
Abstract
One aim of the Vågå study of headache epidemiology was to depict the total panorama of headaches in a small-sized, Norwegian community at the end of the 20th century. In the present part of the study, a search was made for the rare, global headaches. Various, relatively unknown headache categories were observed, such as hydrogen sulphide intoxication (n = 2) after exposure to H2S ambient air concentrations of ≥100 p.p.m. In Vågå, nitroglycerine headache (‘dynamite headache’) proved to be a relatively frequent disorder (n = 13). This represents approximately 0.7% of the study group. A main reason for this, in all probability unusually high frequency is that there previously have been soapstone mines within the precincts of the parish. Another relatively frequently occurring headache followed exposure to wind (n = 7; 0.38%). Ice-cream headache was rare (n = 3; 0.16%), when only the general question was asked: ‘other headaches?’. Approximately 7 years later, an ad hoc procedure was adopted: 50 parishioners who did not answer positively concerning ice-cream headache on the first examination were asked specific questions concerning ice-cream headache. Four had had such an experience, i.e. prevalence of 8%, which is 50 times higher than the original result, but still a rather low prevalence when compared with the mean prevalence from other studies: 39%. This demonstrates that the result as regards prevalence, even for a headache such as ice-cream headache, to a large degree depends upon the interview technique used.
Keywords
Introduction
Several separate headache disorders actually seem to be of the Lilliputian type, as regards prevalence. Generally, any group with a low prevalence, e.g. <0.1%, will be hard to detect in a general headache epidemiology study unless there are clear, easily recognizable traits, such as in cluster headache, chronic paroxysmal hemicrania (CPH) or neck–tongue syndrome. The methodology chosen will to some extent determine the outcome of any study trying to outline the whole panorama of headaches, including the rare ones. The picture may be most complex; there may be various headaches interwoven with each other during a lifetime, such as sinus headache, refraction anomaly headache, etc.; in addition, in strenuous periods, tension-type headache. Also, as demonstrated herein, there may be extremely rare and unexpected headaches, such as hydrogen sulphide headache. If there are several, concomitant headaches, which is frequently the case, and if a questionnaire approach is chosen to sort out the separate headaches, including the rare ones, the likelihood of a fake reflection of reality would seem to be overwhelming.
The Vågå study of headache epidemiology (n = 1838) mainly addresses the major headaches. Another aim of the study was to depict the entire panorama of headaches at the grass-roots level at the end of the 20th century and in this part of the world. A local flavour might enter into the picture: various headaches, such as the ‘Chinese restaurant syndrome’, or monosodium glutamate-induced headache (1, 2), can hardly be expected to be endemic in the heartland of Norway. However, due to special circumstances with the mining industry, nitroglycerine headache might be expected to be more prevalent in Vågå than other rare headaches.
The purpose of the present communication is to give a summary survey of rare, global headaches in Vågå.
Materials and methods
There were 3907 inhabitants in Vågå just prior to the initiation of this study in 1995. All parishioners in the 18–65-year-old age group were invited to participate. Of the accessible parishioners in this age-group, i.e. 2075, 1838 (88.6%) were examined by the principal investigator (O.S.), who guided the parishioner through the question round. The single parishioner was not even allowed to see the questionnaire (3). Not infrequently, unexpected side tracks were entered during the examination. The interview can therefore probably best be characterized as ‘semistructured’. A thorough physical/neurological examination of the face, head and neck was included, and so was a short version, general neurological examination. If medically indicated, a more extensive neurological investigation would be carried out.
The first edition of the International Headache Society (IHS) criteria have been adhered to, whenever they covered a particular field: this first version was the one available at the time of the study (4). Headaches were graded on a 0–6+ intensity scale: 6+=‘excruciatingly intense’; 5+=‘severe’ (same as IHS); 4+=‘moderate’ (same as IHS); 3+=‘mild’ (same as IHS); 2+=‘heaviness/discomfort’; 1+=‘minimal unpleasantness’ (for more information, see (5)). Grade 2+ is the first step with socially significant head pain. The details of the make-up and the normal values for ‘features indicative of cervical abnormality’ or ‘cervical features’, ‘CF’, have been published elsewhere (6). In the headache-free portion of the Vågå population (n = 246), the mean ‘CF’ was 0.42+ scale 0–5.0+ and 0.79+ (mean) in the unselected Vågå study group.
Specific questions were asked about two specific headaches: there had been mining industry in Vågå, mainly soapstone industry, up to the middle part of the 1970s. Some parishioners had also been exposed to mine work, tunnel and road construction work outside the parish. Construction and mining workers were accordingly routinely asked about nitroglycerine exposure. Nitroglycerine headache prevalence figures are likely to reflect reality rather closely. ‘Wind headache’ was not part of the original protocol. However, in the very beginning of the study, a couple of parishioners told about their headache after exposure to wind. Subsequently, farmers and others exposed to wind/outdoor life were questioned about the influence of wind in a systematic way. These data may therefore be close to correct.
The high-intensity headache, coming ‘out of the blue’, was a dramatic one, and was reported on spontaneously to us. Otherwise, no specific questions were asked regarding special brands of rare headaches. The positive responses followed the general questions: ‘other types of headache’/‘headache in other situations’? For that reason, the figures obtained are likely to be minimum figures, with some distortions of reality.
The various headache forms encountered are listed in Table 1.
Rare, generalized headaches in Vågå among a study population of 1838 adults

The last two headaches would presumably be rare ones in most areas, and for that reason they are detailed herein. In the present setting, they proved to be relatively prevalent.
