
Abstract
We conducted a two-stage population-based headache survey among subjects aged ≥15 in Taipei, Taiwan. Subjects with chronic daily headache (CDH) in the past year were identified, interviewed and followed-up. CDH was defined as a headache frequency > 15 days/month, with a duration > 4 h/day. Of the 3377 participants, 108 (3.2%) fulfilled the criteria for CDH, with a higher prevalence in women (4.3%) than men (1.9%). TM was the most common subtype (55%), followed by CTTH (44%). Thirty-four per cent of the CDH subjects overused analgesics. At the 2-year follow-up, 35% of the CDH subjects still had CDH. The significant predictors for persistent CDH at follow-up included: older age (≥ 40 years) (RR = 2.4), CDH onset after 32 years (RR = 1.8), CDH duration ≥6 years (RR = 2.0), medication overuse (RR = 1.8), and ‘daily’ headache (RR = 2.1). We found that CDH is not uncommon in the community and its prevalence is similar among different populations. Older subjects and those with medication overuse may have a more protracted course of illness.
Introduction
Frequently encountered in neurology practice and headache centres are patients with chronic daily headache (CDH), a heterogeneous headache disorder that occurs daily or near daily for a prolonged period of time (1, 2). Among these patients, medication overuse and psychiatric disturbances are common (2–4). CDH has a great impact on quality of life (5, 6) and is an important health issue. Despite this, CDH was not included in the 1988 classification system of the International Headache Society (IHS) (7–9). Silberstein et al. proposed revised criteria for CDH, including transformed migraine (TM), chronic tension-type headache (CTTH), new daily persistent headache and hemicrania continua (10). The criteria successfully classified all patients with CDH in their headache centre (10).
While several clinic-based studies have identified TM as the most common subtype of CDH in headache centres (2, 10, 11), the epidemiology of CDH in the general population has not been fully described. Recent epidemiological surveys have found that CDH was not uncommon in the general (12, 13) or in the elderly population (14, 15). However, the leading subtype of CDH was not consistent among these studies, and little is known about the outcome of CDH subjects in the field.
From August 1997 through to June 1998, we conducted a population-based headache survey in the Greater Taipei area of Taiwan. Part of the results were published elsewhere (16). The present report focuses on CDH, including the prevalence and 2-year follow-up data.
Methods
