
Abstract
The aim of this study was to determine the efficacy of deep brain stimulation (DBS) in the treatment of various types of intractable head and facial pains. Seven patients underwent the insertion of DBS electrodes into the periventricular/periaqueductal grey region and/or the ventroposteromedial nucleus of the thalamus. We have shown statistically significant improvement in pain scores (visual analogue and McGill's) as well as health-related quality of life (SF-36v2) following surgery. There is wide variability in patient outcomes but, overall, DBS can be an effective treatment. Our results are compared with the published literature and electrode position for effective analgesia is discussed.
Introduction
Headache can be extremely challenging to treat. In some patients, standard medical treatment proves ineffective and more invasive forms of treatment, in carefully selected patients, we feel can be justified. Surgery is now accepted treatment in trigeminal neuralgia but its place in the treatment of other headache and facial pain syndromes is not firmly established.
Deep brain stimulation (DBS) has been used successfully in the treatment of chronic neuropathic pain for a number of years (1, 2). More recently, it has been used for the treatment of cluster headache (3, 4). This is a prospective study of seven patients with a variety of cephalalgia in whom we have used DBS. Pre-operative and postoperative pain was measured with visual analogue scores (VAS) of pain and the McGill's Pain Questionnaire (MPQ). Health-related quality of life was measured with the Short-form 36 version 2 (SF-36v2) questionnaire. All patients underwent a comprehensive neuropsychological assessment. All patients underwent insertion of deep brain stimulating electrodes in the periventricular grey/periaqueductal grey area (PVG/PAG) and/or the ventroposteromedial nucleus of the thalamus (VPM), as these were the areas where we have previously found the best analgesia (5–7).
Methods
Seven patients with a variety of different types of head and facial pain syndromes were referred for consideration of DBS. Most often the referral was from a pain clinic, but referrals were also received from neurologists and one from a neurosurgeon. All headaches were classified according to the International Classification of Headache Disorders (8). The mean age was 44.4 years (median 41). There were four male and three female patients. Aetiology varied but included only neuropathic pain affecting the face or head (see case histories below). Medication was recorded pre- and postoperatively but, for simplification, the number of classes of analgesic that a patient was regularly taking is presented. After appropriate informed consent and permission from the local ethics committee, all patients underwent placement of a deep brain stimulating electrode into the PVG/PAG and, in addition, four patients also had a second electrode placed in the VPM nucleus of the thalamus. This second electrode was not inserted if either there appeared to be adequate intraoperative pain relief with the PVG/PAG electrode or the patient became fatigued and stimulation of the PVG/PAG electrode produced sensations in the area of pain (three patients). During postoperative testing, both electrodes were stimulated (both separately and synchronously) to achieve optimal pain relief. These details are summarized in Table 1.
Patient demographics and aetiology

F, female; M, male; PVG, periventricular grey; VPM, ventroposteromedial nucleus of the thalamus; ICHD, International Classification of Headache Disorders. No. of analgesics refers to the number of classes of analgesics that a patient was taking regularly.
Case histories
All patients suffered from severe, intractable neuropathic pain affecting the face or head and had been treated in a pain clinic with a variety of medications without success.
Case 1—anaesthesia dolorosa
A 64-year-old female with severe anaesthesia dolorosa affecting the V2 and V3 distribution on the right. She initially presented almost 10 years previously to another neurosurgical centre with trigeminal neuralgia. After failure with standard pharmacotherapy, she underwent three glycerol injections to the Gasserian ganglion and after failure of these, a microvascular decompression. Subsequently, she developed anaesthesia dolorosa which was unsuccessfully treated with a Vth tractotomy. She was being treated with antidepressants as well as regular morphine and codeine.
Case 2—terminal branch neuralgia secondary to surgery
A 41-year-old male who had multiple operations on his maxillary sinuses for the treatment of recurrent infectious sinusitis 15 years previously. Despite successful treatment, he developed severe, constant, stabbing pain affecting the periorbital area on the left and extending to his vertex. After 13 years of unsuccessful pharmacotherapy, he opted for DBS.
Case 3—terminal branch neuralgia secondary to surgery
A 59-year-old male who developed severe, bilateral perioral burning dysaesthesia 1 year after a resection of a left tonsillar carcinoma with radical neck dissection. It mainly affected the lower lips and to some extent the inside of his oral cavity.