Nitroglycerine headache
A total of 13 parishioners had experienced nitroglycerine headache. Only males were affected: mining work was not considered proper work for females. Contact with nitroglycerine, mainly on the hands, led to headache. Some workers in periods had almost daily headache and even several times a day. The first days after vacation seemed to be the worst. However, with steady exposure the exposed individual seemed to become somewhat ‘desensitized’. Headaches became rare and mild when the workers learned how to protect themselves with gloves. Two cluster headache patients by chance had been mining workers. Nitroglycerine headache possibly was less intense than cluster headache. However, one of them had to ‘stand on his knees’ during nitroglycerine headache attacks.
The headache could at times be both severe (46% of cases) and long-lasting (69%: ‘= a couple of hours’) (Table 2). Generally, the headache was global. Nausea was a not infrequent accompaniment, phono-/photophobia infrequent ones, but there was no vomiting (Table 3). The headache was invariably throbbing (2, 7). Some had experienced a considerable number of attacks (Table 3). Exposure, and headache, had generally occurred many years ago.
Nitroglycerine headache—duration and intensity of attack
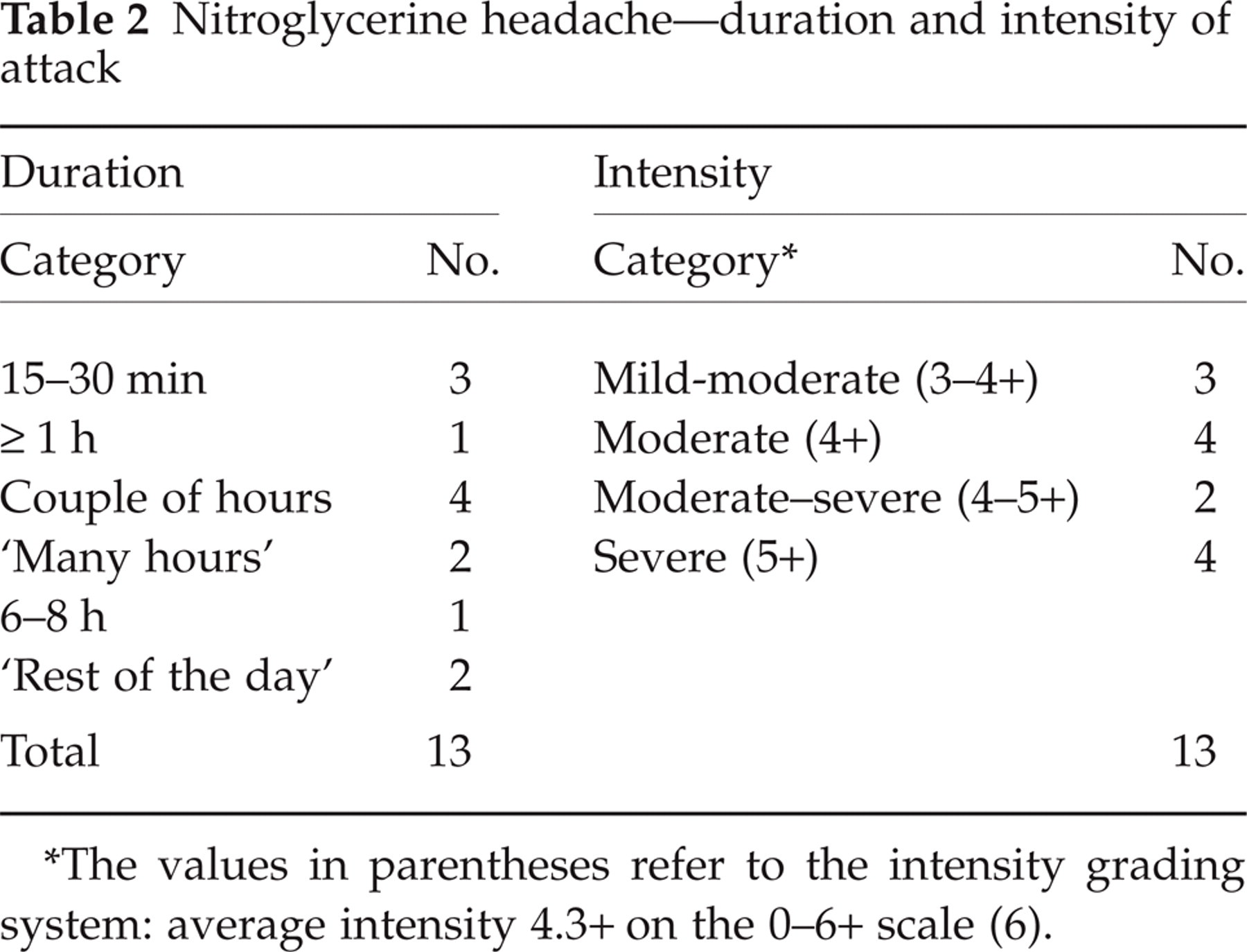
The values in parentheses refer to the intensity grading system: average intensity 4.3+ on the 0–6+ scale (6).
Nitroglycerine headache—Clinical characteristics

Two parishioners had been briefly exposed to nitroglycerine, without developing a headache.
Headache in the wake of nitroglycerine treatment of angina pectoris has not been an item in the present study.
Hypoglycaemia
Two diabetics (onset at ages 6 and 9; male and female, respectively; present ages 26 and 31) had hard-to-monitor diabetes, with a high requirement for insulin. They had experienced multiple episodes of global headache in connection with dysregulation of the diabetes, from 19 years of age and from the beginning, respectively. In the male, the episodes, usually a few per year, lasted <1 h and were characterized by no more than ‘heaviness’/‘mildness’ of pain, i.e. 2–3+ (5); no nausea, no throbbing sensation. Immediate, extra carbohydrate ingestion invariably seemed to abate the situation. In the female, there had been up to 10–15 headache episodes/year, most of them of a moderate degree. A few times a year, however, she lost consciousness and could have convulsions and tongue biting; a longer-lasting and more intense headache would then follow. There appeared to be a temporal relationship between dysregulation of the diabetes, i.e. hypoglycaemia, and the headache.