A population-based headache survey was conducted among subjects aged ≥15 years in each randomly selected household sampled from the Greater Taipei area in Taiwan. According to the government's data in the 1996 years-end population structure, there were 1.83 million households and 4.6 million people aged ≥15 years in the Greater Taipei area (17). In order to obtain at least 1000 respondent households for this study, we planned to sample 1400 households based on the population structure. We adopted a stratified systematic random sampling method that has been described in detail elsewhere (16). The household sampling rate was calculated to be 0.075%.
Overall, 1211 households (86.5%) responded. Of the 4434 eligible subjects in the respondent households, 3377 subjects (76.2%) (1804 women, 1573 men) completed the questionnaire survey and were the participants of this study. The mean age of the participants was 37 ± 15 years (range 15–92 years) (Table 1).
Summary of demographic data in CDH subjects vs. all participants
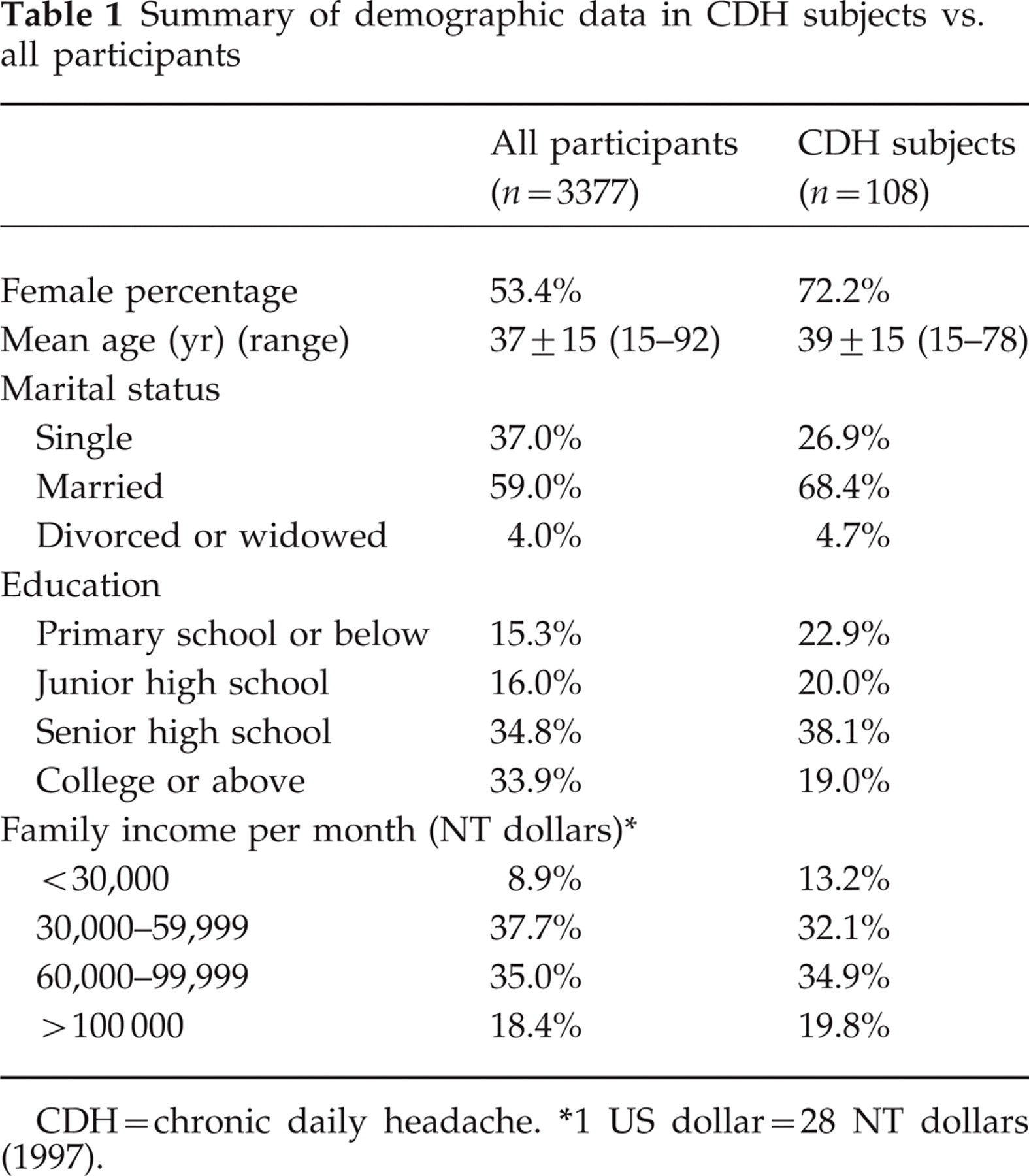
CDH = chronic daily headache.
1 US dollar=28 NT dollars (1997).
First stage: questionnaire screening
The first-stage headache questionnaire survey was conducted from August 1997 through to June 1998. Our interviewers visited the eligible subjects (aged ≥15 years) in the sampled households. The study objectives were explained and, after gaining permission, the questionnaire was administered to each participant by our interviewers.
The screening questionnaire consisted of three parts. The first part was demographic characteristics. The second part was headache profile, which was designed to comply with the IHS criteria for migraine (9). The third part questioned the participants about painkiller usage, physician consultations for headache (categorized as 0, 1, 2, … 8, 9, ≥ 10 times/year) and mental health (30-item version of the Chinese Health Questionnaire, CHQ-30). Modified from the General Health Questionnaire, the CHQ-30 was used for screening minor psychiatric morbidity (MPM), i.e. non-psychotic psychiatric or neurotic symptoms, in the population (18). Each item of the CHQ-30 queries one recent psychiatric or somatic symptom, and a 0–1 scoring method was applied on each item. A total score of ≥10 was associated with MPM (‘cases’), with a sensitivity of 76% and specificity of 77% (19). In this study, we used the CHQ-30 to measure psychological distress.
Second stage: physician interview and identification of CDH subjects
The second-stage study started immediately after the questionnaire screening was completed. All subjects who reported having a headache frequency of ≥3 days/week in the previous year were selected. This cut-off value (≥ 3 days/week) allowed more potential subjects to be screened, so the report bias could be minimized. Our physicians conducted a semi-structured telephone interview with these subjects to ensure that the headache features fulfilled the criteria for CDH (headache frequency > 15 days/month with duration > 4 h/day), and if they had medication overuse (10). Based on the interview data, those with CDH were enrolled and classified using the following criteria.