Case 4—post-herpetic trigeminal neuralgia
A 33-year-old female with a 10-year history of severe post-herpetic trigeminal neuralgia affecting the right V2 and V3 distribution of her face. She had also failed medical therapy with a variety of drugs including morphine sulphate, carbamazepine, amitriptyline and gabapentin
Case 5—chronic postcraniotomy headache
A 46-year-old male who developed severe burning and stabbing pain affecting the right forehead and associated with headache, 6 months after a routine craniotomy for resection of a frontal meningioma.
Case 6—chronic post-traumatic headache
A 34-year-old who suffered a major traumatic head injury following a fall 4 years previously. He was left with mild memory and cognitive problems as well as severe daily headaches centred on the vertex and radiating to both sides.
Case 7—occipital neuralgia attributable to surgical neck trauma
A 34-year-old female who had resection of a cervical (C1/2) schwannoma on the right at the age of 7 years. A recurrence necessitated a second resection in her early twenties. Three to four years later, she developed severe right-sided occipital neuralgia that was not amenable to medication or rhizolysis of the occipital nerve.
Surgical technique
The technology used for targeting the PVG/PAG and VPM is derived from that used for the treatment of Parkinson's disease. Our detailed surgical technique has been described previously (9). Our image-guided technique of targeting PVG/PAG and VPM is as follows. Because the Cosman-Roberts-Wells (CRW) stereotactic frame is not magnetic resonance imaging (MRI) compatible, the targeting was carried out on fused stereotactic magnetic resonance/computed tomographic (CT) scans of 2 mm in thickness using the Radionics Image Fusion and Stereoplan programs. This also reduces errors secondary to field inhomogeneities in magnetic resonance scanning. The third ventricle, the opening of the cerebral aqueduct and the posterior commissure were identified along the midline on the axial images at the levels below and above the AC-PC line. For the VPM, the target site was at the level of the AC-PC line, 12 mm lateral to the midline and 6–8 mm posterior to the mid-commissural point (MCP). For the PVG electrode, the intended target for placing the deepest electrode contact was marked at the periaqueductal grey at a level of <10 mm below the AC-PC line; between the dorsal part of the red nucleus and the superior colliculus in the AP plane; and approximately 5 mm lateral to the lateral boundary of the aqueduct and the third ventricle. Next, the electrode trajectory was selected to avoid possible penetration of the surface vessels on the cortex and the lateral ventricle. This leads to some adjustment of the PVG target localization for each individual patient, and probably contributes to interpatient variation in electrode placement. After making a 2.7-mm twist-drill hole in the skull, a Radionics electrode of 1.8 mm diameter and 2.0 mm exposed tip was slowly passed towards the target while the impedance values were monitored for a sudden drop in impedance value from 500 to 600 Ω to under a few tens of ohms, suggesting possible penetration of a ventricle. The Radionics electrode was replaced by a Medtronic 3387 electrode (Medtronic Inc., Minneapolis, MI, USA). Test stimuli were applied at <3.0 V in amplitude, 120 μs in pulse width and 10–50 Hz in frequency to check for a warm feeling or paraesthesiae in the area of pain or pain suppression, and abnormal eye movements (PVG). Once the pain suppression area was identified functionally, the DBS electrode was fixed onto the skull and externalized for further investigation. The whole stimulation system was then internalized a few days later in a second procedure.
Recording of pain scores
Preoperatively, and at 1 year, each patient recorded twice daily (a.m. and p.m.) VAS of pain (scale of 1–100) in a pain diary over a 12-day period. The 24 VAS scores were averaged to give a single preoperative and postoperative figure. Pre- and postoperative VAS for each group were compared using a paired t-test with a two-tailed P-value of <0.05 taken as significant. Each patient also completed an MPQ on both occasions, in the presence of a specialist nurse. For analysis of data, we used the Ranked Pain Rating Index (PRI(R)) as described by Melzack (10). In this method of scoring, each word in a category is assigned a number, depending on its severity. Using this method, we calculated overall pain rating index PRI(R) (out of 78), sensory PRI(R) (out of 42), affective PRI(R) (out of 14), evaluative PRI(R) (out of 5) and miscellaneous PRI(R) (out of 17). In addition, as we were particularly interested in the burning component of pain, we scored question 7 separately. Question 7 gives the patient the opportunity to select one of four words of increasing severity (hot, burning, scalding, and searing) and they were thus assigned a score of 0–4. Pre- and postoperative MPQ scores for each group were compared using the t-test with a P-value of <0.05 taken as significant.