The headaches were symptom-poor, and none of them had any other headache.
The connection hypoglycaemia/headache is briefly mentioned in some textbooks (e.g. 8–10). However, in many contexts, headache is not even mentioned as a symptom of hypoglycaemia (11). While in the IHS classification from 1988 (4) a glucose value < 2.2 mmol/l is regarded as a criterion, in the new 2004 version (12) it is argued that there is no connection between hypoglycaemia and headache.
The more severe headache episodes in the female may, wholly or partly, have been caused by the convulsions (13).
The present authors have not gone deeper into this matter. The case histories are therefore just summarily presented without taking any position as regards the above argument.
Grass-burning and headache
A 65-year-old male had every year, from boyhood onwards, had a particular headache during the traditional days of ‘grass-burning’, i.e. in late April each year. During a period of 2–3 days or so, left-over, decaying, semidry grass from last year was being burnt. He was convinced that it was only after inhalation of this special type of smoke that this headache appeared and after an exposure of ≥0.5 h. Each episode lasted from a couple of hours to ‘the rest of the day’; a headache starting in the afternoon would have abated by the next morning. The headache was global, but most marked in the anterior parts; it was symptom-poor, not being accompanied by nausea, vomiting, dizziness, photo- and phonophobia; it was moderately intense and clearly weaker than the migraine without aura attacks, from which he also suffered. This headache thus had characteristics and a temporal pattern clearly at variance with those of a full-blown migraine attack. The migraine attacks, moreover, disappeared around 15 years ago.
With the exception of one spring when he was especially careful to avoid the smoke, the original pattern had continued in the same way in the 6-year follow-up period. The observation period duration and the strict temporal association with the particular smoke make it hard flatly to reject a causal relationship between this type of smoke and the headache. The difference between the clinical manifestations of this headache and migraine without aura count in the same direction.
Hydrogen sulphide (H2S) intoxication
A 40-year-old man, working at the sewage purification works during a 6-year-long period generally spent 4 h at a time and a total of approximately 7 h daily at the sewage works. During these years, he would have between six headache attacks per week and one attack per 2 weeks, usually of mild/moderate intensity (3+ to 4+) and usually of many hours’ duration. The worst headache appeared in the afternoon. By the next morning he would more or less have recuperated. Occasionally, the headache would ‘explode’: in the course of a minute or less, it would increase considerably in intensity, to attain a level corresponding to grades 4–5+ on a 0–6+ intensity scale (5), headache at this higher level lasting ≥0.5 h at such times. Occasionally, this would be accompanied by an offensive odour, but usually the odour could seem less offensive at such times. Pain-killers in high dosages would have only marginal effect in such situations. The headache would be pounding and bifrontal/bitemporal. At the peak, the pain could also be felt in the occipital/nuchal areas. Pain and pounding increased upon sneezing and bending forwards. There was no nausea/vomiting/photophobia/phonophobia, but slight dizziness. The headache even at this higher level would generally not lead to bedrest, but working capacity could probably be reduced by ≥30%. Blood pressure was 140/90. ‘CF’ was at 0.5+. He had no other headache, either during the actual period or prior to or after it. There was no family history of migraine.
Equipment for measuring air hydrogen sulphide concentration was then obtained. While the recommended upper level of H2S is at 10–15 p.p.m., the levels at work proved to be 100 p.p.m. Once this was discovered, counter-measures, such as increased ventilation (14), were introduced and kept the H2S concentration closer to the recommended upper level. This was also combined with shorter stays in the sewage purification plant. After these measures were adopted the headache disappeared, never to return, in spite of continuing the same work.
There were two other workers at the premises at the time: case 2, a 60-year-old male, also had headache, apparently related to work and, in the end, was transferred to other work because of this. He worked in Vågå, but at the time of the study he lived outside and was therefore not included (Table 1). The third man, 48 years old, claimed that he was headache free at the examination in connection with the Vågå study. He had worked at the premises for a number of years. Soon after the examination, however, he realized that he had had a daily discomfort all through these years. The global headache could mostly be characterized as ‘heaviness’/‘discomfort’ (2+), or even only as ‘minimal unpleasantness’ (1+), but at times there could be a ‘mild’ headache (3+) on the 0–6+ scale (5). It was in particular the improvement during a summer vacation that finally opened his eyes. He then also realized that through the years there had been recuperation even during weekends and a partial recuperation even during the night. He was finally transferred to other work, and the headache left him entirely. Cases 1 and 3 were followed up for 6–7 years.
Vocalist's headache
A 23-year-old carpenter was a vocalist in a dance music band as a youngster. Between 14 and 15, he experienced a headache that invariably appeared late into the night after several hours of what he termed ‘hard’ singing. The headache was global and intense, but was unaccompanied by nausea/photophobia, and there was no pounding sensation. Each episode lasted 2–3 h. Apparently, this headache differed entirely from migraine without aura, from which he also suffered at the time and still does. He had to stop singing in the band, whereafter this headache disappeared entirely. From around 27, he again could sing in a band, without any headache.
This headache did not seem to be a headache with a ‘vascular’ component. The ‘CF’ was 0 (6). The headache had the features of acute tension-type headache. Could it have been a headache secondary to ‘inadequate’ muscular activation?