Diagnosis and classification of CDH
If the subjects had CDH, i.e. a headache frequency > 15 days/month and duration > 4 h/day if untreated, a subtype of CDH was diagnosed based on the criteria proposed by Silberstein et al. (10). In our study, CDH was classified into three mutually exclusive diagnoses: TM, CTTH and ‘other CDH’. TM was diagnosed if the subjects fulfilled the following criteria (10): > 15 headache days/month for > 1 month; duration > 4 h/day if untreated; and at least one of the following: either a prior history of IHS migraine, current headache meeting all the criteria of IHS migraine other than duration, or a history of increasing frequency coupled with decreasing migraine symptoms for at least 3 months. A diagnosis of CTTH (10) was made if the subject had: headache for > 15 days/month for ≥ 6 months, duration > 4 h/day if untreated; and at least two of the following characteristics: a pressing/tightening quality, mild or moderate in severity, bilateral location, or no exacerbation on movement; no vomiting; and no more than one characteristic of nausea, photophobia or phonophobia. Subjects who met the criteria for both CTTH and TM were classified as TM. In contrast, CDH subjects who did not fulfil the criteria for either TM or CTTH were classified as ‘other CDH’.
Medication overuse
Based on the interview data, CDH subjects were considered to be overusing analgesics if they met one of the following criteria (10) for at least 1 month in the past year: use of simple analgesics (> 1000 mg of aspirin or acetaminophen) > 5 days/week; use of combination analgesics (caffeine, barbiturate-containing medication) (> 3 tablets per day) > 3 days/week; use of narcotics (> 1 tablet per day) > 2 days/week; or use of ergotamine (1 mg orally, or 0.5 mg per rectum) > 2 days/week.
Follow-up
From July through to December 1999, 2 years after the initial questionnaire survey, our physicians contacted all the enrolled CDH subjects via telephone and queried their current headache profile and usage of analgesics.
Statistical methods
Statistical analysis was performed using the Statistical Products of Service Solution (SPSS) software, version 10. The prevalence of CDH was reported as the number of cases per 100 persons with 95% confidence intervals (CI). Age- and sex-specific prevalence were also calculated. Student's t-test and chi-square test were used for comparison when appropriate. The potential predictors of poor outcome in this study, defined as the persistence of CDH at follow-up, were analysed. The outcome predictors were presented as relative risks (RR). A P-value of less than 0.05 was considered statistically significant.
Results
During the first-stage questionnaire screening, 2082 (1289 women, 793 men) of the 3377 participants had had at least one headache in the previous year. Of them, 233 subjects reported an average headache frequency of ≥3 days/week during the previous year. These subjects were further interviewed by our physicians via telephone.
Figure 1 shows the clinical confirmation process for CDH. Thirty-three subjects (14%) were unable to be contacted; these non-responders did not differ from responders in age (41 ± 15 vs. 40 ± 15 years) and sex (females 64% vs. 74%). Of the 200 subjects (86%) who completed our physician interview, 108 (54%) were diagnosed as CDH; the other 92 were excluded because their headache frequency (n = 76) or duration (n = 16) did not meet the criteria for CDH (Fig. 1).

Flow chart of the diagnostic process of chronic daily headache (CDH).
Prevalence of CDH
The 1-year prevalence of CDH was 3.2% (108/3377) (95% CI 2.6–3.8%). Sixteen subjects (13 women, 3 men) (0.5% of the participants and 15% of the CDH subjects) reported that their headaches were daily, i.e. 30 days/month. The demographic data of our CDH subjects are shown in Table 1. Seventy-eight (72%) CDH subjects were women and were younger than the male CDH subjects (37 ± 14 vs. 44 ± 15 years, P < 0.05). The 1-year prevalence of CDH was 4.3% (95% CI 3.4–5.2%) in women and 1.9% (95% CI 1.2–2.6%) in men.
Subtypes of CDH
TM was the most common CDH subtype (n = 59), accounting for 55% of all CDH subjects and 1.7% of all participants. Forty-seven subjects (44% of all CDH subjects and 1.4% of all participants) met CTTH criteria. Two subjects (both males, aged 23 and 63 years) who failed to meet the criteria for either TM or CTTH were classified as ‘other CDH’. Among women, TM was more common than CTTH (TM 2.8%, CTTH 1.6%); among men, CTTH was more common (CTTH 1.2%, TM 0.6%), due to the increase of CTTH subjects after age 40 (Fig. 2).

Prevalence of CDH in different age groups. ▪, transformed migraine; (shaded box), chronic tension-type headache; □, chronic daily headache.
