
Abstract
This study explores the relationship of the pain of the migraine headache and the associated features of migraine. Migraineurs (n = 1025) (ICHD-2, 1.1-1.2 and 1.5.1) were evaluated retrospectively using a detailed database (daily unremitting excluded). Variables studied included headache intensity and duration, associated symptoms and pain characteristics. Non-parametric correlations were used to evaluate relationships among variables. Headache intensity correlated with nausea, vomiting, photophobia, phonophobia, dizziness (all P = 0.000), running of the nose/tearing of the eyes (P = 0.007), and osmophobia (P = 0.044), but not with diarrhoea or taste abnormality. Headache duration correlated only with osmophobia (P = 0.002) and taste abnormality (P = 0.005). Throbbing, pressure and stabbing pain correlated with most of the associated symptoms. Aching correlated only with taste abnormality. This correlational study demonstrates that migraine pain is clearly related to nausea, but is also correlated with other associated migraine symptoms. Taste abnormality and osmophobia are better correlated with headache duration rather than headache intensity.
Introduction
Visceral pain is often accompanied by nausea and/or vomiting (1–3). Most migraine attacks include nausea and other associated symptoms. The onset of pain usually precedes the associated symptoms. It seems intuitive that the more intense the migraine attack (usually judged by the degree and/or duration of pain), the worse the associated symptoms. However, the relationship between both the intensity and the duration of pain and the associated symptoms of the acute migraine attack has never been established. Nor is it known whether all the associated symptoms behave in the same fashion in relation to the pain. Furthermore, pain of the acute attack is often described by migraineurs as throbbing, but other descriptions such as aching, pressure and stabbing are used. It is not known whether any or all of these characteristics of the migraine pain predict the occurrence of any, all, or some of the associated symptoms during the migraine attack.
This study explores the relationship between the intensity, duration and character of the pain of the acute migraine attack and the nausea and other associated migraine symptoms experienced during the migraine attack, using a large detailed clinical database in tertiary headache care.
Patients and methods
Study population
The study population consisted of consecutive patients treated by one of the authors (L.K.) in his clinical practice with the clinical and computer-aided diagnosis of migraine, ICHD-2, 1.1, 1.2, and 1.5.1 (4), with daily unremitting headache patients being excluded. A computer program was used to record the data at the time of the initial structured interview conducted either by L.K., or by nurse practitioners trained in headache and neurology.
Patients were excluded from the study if they had: (i) no headache; (ii) headaches thought to be related to trauma or injuries; (iii) complicated neurological problems, i.e. underlying brain or systemic illness related to their headaches; (iv) recent onset headaches, i.e. <1 month prior to study; (v) significant legal issues related to their headaches; (vi) been seen prior to the initiation of the database; (vii) declined to, or were cognitively not able to participate in the database interview; and (viii) language or intellectual barriers.
Study design
All patients received a headache evaluation, based on their past month's typical headache characteristics, as well as a physical and neurological examination. A thorough medical history of these patients was also recorded. All current and past acute migraine medications, prescribed or non-prescribed, used by the patients were noted. All patients were evaluated by L.K. The headache diagnoses were made according to International Headache Society criteria (3) using a computer algorithm written by L.K., and each patient's diagnosis was clinically verified by L.K. Approval was obtained from an institutional review board for the use of the patient's information. The personal identities of patients were discarded when the data were downloaded to the statistical package.
Headache intensity, headache duration, headache character, nausea and other associated symptom rating
All assessments were based on the ‘average’ headache. Headache intensity was rated by the patient on a 0–10 scale, with 10 being unbearable pain. Headache duration was recorded in minutes. Associated migraine symptoms occurring during the migraine attack (nausea, vomiting, photophobia, phonophobia, dizziness, diarrhoea, running of the nose/tearing of the eyes, osmophobia and taste abnormality) and headache pain characteristics (throbbing, aching, pressure and stabbing) were graded on a 0–3 scale ranging from none through mild, moderate, and severe. The associated symptoms recorded were found to be the commonest reported by patients and hence routinely assessed in all patients seen in the clinic. These symptoms were not diary controlled, although many of the patients had recorded these parameters using the Headache Center of Atlanta website and also using diaries from previous headache care providers.