Health-related quality of life
This was assessed pre- and postoperatively using the SF-36v2 questionnaire. We used the summated ratings and standardized SF-36 scoring algorithms documented elsewhere to score the eight SF-36 scales (11, 12). The eight categories are as follows: Physical functioning (PF) gives a subjective assessment of the patient's physical well-being; Role physical (RP) describes how the patient's usual activities are affected by physical problems; Bodily pain (BP), General health (GH), Feeling of vitality (VT), General mental health (MH) are as perceived by the patient; Social functioning (SF) is how the patient's social activities are affected; Role emotional (RE) describes how the patient's usual activities are affected by emotional problems. Pre- and postoperative scores for each category, including physical component scores (PCS) and mental component scores (MCS), were compared using a t-test (P < 0.05 taken as significant).
Post-operative electrode localization
We calculated the exact position of the PVG electrodes in four patients using the postoperative MRI (the other three had only postoperative CT, not MRI). The aim was to look at the variability in the position of these electrodes, although the number of patients was too small to comment on position and degree of pain relief. The calculations were carried out as follows. First, the MCP was calculated. Then, the position of the lowest electrode contact (out of four) was calculated relative to the MCP (in the anteroposterior plane), relative to the midline (giving a lateral value) and relative to the AC-PC line (giving a vertical value). The lowest contact was used as this corresponds to the ‘target’ that is calculated during surgery.
Results
In general, five patients were very pleased with the results of stimulation. Two patients (1 and 3) were less positive but did not regret having the procedure carried out. As shown in Table 1, all but one patient were able to reduce the number of analgesic medications, and three patients were able to stop medication altogether. Only one patient (patient 1) required opioid analgesics postoperatively (compared with six preoperatively). It should be noted that follow-up for titration of the stimulation parameters is an ongoing process (see Discussion).
Electrode locations
Figure 1 shows typical electrode placements in both PVG and VPM nuclei. The mean relative distances to the MCP (four patients) were −15.9 mm (i.e. posterior) in the AP plane (SD = 3.2), 4 mm in the lateral plane (SD = 1.7), and −6.8 mm below the ACPC line (SD = 1.5).

Postoperative T1-weighted axial magnetic resonance imaging scans showing electrode placements. On the left, the lowest contact of the VPM electrode (white arrow) is shown laterally to the PVG electrode that is traversing the region just lateral to the posterior commissure. On the right, the final position of the PVG electrode (black arrow), just anterior to the superior colliculus.
Visual analogue scores
The mean reduction in VAS was 53.4% (SD = 22.9) (Table 2). However, improvement varied from as little as 17.6% at 2.5 years in a patient with idiopathic trigeminal neuralgia to 100% at 2.5 years in a patient with post-herpetic trigeminal neuralgia. Statistical analysis using a paired t-test showed that these results were significantly different (P = 0.003). The two patients with the worst postoperative improvement (patients 1 and 2) both had initially good results. However, their more recent pain scores may have been adversely influenced by additional pain. Patient 1 developed a severely painful frozen shoulder that, we believe, may have influenced her reporting of pain. Similarly, patient 2 developed pain associated with the extension lead tract (presumably due to fibrous scarring). This pain was not influenced by the stimulator as it was in a different somesthetic area.
Pre- and postoperative pain scores for each patient.
