highest in early adolescence (13–14 years), after which it was infrequently reported; however, neck and upper back pain was increasingly reported in later adolescence. For approximately 20% of subjects (representing boys and girls equally), early adolescent headaches appeared to progress into mid-adolescent neck and upper back pain. Pain repeatedly experienced in the head, neck and upper back suggests sensitization of pain structures, potentially as a result of the adolescent body's biomechanical responses to intrinsic and extrinsic imposts. These findings require further investigation to understand the causes of abnormal adolescent pain patterns.