Cold exposure headache
‘Wind headache’ (IHS 4.3.1)
Several parishioners (n = 7, Table 4) commented that cold wind could result in infrequently occurring, transitory and diffuse discomfort in the head, face and neck areas, usually of a few hours’ duration and without accompanying symptoms. The sufferers were mainly males and were engaged in outdoor activities, and the headache seemed to arise only upon this special exposure. The complaints were mild/moderate (3–4+), and the parishioners did not seem to place much emphasis upon them. One farmer (case 6) felt that cold wind was the only precipitant of this headache and that, on exposure, this particular headache would always be precipitated. He otherwise tolerated cold stimuli well; only the cold wind was intolerable to him. He had a somewhat fluctuating tendency to neck stiffness as an adult, which transiently worsened during seasonal tractor work (15). The wind headache seemed largely independent of the neck complaints. This farmer also had exertional headache and nuchal jabs (no jabs in the head) of 1–3 s duration (16). Neurological examination only revealed tenderness over the right trapezius muscle. ‘CF’ in the ‘non-tractor’ season was 0. Accompanying headaches, if any, are recorded in Table 4, to indicate that there was little likelihood that in any of these seven parishioners the wind headache could have been confused with a coexisting headache. The T-TH (in case 2) may be an exception.
Wind exposure headache
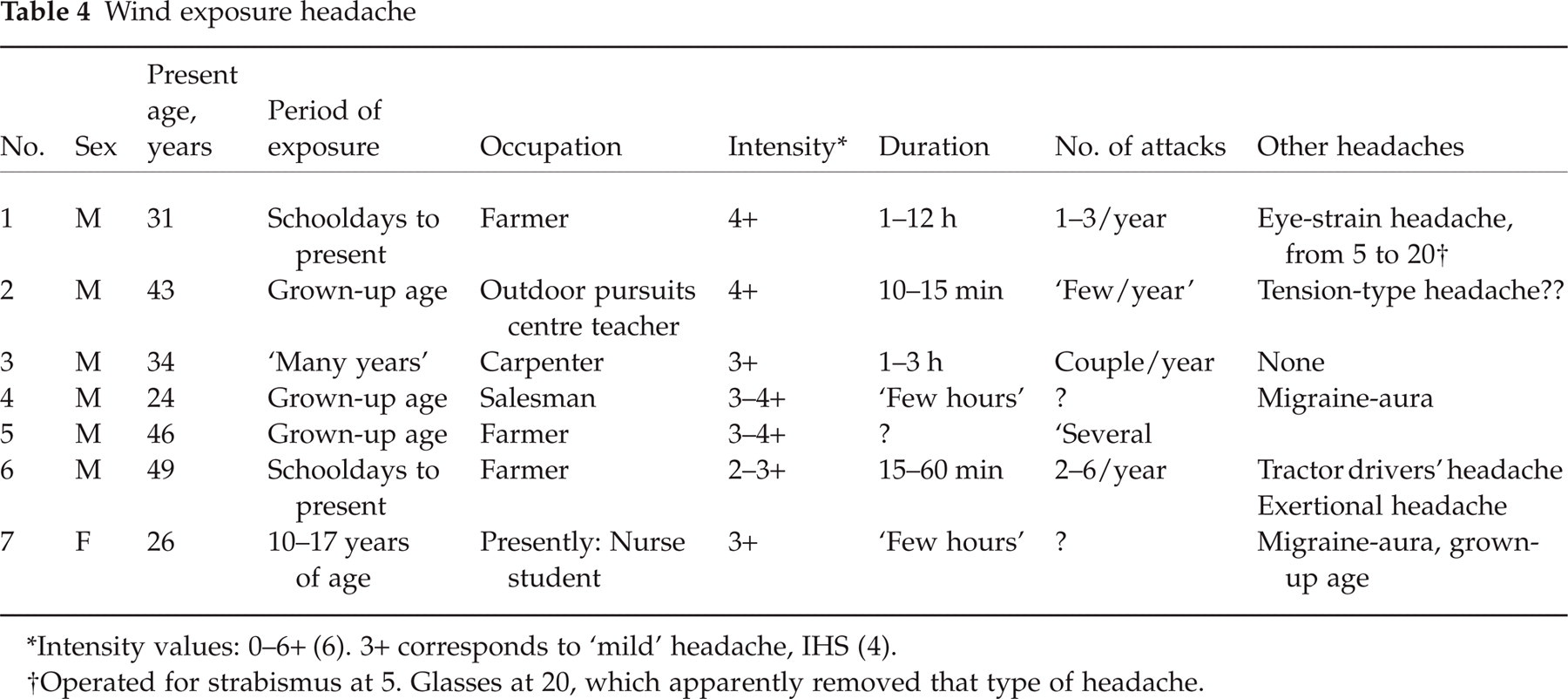
Operated for strabismus at 5. Glasses at 20, which apparently removed that type of headache.
Low swimming pool temperature headache
In a solitary parishioner, a 55-year-old man, relatively cold swimming pool water provoked generalized headache as a youngster, and he had to cease swimming at the time. The attacks appeared to be symptom poor, except for the global headache. As a 35-year-old man he no longer reacted negatively to cold water.
Coldness exposure—‘frozen hair
A variant of the cold exposure headache was reported by a 31-year-old carpenter. This parishioner was a ‘classic’ migraineur from the age of 18. At the age of 25 he went for a walk after a shower, on a cold winter day, and his hair froze to ice. He dates the actual headache back to this episode. He was completely unable to work for 2–3 weeks and had to use analgesics at the time. The headache was global, with a frontal maximum; it was chronic-fluctuating and up to moderately intense (4+) and was not accompanied by nausea/feeling of pulsation. The headache followed a protracted, decrescendo course and finally faded away after a few years of suffering. ‘CF’ was 1.5+ (mean, Vågå material: 0.79+ scale 0–5.0+ (6)). In this case, there seems to have been a one-time cold stimulus, with an ensuing, chronic-fluctuating headache, and not a repetitive headache after repetitive, stereotypical cold stimuli. This may be sort of a ‘Titanic’ syndrome: freezing of the hair after immersing in the cold waters of the North Atlantic.