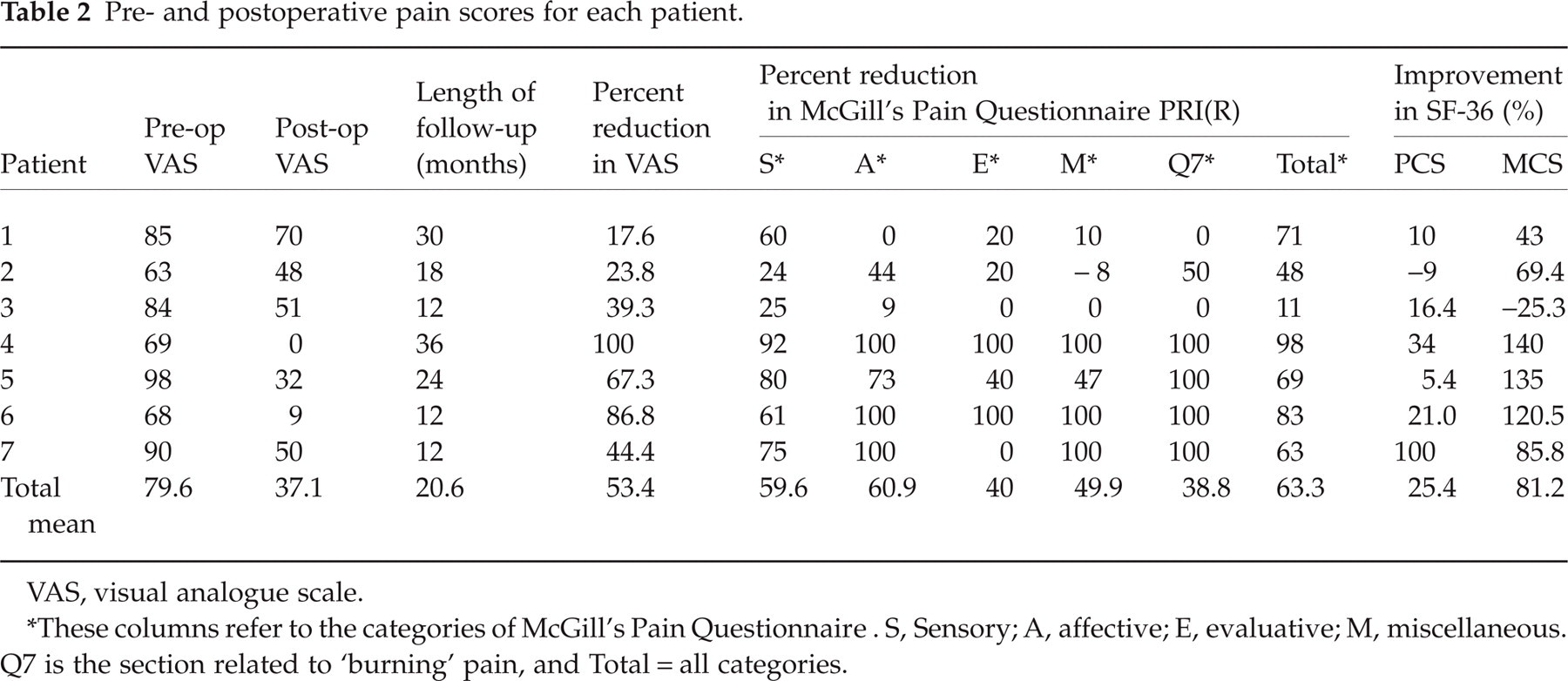
VAS, visual analogue scale.
These columns refer to the categories of McGill's Pain Questionnaire. S, Sensory; A, affective; E, evaluative; M, miscellaneous. Q7 is the section related to ‘burning’ pain, and Total = all categories.
McGill's Pain Questionnaire
There was a significant reduction in ‘total’ ranked pain rating index (PRI(R) total) after surgery by 63.3% from a mean preoperative score of 54.1 to 19.4 postoperatively (P = 0.018, t-test). Table 2 and Fig. 2 summarize these results. Similarly, there was a significant reduction in all PRI(R) subgroups (P < 0.05, t-test), with the sensory and affective groups improving by approximately 60%. The only exception was the ‘miscellaneous’ subgroup that was weakly significant (P = 0.058).

Pre- (▪) and postoperative (□) McGill's Pain Questionnaire (MPQ) scores for each category. The method used is the Pain Rating Index (R) (PRI(R)) as defined by Melzack (see Methods). Misc, Miscellaneous. Error bars denote 1 SD from the mean. All categories reached statistical significance (see Results).
Table 2 shows that there are clearly two groups of patients. The first (patients 2 and 3) made small improvements but not dramatic ones. Although there has been some improvement in sensory scores, there is certainly little or no improvement in the ‘evaluative’ scores that describe how the pain affects the patient's activities. The other group showed impressive improvements in both VAS and MPQ scores with 100% improvement in many of the affective/evaluative categories. In these patients, burning pain (Q7) seemed to improve markedly.
Health-related quality of life
The pre- and postoperative SF-36 scores are summarized in Table 2 and Figs 3 and 4. Overall, there was a significant improvement in MCS from 22.2 (SD 5.2) preoperatively to 43.2 (SD 17) postoperatively (P < 0.05). However, although PCS improved from 29.5 to 39.1, this was not significant. Figure 4 shows that none of the individual physical categories improved, but that improvements were mainly due to better scores in the bodily pain, general health and social functioning categories.