Statistical analysis
Descriptive statistics were obtained using SPSS version 11 for the Macintosh (SPSS Inc., Chicago, IL, USA). Correlations were performed using Spearman's ρ. One-way
Results
Demographic characteristics
One thousand and twenty-five migraineurs (ICHD-2, 1.1–1.2 and 1.5.1) were evaluated, patients with daily unremitting headache being excluded. Of the migraineurs, 85.6% were females, the mean age was 38.2 (SD 12.2) years, mean body mass index was 25.2, 60.7% were married, 33.7% single, 5.1% divorced, and 0.5% widowed, mean lifetime duration of headache was 14.9 years, average duration was 29.2 h (mean) and 24.0 h (median), average intensity was 7.4 (mean) and 7.0 (median), and mean migraine headache frequency 12.7 headache days per month. Reported percentage frequency of associated symptoms: nausea 90.1%, vomiting 51.8%, photophobia 93.9%, phonophobia 91.4%, dizziness 72.4%, diarrhoea 28.2%, running of the nose/tearing of the eyes 44.2%, osmophobia 28.0% and taste abnormality 23.1%. Reported frequency of headache character: throbbing 91.6%, aching 87.9%, pressure 89.6% and stabbing 71.0%.
Study results
Headache intensity correlated with nausea, vomiting, photophobia, phonophobia, dizziness (all P = 0.000), running of the nose/tearing of the eyes (P = 0.007), and osmophobia (P = 0.044), but not with diarrhoea (P = 0.054) or taste abnormality (P = 0.550). Figure 1 shows the headache intensity expressed as moderate (4–6/10), severe (7–8/10), and very severe (9–10/10) vs. the grade of associated symptoms(0–3) with the χ2 significant values shown.

Headache intensity expressed as moderate (4–6/10), severe (7–8/10), and very severe (9–10/10) vs. the grade of associated symptoms (0–3). χ2 significant values are shown.
Unlike intensity, headache duration in minutes correlated only with osmophobia (P = 0.002) and taste abnormality (P = 0.005).
Three headache characteristics—throbbing, pressure and stabbing—show similar significant correlations with associated symptoms; aching headache does not (see Table 1). Of note, while there was a strong correlation between headache intensity and throbbing (P = 0.000), pressure (P = 0.002) and stabbing (P = 0.000), this is not seen with aching (P = 0.109).
Correlation of headache character and migraine-associated symptoms

Values in bold are statistically significant (P < 0.05).