It is hard to control the circumstances of this case. A better approach may be: has any one observed anything similar?
Ice-cream headache (4.3.2; IHS (4))—ice-cream headache during the Vågå study proper
Ice-cream headache was described by three parishioners (two females, aged 22 and 53 and one male, aged 40), corresponding to a prevalence of 0.16%. The male parishioner had experienced one solitary episode of moderate intensity. In the younger female, ice-cream and ‘quick soft-drinks’ would both ‘invariably’ provoke mild to moderately intense headache. In the last case, with no other headache, the ice-cream headache was repeatedly right-sided in the ocular and vertex areas. There was no nausea, photophobia, phonophobia or throbbing sensation in any of them. The headache lasted a few minutes only.
Telephone interview concerning ice-cream headache in Vågå
We suspected that the ‘real’ prevalence in Vågå could be considerably higher than 0.16%: our study protocol had probably not been sufficiently sensitive to catch all individuals with ice-cream headache. After ending the Vågå study, it was decided to explore this possibility, and the following ad hoc procedure was adopted: 50 parishioners who had all previously answered in the negative the questions: ‘any other headache?’/‘headache in other situations’ were randomly selected (27 females and 23 males) and contacted by telephone. The female/male ratio was 1.17, as against 1.05 in the whole Vågå series. Each of them was asked the following questions: ‘Have you at any time prior to the headache investigation in Vågå had any headache when eating ice-cream’? If so, ‘how frequent, intense, and long-lasting have the episodes been? And where was the headache located? Did you take precautions before eating ice-cream, such as waiting until the ice-cream had started melting – or: did you take small portions at a time?’. A clear-cut ice-cream headache was present in three of these 50 parishioners. In one of them it lasted for 5 min and in the other ones for <1 min. The headache seemed to be moderately intense and was located in the vertex area. In still another parishioner, there was a vague feeling (‘discomfort’, stage 2+ actually, the first step of head pain) in the forehead, lasting 0.5–1 min. This borderline case was also included, in spite of the mildness of the complaint, to give a prevalence of 8%. In another four there was a ‘discomfort’, but only in the teeth. Still another had discomfort, if too large and cold a piece of ice-cream was swallowed, but only in the upper neck, bilaterally, for which reasons he was not included. All four parishioners with headache during ice-cream eating had also noted transitory, dental pain.
The suspicion that the low initial prevalence had a methodological background was to a large extent verified: the figure obtained on the direct approach was 50 times higher than the original one.
Varnish intoxication
A 62-year-old man was at 34 exposed to newly spread/drying varnish for 3 days, on one solitary occasion. The varnish was spread over an extensive surface in the rooms; he had no particular protection and there was no extra ventilation. After some time of exposure, he developed a more or less continuous, frontal, moderate/severe headache without nausea, but with photo- and phonophobia and possibly some throbbing. After the exposure, the headache gradually faded away. At 62, blood pressure was 155/90; ‘CF’: 0.5+ (normal value). This patient otherwise had ‘no headache’, i.e. stage 0 (5).
High-intensity headache, coming ‘out of the blue’
This type of headache was dramatic and was reported to us spontaneously. Abrupt onset headache of high intensity had been experienced by four parishioners, three females and one male. In only one of them was the underlying diagnosis absolutely clear: subarachnoid haemorrhage due to a ruptured aneurysm, at 18 (a presently 47-year-old female). The bilateral, severe, throbbing pain disappeared completely after clamping of the aneurysm.
In the male, a professional rescuer, aged 42, the intense headache, which had a left-sided preponderance, reached a peak in ≤0.5 min and then followed a slow, decrescendo curve that reached the zero line within a ‘small week’ (at 40 years of age). His memory is incomplete concerning the very first part (probably a few minutes only) of this period. When he came to, there was a sensibility loss in the left side of the forehead up to ‘where the hair starts’ and this persisted for 5–10 min. A neurological examination approximately 2 weeks after the attack showed normal findings, for which reason no further investigations were carried out. He is presently in good shape, maintaining a full-time job, and still with a normal neurological investigation (headache category: 0).
The two other ones, 30 and 47 years old, experienced a sudden bilateral headache with unilateral preponderance. Both are, as far as we are concerned, non-classifiable.
Acute iridocyclitis
A 49-year-old woman had had acute iridocyclitis 5 years previously with bilateral affection. In addition to the ocular pain, there was a shortlasting supraorbital pain. The iridocyclitis left no sequelae.
Nose-bleed and headache
For the sake of completeness, a 62-year-old male parishioner is also mentioned. As a child, probably from approximately 11–13 years-of-age, he had an episodic (approximately once a month) global headache at the ‘heaviness’/‘discomfort’ stage (first stage of headache; stage 2 on a 0–6+ scale (5)). The headache was otherwise symptom poor and there were no autonomic phenomena. ‘Every time’ the headache was accompanied by nose-bleed. The side of the nose-bleed could no longer be remembered. There was a normal blood pressure (140/85) presently; ‘CF ‘was 0 (on a 0–5+ scale (6)). There were also normal findings upon neurological examination. There were no apparent signs of Osler's disease.
Discussion
It is the considered opinion of the authors that a time-consuming, face-to-face technique is probably the preferable (or only) way to obtain reliable/optimal data for prevalence as regards the panorama and complexity of rare and unexpected headaches. The investigator should be sensitive to all types of input in connection with the questions: ‘Other headaches?’; ‘headache in other situations?’. There are many pitfalls in this field, however, also when using this approach, as also demonstrated in the present study, in particular in connection with ice-cream headache.