Changes in the physical component score (PCS) and the mental component score (MCS) as a result of surgery. ∗P < 0.05 (see text for details). ▪, Preoperative; □, postoperative.

Overall breakdown of preoperative (▪) and postoperative (□) SF-36 scores for each category. PF, Physical functioning; RP, Role physical; BP, Bodily pain; GH, General health; VT, Vitality; SF, Social functioning; RE, Role emotional; MH, Mental health. ∗P < 0.05 (t-test).
Complications
There were no deaths in this series. One patient (patient 5) had a chronic implant infection that was treated with long-term oral antibiotics until, after 2 years, recrudescence of the infection led us to remove the implant. It has now been successfully reimplanted. A second patient (patient 2) has pain associated with the extension lead and is awaiting revision.
Discussion
This study has shown that deep brain stimulation of the PVG/PAG and/or VPM nucleus of the thalamus can significantly improve a variety of different types of cephalalgias, including trigeminal neuralgias, postoperative facial pain, occipital neuralgia and post-traumatic headache. This has been demonstrated by improvements in both pain scores and the SF-36v2 health-related quality of life questionnaire. However, it is clear from our results that some patients fare significantly better than others. Looking at the overall pain scores (VAS and MPQ), there are four patients (4–7) who have done well on both sets of scores, and three who have not done so well on VAS and/or MPQ. Subjectively, this correlates with whether these patients feel that they have done well or not. It also correlates with improvement in SF-36 scores, i.e. the three patients that improved the least in the pain scores also improved least on the SF-36. The question is whether this could, in retrospect, have been predicted. The main difference between the two groups is that the former group, who did less well, were those who had been subjected to multiple episodes of surgery, often in order to try to treat their pain. For example, patient 1 had had a multitude of procedures for her trigeminal pain, including rhizolysis, microvascular decompression and Vth nucleus tractotomy. She eventually developed a different pain (in her shoulder) that masked her original pain. Patient 3 had had multiple operations on his neck and the origin of the pain was somewhat obscure. In addition, when other factors may be contributing to the pain (e.g. patient 2 developed pain related to the extension lead), treatment tended to be less successful. All of the patients required intensive programming sessions(lasting up to an hour) when initially treated. These sessions were repeated at 3–6-monthly intervals for the first year and then on an annual basis, unless the patient experienced a return of their pain. Pain will often respond to a narrow frequency range of stimulation (e.g. 30–50 Hz). It may be, therefore, that patients with more than one nerve involved, or additional pain from another source, are more difficult to treat than those with a single specific source of pain.
The SF-36 health survey has been extensively validated, both with respect to changes in scores with treatments as well as population norms (13–17). It has also been used extensively in the evaluation of patients with chronic neuropathic pain (18–21). Comparison of our data with local population norms (22) for SF-36v2 shows that, even postoperatively, these patients have much lower scores than expected in an age-matched population. Our results show that the MCS improve markedly, compared with the PCS scores. This is not surprising, considering that DBS does not treat any underlying physical condition, but attempts to alleviate the pain that has resulted from it.
DBS has been successfully used to treat a variety of neuropathic pain syndromes (2, 5, 23–25). The largest of these series (23) included 12 patients with anaesthesia dolorosa who did not successfully respond to DBS. DBS is also under investigation in the treatment of chronic cluster headaches (3, 4, 26, 27). Our series differs from these studies in terms of both aetiology and effectiveness of stimulation, which varied widely, depending on the aetiology.
Various targets for DBS electrodes have been described, including the VPL-VPM (1), center median-parafascicular complex (CM-Pf) (25) and the periventricular grey area. Our average co-ordinates for the PVG are several millimetres posterior to those described by May et al. (28) (x =−2, y =−18, z =−8 in Tailarach space) as the area that has been shown, with the use of positron emission tomography, to be activated in cluster headache. These authors describe this area as the posterior hypothalamus and we believe we are targeting a different region. Also of note is that our PVG electrodes are placed on the side contralateral to the pain, in contrast to cluster headache, where the electrodes are placed ipsilaterally.
In summary, we have shown that DBS, in carefully selected patients, is a safe and effective treatment in a variety of headaches and facial pains and that it can lead to improvement in health-related quality of life. However, there is wide variation in pain improvement after treatment with DBS and we need to elucidate further the factors that will allow us to predict which patients will do best.