Table 2 shows the impact of increasing migraine-associated features on headache pain intensity. Diarrhoea does not show the progressive increasing trend shown by the other symptoms. Figure 2 shows the grade of associated symptoms (0–3) vs. the pain intensity expressed as moderate (4–6/10), severe (7–8/10), and very severe (9–10/10) with the χ2 significant values shown.
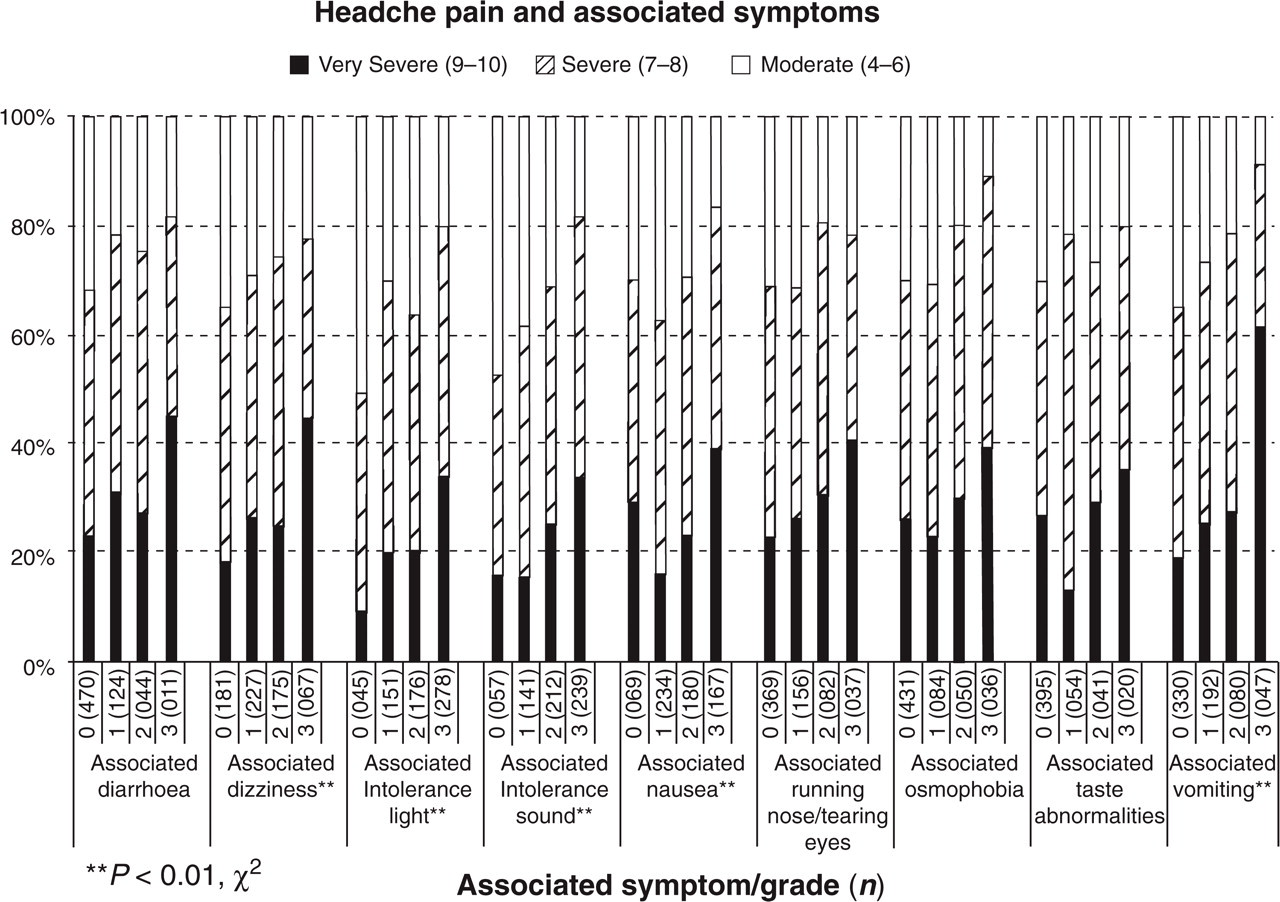
Grade of migraine-associated symptoms (0–3) vs. headache pain intensity expressed as moderate (4–6/10), severe (7–8/10), and very severe (9–10/10). χ2 significant values are shown.
Headache pain intensity for increasing grade of migraine-associated symptoms. Mean ± SD (n)

One-way analysis of variance (
Discussion
Visceral pain is well documented to produce nausea (1–3). Visceral afferents are presumed to project to emetic components of the solitary tract (5). Somatic pain is often accompanied by nausea and presumably similar projections to the solitary tract are present. Nausea is one of the defining features in the classification of migraine (4). The clinical impression is that the more severe the migraine attack, the greater the nausea and other associated symptoms. The relationship of pain to nausea and other associated symptoms has not been systematically evaluated in migraine attacks. However, recently this relationship has been experimentally evaluated in migraine patients and controls (6). Production of pain by application of ice to the temple produced nausea on the third application but did not when applied to the hand in migraineurs or to the temple in non-migraineurs. This implies some uniqueness in the migraineur's activated trigeminal system in producing nausea. Photophobia has also been shown experimentally to be induced in migraineurs, but not in controls, by painful stimulation in the trigeminal nerve distribution (7). Verification of these findings is difficult in the acute migraine attack. However, one way to approach this issue is to assess the effect of increasing pain intensity recorded by migraineurs on the degree of nausea and other associated symptoms experienced during a migraine attack. The current study was done to explore the relationship of migraine pain intensity, duration, and character to nausea as well as to other associated migraine symptoms.