Cooling the head
That various types of cold exposures may give rise to headache is well known. It has also been shown in experimental situations that coldness exposure as such to the vertex may cause headache (17). Similar mechanisms may be a rational cause for the wind headache, and also for the ‘frozen hair’ headache, as well as the low swimming pool temperature headache. The standard temperature in experimental cooling, as with ‘the cold pressure test’, has been +3–4°C. During a 1-min period, the one hand is exposed to cold water up to the wrist (18, 19). The difference between such a shortlasting exposure to 3–4°C water and a relatively long-lasting exposure to ice, as in the ‘frozen hair case’ may, nevertheless, be a significant one: the latter may lead to more drastic local consequences than the cold pressure test, first, since it was ice, and second, due to the proximity of the ice to the skull.
Negoro et al. (20) have recently described a ‘benign hot bath-related headache’ (n = 3, all females), a headache that Liao et al. (21) prefer to term ‘bathing headache’. These authors claim that any abrupt temperature change can underlie this sort of headache, also cooling. Even though the low swimming pool headache described herein is an essentially benign headache, it had the consequences that bathing was totally discontinued at the time. It is, furthermore, remarkable that after a considerable respite he no longer reacted to the same stimulus.
As regards wind headache, it took a considerable time before the wind headache manifested itself during the solitary episode. It did not seem to have the qualities of an abrupt, high-intensity headache (Table 4). It is, furthermore, remarkable that, in the present setting, this was a male headache.
Ice-cream headache
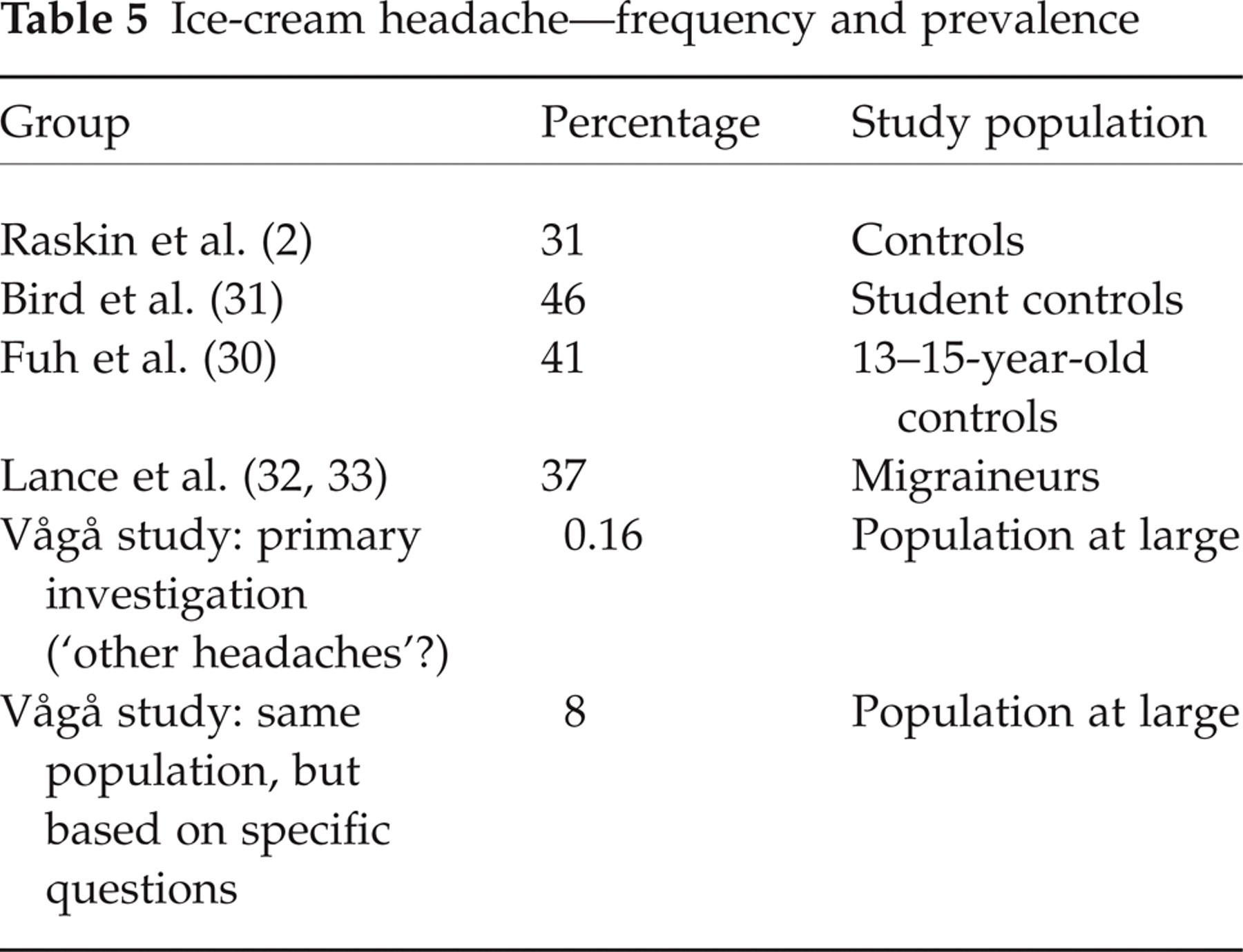
While in the initial study we found a prevalence of 1.6 per 1000, others have found a much higher prevalence, i.e. 31–46% (2, 22, 23) in control series (Table 5), while in migraineurs a frequency of 37% has been found (24, 25). The evidence that ice-cream headache is a frequent disorder is thus overwhelming.
