
Abstract
The authors report long-lasting airplane headache in a patient with non-allergic, chronic rhinosinusitis. Association of mucosal inflammation with compromised sinonasal ventilation and sinus barotrauma created a base for not only the pain but also for the prolongation of symptoms. Effective therapy with antihistamine and nasal decongestant supports the theory that sinonasal barotrauma plays a triggering role in the pathophysiology of airplane headache.
Introduction
Airplane headache is a newly introduced form of headache that appears during flights when the plane is landing or taking off. Its prevalence is not known and the underlying pathophysiology is uncertain, although sinonasal barotrauma has been proposed (1–3). Based on the few reported cases, airplane ascent- and descent-triggered headache is characterized by sudden onset, severe, mainly unilateral pain localized to the orbital, temporal, frontal, sometimes parietal and facial regions; the symptoms rarely last more than 1 h, and the pain is jabbing, stabbing, shooting, bursting, pressing, piercing and sharp in quality (1–6) Additional symptoms are rare, although unilateral tearing, nasal congestion and stuffy feeling of the face may be present (2–4). Physical examination, routine blood tests and head imaging studies are not specific (1–6).
Here, we present a new case, where the recurrent and prolonged headache attacks appeared during airplane landings in a patient with chronic rhinosinusitis. We also discuss the possible cause of the long pain duration and slow recovery.
Clinical history
A 27-year-old woman, a frequent flyer, had reported her first sudden-onset headache during commercial airplane descent 2 years before her neurological examination, after years of headache-free flights. The severe, bilateral headache (10/10 in intensity) developed in her cheek, ear, forehead, and on the top of the head. The pain was stabbing and pressing, later pulsating. There was only mild nausea without light and noise sensitivity. Aura and autonomic symptoms were not present. She had impaired hearing associated with tinnitus for 2 days. The pain remained severe until landing, then slowly diminished, but lasted for 2 weeks. Headaches on the next plane trips were identical in localization, intensity and quality. The pain lasted for at least 1 week in each case. She took different painkillers, including non-steroidal anti-inflammatory drugs just before departing and before descent without any relief. Subsequently, she noticed similar but less intense headaches on the subway, in tunnels, and during up- or downhill driving.
There was no chronic disorder or any other type of headache in her medical history. She was not on regular medication, and she did not smoke. Neurological examination was normal. Paranasal sinus computed tomography and 3-T brain magnetic resonance imaging (MRI) showed bilateral inflammation in the maxillary, sphenoid and ethmoid sinuses (Fig. 1A–C) [MRI: axial T2 turbo spin echo, repetition time (TR) 6000 ms, echo time (TE) 93 ms, echo train 18; coronal fluid-attenuated inversion recovery, TR 9000 ms, TE 93 ms, echo train 16; sagittal T1 gradient echo, TR 440 ms, TE 2.5 ms and diffusion-weighted apparent diffusion coefficient sequences, b = 0, b = 500, b = 1000 with 4 mm slice thickness performed by a Siemens Trio Tim 3.0-T MRI machine, Erlangen, Germany]. Routine blood tests revealed an increased number of eosinophilic cells repeatedly (8.3% and 9.8%), while allergen-specific immunoglobulin E (IgE) tests were negative. Nasal endoscopy indicated swelling of the nasal mucosa with tough and colourless exudates. The typical clinical symptoms and nasal endoscopic findings such as nasal obstruction and postnasal catarrh, negative allergy tests, and abnormal results of sinus imaging supported the diagnosis of chronic non-allergic rhinosinusitis. Treatment with oral levocetirizine (5 mg/day) and mometasone nasal spray (100 µg/day) was introduced, and subsequent flights were almost painless. Six months later, MRI was performed again and the images demonstrated mild regression of mucosal abnormalities in the paranasal sinuses. Blood tests did not show change in the slightly increased number of eosinophilic cells.