The mean ages of the subjects with CDH subtypes were: TM, 37 ± 14 years and CTTH, 42 ± 15 years. The mean age of CDH onset was 30 ± 12 years for TM and 35 ± 14 years for CTTH (all CDH: 32 ± 13 years). The mean duration of CDH was 6.0 ± 5.4 years for TM and 6.6 ± 7.9 years for CTTH (all CDH: 6.3 ± 6.6 years). A higher female to male ratio was noted in subjects with TM (5.6:1), in contrast to that of CTTH (1.5:1).
Medication overuse
Thirty-seven (23 women, 14 men) (34%) of the 108 CDH subjects met the criteria for medication overuse (> 1 month) (10). Of them, 65% (24/37) had overused analgesics > 6 months in the previous year. Medications overused included simple analgesics (46%) and compound analgesics (54%). None of the CDH subjects overused narcotics or ergotamine during the survey. Over-the-counter was the most common source of these analgesics (73%), followed by prescription (22%) and both (5%). Compared with non-abusers, medication over-users were older (45 ± 15 vs. 36 ± 14 years, P < 0.005) but neither differed in sex distribution or subtypes of CDH.
The majority (58/67, 87%) of the CDH subjects without medication overuse reported that they did not use any painkillers until the headache became ‘truly big or annoying’. In contrast, 46% (16/35) of the subjects with medication overuse admitted that they took painkillers even when their headaches were trivial, because: ‘I have to stop the headache before it gets bigger’ (n = 8), ‘I can not tolerate any functional limitation at all’ (n = 5) or ‘I can not tolerate any pain at all’ (n = 3).
Physician consultation for headache
Sixty-one (57%) subjects with CDH had consulted physicians for their headaches during the previous year, including 20 (19%) having consulted physicians for ≥ 10 times. Family doctors were the most frequently consulted physicians (41%), followed by neurologists (28%). Among the subjects who had consulted physicians, only 5% (3/61) had been treated with headache-preventive agents.
To estimate the numbers of physician consultations, we assigned a value of 10 in the analysis if the consultation number was ≥ 10. The resulting number of physician consultations per year among CDH subjects was 3.1 (TM 3.3, CTTH 3.0).
CHQ-30
Subjects with TM had higher CHQ-30 scores (13.2 ± 8.2) than those with CTTH (7.5 ± 6.5) (P < 0.001). The percentage of ‘cases’ (CHQ score ≥10) was also higher in subjects with TM (66%), compared with that of CTTH (36%) (χ2 = 9.4, d.f. = 1, P < 0.005).
Follow-up
Of the 108 CDH subjects, 106 (77 women, 29 men) (98%) were successfully followed-up after 2 years. Thirty-seven subjects (24 women, 13 men) (35%) still had CDH. Of them, 20 (13 women, 7 men) (54%) had medication overuse. On the other hand, 69 subjects (53 women, 16 men) (65%) no longer had CDH at follow-up; their mean headache frequency was 4.1 (0–12) days/month.
Of the 37 subjects with medication overuse identified at the initial survey, 36 were available for follow-up. Of them, 16 (44%) continued overusing analgesics and still had CDH two (6%) had stopped overuse but were still bothered by CDH, and the remaining 18 (50%) were free from CDH and no longer overused analgesics. Fifty-eight per cent (11/19) of those who overused compound analgesics still had persistent CDH at follow-up, compared with 41% (7/17) of those who overused simple analgesics.
For the calculation of RR, we used the mean values of continuous variables as dichotomous cut-off points. Five predictors of poor outcome, i.e. the persistence of CDH at 2-year follow-up, were found: older age (≥ 40 years), later CDH onset (≥ 32 years), longer CDH duration (≥ 6 years), medication overuse, and ‘daily’ headache (30 days/month) (Table 2). In contrast, gender, CDH subtypes and the psychiatric ‘cases’ (CHQ ≥ 10) were not significant predictors.