Ice-cream headache—frequency and prevalence
The low prevalence in our original study seems, once more, to bring us to the core of what is headache epidemiology. In headache epidemiology, using a face-to-face technique, there may be principally three different ways of approaching a headache diagnosis: (i) one can ask about symptoms, such as nausea, vomiting, exact localization of the headache, frequency and intensity. These elements, when arranged in an orderly and meticulous way, may help in pattern recognition; (ii) with rather mono-symptomatic, and not too intense disorders, the already mentioned approach will not necessarily reveal the nature of the headache. A good example of this type of ailment is ‘jabs’ or ‘stabs’. In such a situation, it is better to ask one salient question: have you had a brief, stinging pain in the head (and/or the neck/face)? However, the situation may become more complex, e.g. in temporal arteritis. It would not be the correct approach, and hardly rewarding, to ask everyone in a broad headache survey: ‘have you had an “inflammatory” reaction in the temporal vessel on the one side, accompanied by elevated ESR’? There are many headaches, and time during such an examination is limited. One cannot include all headaches, asking pointed questions. One has to draw a line; (iii) there is a third way, a ‘buoy’, so to speak: asking rough, generalized questions, such as: ‘Other headaches’? or ‘Headache in other situations’? But then the net has ‘large meshes’. This approach may, nevertheless, give an occasional ‘catch’. Some strange headache pictures have shown up in such situations. There are various, clearly negative aspects of this technique: one may preferably get hold of those who recently had such complaints; or those with a low pain threshold. One should therefore not expect exact prevalence figures from this approach, but it may give a hint, something to work further on.
This may serve as a background to our handling of the ice-cream headache problem.
We only asked: ‘Other headaches?’, ‘Headache in other situations?’, as regards this headache. And we have been severely punished for having handled the matter in this way. Our ‘defence’? Time is limited during the examination in an epidemiological headache study. Furthermore, we have never primarily been contacted regarding ice-cream headache. This headache has come up as a separate issue, probably only in a total of 10–20 consultations during our professional lives. Why? Such patients probably immediately understand the nature of the headache and that they themselves are the proper persons to take care of it. A physician would hardly have much to contribute. This assumed patient attitude has been transferred to us: ice-cream headache, as such, is probably a minor, highly transitory complaint, not worthy of extra attention during a busy (epidemiology) examination.
The discrepancy between our initial data (0.16%) and those in pre-existing surveys (a mean of 39%) is enormous (Table 5). The discrepancy clearly derives from differences in methodology. The discrepancy between our later result (8%) and the mean prevalence in previous studies is still considerable and may partially depend upon definition of what ice-cream headache is, in particular its ‘severity’. Is there a ‘mild’/‘moderate’ pain; is there only a ‘minimal unpleasantness’ (grade 1+), or is there simply a feeling of ‘coldness’? This is probably the main issue, as far as prevalence is concerned. In the present study, only those with pain, i.e. ≥2+ on a 0–6+ scale, were included and only those with a pain in the head. If that has been the case also in the other mentioned series, then a real discrepancy may exist between people in heavily populated areas around the world and those in the rural, mountainous area of Scandinavia.
The situation may appear to be exactly the opposite of the one encountered with regard to jabs. In our study, the prevalence of jabs was 35.2% (26). In two other studies, also based on a face-to-face interview technique, the results were 2% and 0.2%, respectively (27, 28). The present experience makes us suspect, even more strongly than before (26), that while we specifically ‘went for’ the jabs, the two other studies may not have had that specific objective and therefore only/mainly detected those who spontaneously mentioned their jabs.
In rare or not so important headaches with clear characteristics, simple questionnaire studies with clearly defined aims can render reliable results, just as in Fuh and coworkers’ study of ice-cream headache (22)—provided the intensity problem is handled in a rational way.
Hydrogen sulphide headache
Decay of organic, sulphur-containing material, e.g. sewage, manure/dung and compost, gives rise to hydrogen sulphide. Stirring of such material and non-ventilated facilities can increase the ambient air concentration of the gas. H2S is above all a respiratory tract toxin, since absorption through skin is negligible. It inhibits reversibly the cytochrome oxidase at the end of the respiratory chain, in aerobic cell mitochondria (29–31). This may explain its toxicity. In the body, it is rather quickly degraded metabolically and does not accumulate. Accordingly, it has little long-term effect, provided focal brain lesions are evaded at peak concentrations, e.g. in the lentiform nucleus. Low concentrations of H2S (0.2–1 p.p.m) cause an irritant, unpleasant odour of the ‘rotten egg’ type (29, 30). At around 10 p.p.m., additional eye soreness is noticeable. At around 50 p.p.m., respiratory tract symptoms appear. What makes H2S such a sinister toxin is that at ≥100 p.p.m., the olfactory bulb is paralysed, and the offensive odour then disappears entirely (29). The intoxication may from then on be insidious (32). Maximal allowable concentrations under working conditions are considered to be around 10 p.p.m. (29, 30). Others have mentioned standards clearly lower than this (33). Ambient air concentrations of >50 p.p.m. necessitate immediate evacuation (29).
Headache is mentioned as a symptom of H2S intoxication (29–31, 33), together with weakness, lethargy, nausea, dizziness, but possibly mostly from 300 to 500 p.p.m. in acute situations. A 0.5–1-h exposure will at these (or lower) concentrations cause headache, followed by unconsciousness and respiratory failure. An exceptional finding was made by Kangas et al. (14), who reported more headache among those exposed to up to 20 p.p.m. of H2S than among unexposed ones. However, the authors seem to be in doubt about the significance of their finding. It should, nevertheless, be stressed that 20 p.p.m. has been stipulated as the maximum allowable concentration for 8-h exposure, and even as a ‘ceiling limit’ for shorter exposures, i.e. 15 min (32).