T2-weighted axial 3-T magnetic resonance images of a patient with airplane headache and chronic rhinosinusitis. The images show high signal intensity of the thickened mucosa in the maxillary (A), sphenoidal (B) and ethmoidal (C) sinuses on both sides.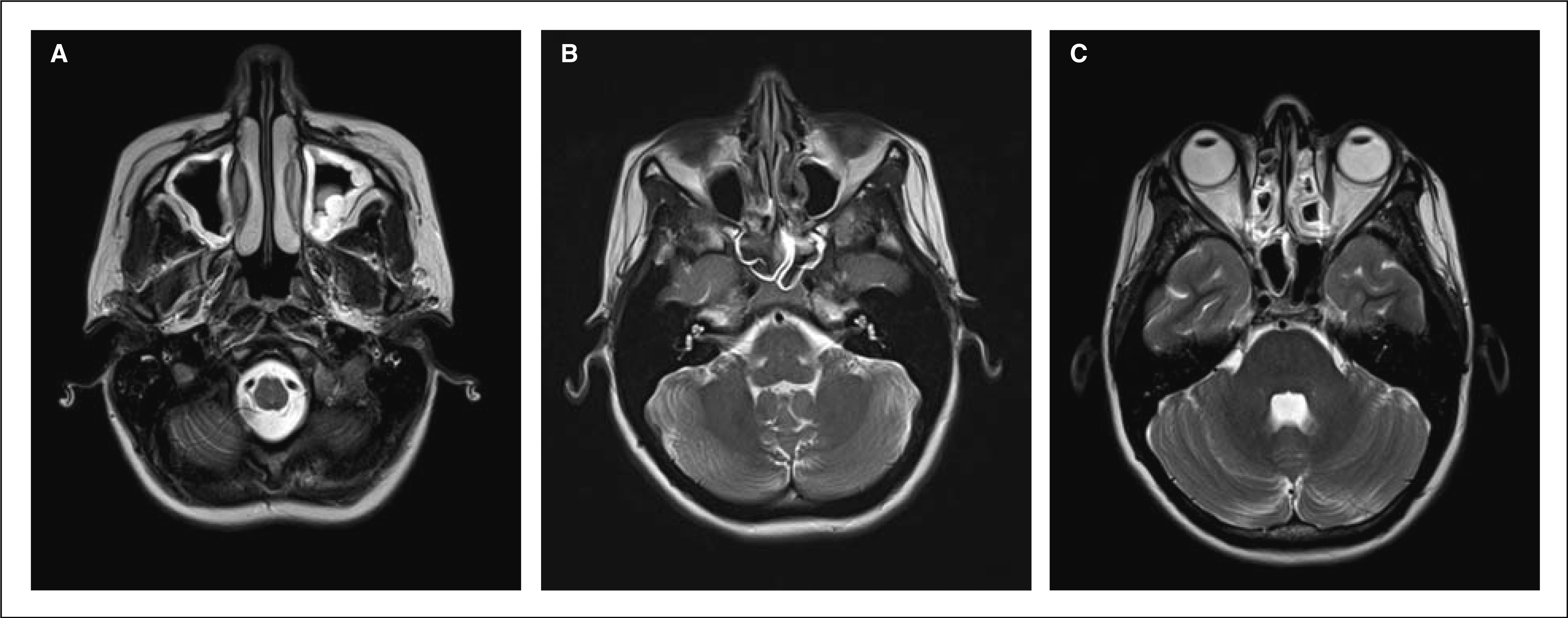
Discussion
Here, we report a case of a young patient with repeated, long-lasting headaches manifested not just during flight landing, but also during travel on the subway, in tunnels, as well as up- and downhill driving. Consistent with previous reports, the pain was localized to the anterior part of the head; aura, autonomic and vegetative symptoms were not present (1–6). The sudden-onset headache was not constant: the high-intensity pain subsided after a few minutes (1–6). However, the pain lasted much longer than previously reported, and the headache was bilateral, in contrast to most published cases characterized by unilateral pain (1–6). Based on our imaging studies, we suspect that the long pain duration and the bilateral pain projections could be attributed to the bilateral sinus pathology.
Paranasal sinuses have various physiological functions, including regulation of intranasal pressure. Under particular travel circumstances the ambient pressure increases (e.g. during airplane descent) or decreases (e.g. during airplane ascent) (7, 8). Under abnormal conditions, a vacuum effect due to the relatively low or high pressure inside the sinuses may result in mucosal oedema, seroangineous exudates, and even submucosal haematoma (7). Sensory impulses from the affected sinus mucosa are conducted by branches of the trigeminal nerve, leading to referred pain in the anterior part of the head (8). Furthermore, barotraumas could stimulate nociceptors of local arteries, which may contribute to the headache via the trigeminovascular system (2). It is likely that impaired sinus ventilation due to rhinosinusitis creates disposition not only to barotrauma but also to prolonged recovery. Since air outflow from sinuses is altered in rhinosinusitis, the pain can be triggered by minor changes in ambient pressure, e.g. during travelling down or uphill, on subway and in tunnels. Such small but frequent alterations in pressure may prevent alleviation of the symptoms. Furthermore, successful symptomatic therapy with antihistamine and nasal decongestant supports the theory that sinonasal barotrauma plays a triggering role in the pathophysiology of airplane headache.