Prognostic factors for the persistence of CDH at follow-up
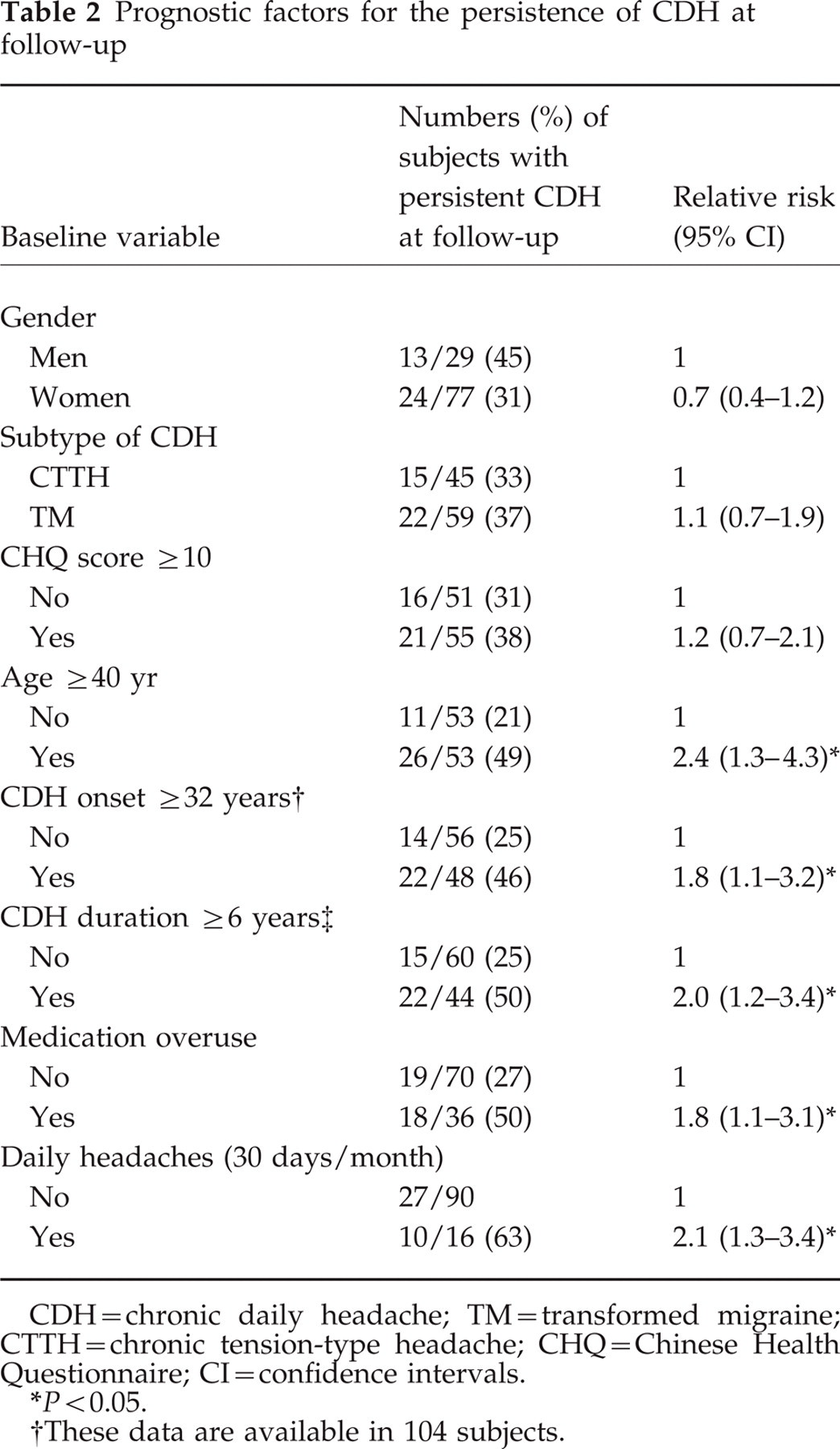
CDH = chronic daily headache; TM = transformed migraine; CTTH = chronic tension-type headache; CHQ = Chinese Health Questionnaire; CI=confidence intervals.
P < 0.05.
These data are available in 104 subjects.
Discussion
There are several major findings in this study. The 1-year prevalence of CDH was 3.2%, with TM as the most common subtype (55%). The prevalence was higher in women (4.3%) than men (1.9%). Medication overuse was found in 34% of our CDH subjects. At the 2-year follow-up, one-third of the CDH subjects still had persistent illness, especially the older subjects, or those with medication overuse and ‘daily’ headache.
Due to a 14% loss rate at the second-stage survey, our prevalence of CDH (3.2%) was slightly under-estimated. Despite this, our result was comparable with those of previous population-based studies: 4.1% in the United States of America (USA) and 4.7% in Spain (12, 13). Intriguingly, two CDH studies (14, 15) conducted in the elderly (≥ 65 years) also revealed similar figures (3.9% in Kinmen, Taiwan and 4.4% in Italy). These findings suggest that the prevalence of CDH may be rather consistent in different populations and, unlike that of migraine, does not decrease with age.