The H2S intoxication/headache interrelationship is a critical one and brings us to the core of what is headache epidemiology research at the grass-roots level. The first author had previously barely heard about headache caused by H2S and had little idea about what a 100 p.p.m. concentration of H2S meant. Accordingly, a large question mark was put behind the story of case 1 at the first examination. The most-affected parishioner (case 1) allegedly worked with H2S air concentrations of up to 100 p.p.m. The H2S air concentrations did apparently not reach the levels at which headache will definitely be generated, according to the literature. The headache he experienced was intermittent. The temporal aspects, nevertheless, seemed to indicate a cause-and-effect relationship. Could it be that the technical equipment was not functioning properly or that the measurements were not taken at the right locations, i.e. that the odour disappeared at times? Or could relatively low concentrations cause toxic effects with longer exposures?
When re-engaging with this topic 4 years after completing the field work in Vågå, one started wondering: was it really exactly 100 p.p.m.? It was! And more times? Every time! Never slightly above or below? Well, it could not be above: the scale went to 100 p.p.m.! It then proved that the indicator went up to 100 p.p.m. with great speed and stayed there. In other words, the concentration was never below 100 p.p.m., but it could have been considerably higher. The correct levels of H2S at the time will never be known.
The latter information led us to explore further among the other workers at the premises at the time. Cases 2 and 3 would not have been discovered unless: a follow-up was made after 4 and 6 years, respectively, as regards case 1, but concerning the time prior to examination (i). One originally started to have suspicion regarding case 1 as a consequence of the question: ‘headache in other situations?’, and the follow-up was extremely meaningful. In case 3, there was no positive response to this question initially, and cases 2 and 3 could thus easily have gone by unregistered. Such a headache could, of course, have been detected, even en masse in an inquiry among sewage plant workers, where the plant was not functioning at an optimal level. The focus of interest could then be directed towards this problem only, and specific questions could have been asked. This type of policy was not within the scope of the Vågå study: we did not even know that this problem existed in Vågå. The whole problem could therefore easily have been neglected in the Vågå study. A general headache questionnaire, without personal contact, would in all probability have led to a total failure as regards H2S headache.
Comment on grass-burning
The influence on human health (34) of gas from burning grass fields has not been known, at least not up to 1987. At that time, apparently neither the gas composition of slash burning in the ‘summer burning season’, nor its quantitative contribution to the particulate air pollution, was known. By now, the gas from garden trash burning has been analysed (35), i.e. left-over grass, leaves and loppings from trees, in other words, a composite made up by several constituents, admittedly somewhat different from grass, of the ‘grass-burning’. The composition of the gas and composite products from garden trash-burning (10 kg) was found to be approximately: 1 kg of CO; 1 kg of ashes, soot/carbon deposits; 25 g aldehydes; and 5 g of PAH compounds (35). As far as the grass-burning is concerned, one might also wonder whether hydrocarbons, such as methane, would be a component of the smoke. The highest ‘allowable’ atmospheric CO concentration has been given as 25 mg/m3 (criteria proposed for Norway) and 35 p.p.m. (EU). The CO concentration in the smoke from trash-burning may exceed the CO concentration in the ambient air in a narrow street with heavy, but slow traffic (by 3–4 times (35)). CO binds to haemoglobin with an affinity ≥230 times that of O2. An ambient air CO concentration of 35 p.p.m. may lead to 5% carboxyhaemoglobin (29). Symptoms such as headache reportedly begin at 10–20% carboxyhaemoglobin (36). The carboxyhaemoglobin concentration will, nevertheless, clearly depend upon many factors, e.g. total exposure time.
From the literature, we have not been able to extract much information regarding headache in the acute situation. The acute symptoms of CO intoxication are: weakness and apathy. The chronic symptoms are: severe headache, abdominal pain, nausea and vomiting. Warehouse workers’ headache is well known (29): headache due to increased CO concentrations in enclosed warehouses, the CO being generated by propane-fuelled forklifts. In our case, the exact concentration of the CO in the actual, inhaled smoke cannot be stipulated, but the case history is suggestive of a causal relationship between smoke and headache. If so, it is likely that the headache was mediated through the production of CO (and carboxyhemoglobin).
Conclusion
The present study is of a descriptive nature and is not an analytical study. The findings represent prevalence estimates of some established headache diagnoses. However, the study also seems to have generated hypotheses, which in their term ought to be tested in particularly designed studies.
The grass-burning headache and the headache following exposure to H2S are examples of poorly defined headaches. The present authors previously had vague ideas about H2S headache and had never heard about anything similar to the grass-burning headache. H2S headache has been well known in connection with drastic intoxications in industrial catastrophes, but then in connection with other major symptoms of intoxication. In the present situation, a more low-grade, protracted H2S exposure had taken place. Headache under such conditions is to the best of our knowledge only poorly known, if at all.
This study served only to identify these rare headaches. It is therefore out of the question that these two types of headache could have been the focus of interest from the beginning of the present study.
Already in the next round, however, such headaches can be the focus of interest; grass-burning headache questions to farmers and H2S headache questions to purification plant workers. At that stage, even questionnaires can be used, once the problems (headaches) have been identified. To emphasize our position: we consider H2S headache to be a definite, rare headache; grass-burning headache, with only one case, would certainly need some corroboration. Also in future research, the present approach would be a valid one to conduct a survey of the total situation in a community. Absolutely exact figures can generally not be expected with this approach. The figures for wind headache, nitroglycerine, H2S, and ice-cream headaches are probably more valid ones.
Footnotes
Acknowledgements
We are indebted to GlaxoSmithKline of Norway, Pharmacia & Upjohn, and the Alf Harborg Foundation, Department of Neurology, St Olavs Hospital, Trondheim, Trondheim University Hospitals, for generous support during the various phases of the investigation. The authors are also grateful to the personnel at the Vågå Health Centre at Vågåmo for their aid. Last, but not least, we thank the inhabitants of the Vågå commune for their collaboration.