The study shows a very convincing correlation of the intensity of the migraine pain to the degree of nausea. These findings do not necessarily imply cause and effect, however. Selective blocking of pain without impacting on the other components of the migraine attack may be the only way to verify that the pain is causing the increased nausea. Triptans, not known to decrease nausea in other conditions, may reduce nausea in the acute migraine attack but the mechanism is unknown and may not be related to the reduction of pain. Rarely patients will report nausea without headache in migraine, while nausea can be a premonitory symptom (8) and these are clinical points against this hypothesis. Headache intensity also correlated strongly with vomiting, photophobia, phonophobia, dizziness, running of the nose/tearing of the eyes and osmophobia (barely, P = 0.044) but not with diarrhoea or taste abnormality. This suggests that nausea is not unique and most of the other associated symptoms are similarly affected by increasing the intensity of pain of the acute migraine attack.
Reference to Table 2 and Fig. 2 shows that increasing nausea and also other associated symptoms are correlated with increasing migraine pain intensity. Thus, increasing either pain or nausea and associated symptoms may increase the other and produce a multiplier effect, resulting in a more intense and prolonged migraine attack as suggested by Drummond (7).
A recent study of cluster headache supports the hypothesis of pain intensity, in at least some primary headaches, being correlated with associated symptoms (9). Comparing 148 typical cluster headache patients with nine patients without cluster-associated autonomic symptoms, it was concluded that the less intense the acute attack, the less likely the presence of associated autonomic symptoms.
Unlike migraine pain intensity, in the current study headache migraine pain duration correlated only with osmophobia and taste abnormality and not with other migraine headache-associated symptoms. Thus, intensity and not duration of headache may be the activator of most, but not all associated symptoms.
Taste abnormality and osmophobia may behave in a different fashion, as documented in both the headache intensity and the headache duration data. Taste abnormality and osmophobia are better correlated with headache duration rather than headache intensity and these associated symptoms may be driven by other factors.
Patients frequently describe the quality of their headaches in terms of throbbing, aching, pressure or stabbing. Table 1 shows that throbbing, pressure and stabbing correlate strongly with most or all of the associated symptoms. Aching shows little correlation with associated symptoms, with the exception of taste abnormality. There is a strong correlation between headache intensity and throbbing (P = 0.000), pressure (P = 0.002) and stabbing (P = 0.000), but not aching (P = 0.109). Thus aching is the only headache character which does not correlate with headache intensity and may explain why aching is different from the other headache characteristics. This finding also supports the relationship between headache intensity and associated symptoms.
Figure 3 shows possible mechanisms/pathways of migraine pain producing nausea and other associated symptoms. One of the more likely pathways to nausea is the activation of nausea-responsive neurons in the solitary nucleus and tract by input from the trigeminal nucleus caudalis. This connection has been documented (10, 11). However, other unknown pathways or mechanisms may be involved and some of the pathways may be reciprocal. The pathways and mechanisms involved in the other associated symptoms of migraine are not known.

Potential relationships between pain, nausea and other associated features.
The modular theory of headache suggests that different modules of neurons may be activated and produce clinical expression of the acute migraine attack (12). Therefore, the character of the migraine may be dependent on the particular module(s) of migraine being activated. For example, the activated pain pathways may activate associated symptoms pathways; or the pain pathways and the nausea pathways may both be simultaneously activated by another mechanism and may not be related to either symptom having an effect on the other. Also, one module may feed back positively on another module as suggested by the nausea and other associated symptoms impacting on pain, alluded to before.
This study suffers from some limitations. This is a study of a single tertiary care clinic and is also not a population cross-sectional study. An important limitation of the study is the absence of diary documentation or preferable real-time electronic documentation (13) of all migraine events. However, some patients had documented headache profiles from prior provider evaluations and use of the clinic's website questionnaire prior to first visit. Also lacking in this study is the temporal evolution of the headache in both individual headaches (14) and over years for individual patients. The large number of correlations performed in this study almost guarantees that some will be statistically significant by chance. The most important shortcoming is that this study documents associations which do not prove cause and effect.
Conclusion
Using clinical data, this study supports the hypothesis that migraine pain intensity is correlated with nausea and most other associated symptoms. While intuitive, this has not been demonstrated before. Surprisingly, differences were found between the associated symptoms. Taste abnormality and osmophobia are better correlated with headache duration rather than headache intensity. Throbbing, pressure and stabbing pain qualities, which also correlate with pain intensity, correlate with the associated symptoms. Aching, which does not correlate with pain intensity, does not correlate with associated symptoms. The study does not establish a cause and effect relationship between the various correlations. The mechanisms and pathways of these findings remain to be elucidated.