In contrast to the consistency in CDH prevalence, the leading subtype of CDH differs among studies. TM was slightly more common than CTTH in this study and studies done in Spain and Italy (13, 15), while the opposite was found in the USA and Kinmen, Taiwan (12, 14). Although TM is the most common subtype of CDH in headache centres, the leading subtype in the communities is at present inconclusive. We also found a gender difference between TM and CTTH; that is, more women than men had TM and the reverse for CTTH. This finding is similar to our experience in a headache clinic (6) but has not been reported in previous surveys.
Our finding suggested that 1.1% (37/3377) in the population had CDH with analgesic overuse. This figure was similar to the 1.0–1.7% recalculated from previous studies (13–15) and 1.6% of one recent report (20). Only one-third of our CDH subjects overused medication, compared with the 70–80% found in clinic-based samples (4, 21). Medication overuse therefore might be over-represented in headache centres. In this study, 44% of medication over-users reported that they took painkillers even when the headaches were still minor. Their low tolerance to pain may predispose them to painkiller misuse and rebound headache. Moreover, physicians in Taiwan are not familiar with the concept of drug-induced headache. Few of our CDH subjects had received headache-prophylactic treatment, and in 27% of our medication over-users, the painkillers were prescribed by physicians, i.e. of ‘iatrogenic’ origin. To avoid the misuse of headache medication, education for both patients and doctors would be of equal importance.
We found that TM subjects had higher CHQ scores than CTTH subjects. This result is compatible with our experience in a hospital-based sample (6). TM subjects, whether in headache clinics or the community at large, do suffer greater psychological distress than other headache subjects.
As most of our subjects did not receive any specific headache treatment, it is not possible to evaluate the impact of prophylactic treatment upon the outcome of CDH subjects in this study. However, the follow-up results may represent the natural course of CDH. One-third of our CDH subjects had persistent illness at the 2-year follow-up. This suggests that CDH is a fluctuating illness in the community; it may wear off, or persist for years without remission. We are unaware of the reason why older subjects (≥ 40 years) had poor outcomes at follow-up, but this finding is consistent with our previous field study, where two-thirds of elderly CDH subjects (≥ 65 years) had persistent illness after 2–4 years (14). Older subjects with CDH may have a more protracted course that justifies an intensive treatment programme. Medication overuse was also a poor outcome predictor in our survey of elderly subjects with CDH (14). However, overuse might be an epiphenomenon of intractable CDH, rather than the cause of CDH transformation.
The current criteria of CDH (10) cover a spectrum of subjects with variable headache frequencies (16–30 days/month). While most patients in headache clinics suffer ‘daily’ headaches, only a small portion of community CDH subjects do (15% in our CDH samples and 37% in the USA study (12)). As a result, the prognosis of CDH subjects without specific headache treatment was not bad in this study: only 35% had persistent CDH (however, 63% in those with ‘daily’ headaches). We suggest using the prognosis of our ‘daily’ CDH subjects as a reference when comparing with hospital CDH patients. It has been reported that 60% to 80% of hospital CDH patients continued to do well after specific headache treatment (22). This favourable outcome stresses the importance of specific headache management.
Some methodological issues should be addressed here. First, since the study was designed and described as a headache survey, the decision to participate may be influenced. Subjects with frequent headaches were more likely to join the study than those without headache. Nonetheless, our interviewers had tried their best to recruit all the eligible subjects in the respondent households to decrease this bias. Secondly, the clinician-confirmation rate of CDH at the second-stage survey was lower (54%). This was because we used a ‘loose’ cut-off value (3 days/week) for screening that optimized detection sensitivity at the price of case-ascertainment rate. In fact, many subjects who reported having three headache days per week did not actually have CDH: after physician interview, only 30% of them fulfilled the frequency and duration criteria for CDH. On the other hand, the clinician-confirmation rate of CDH was much higher (72%) in those reporting four–seven headache days per week.
Thirdly, medication overuse may be underestimated as headache subjects usually under-report it. Although we used clinician interviews to reduce this report bias, it might be inevitable in this study where information depends on self-reporting. Fourthly, the physician interview was conducted via telephone. The telephone interview could not replace face-to-face evaluation; nor could it rule out the possibility of secondary headaches. However, in a population-based study that included clinical evaluation (13), secondary headaches were rare, so we expect the influence of this factor to be small.
Footnotes
Acknowledgements
This study was supported by National Health Research Institute grants (DOH86-HR-633, DOH87-HR-633 and DOH88-HR-633) and Taipei Veterans General Hospital grants (VGH-368).