
Abstract
Previously, we described a large Dutch family with hereditary vascular retinopathy (HVR), Raynaud's phenomenon and migraine. A locus for HVR was mapped on chromosome 3p21.1-p21.3, but the gene has not yet been identified. The fact that all three disorders share a vascular aetiology prompted us to study whether the HVR haplotype also contributed to Raynaud's phenomenon and migraine in this family. Whereas the parent-child transmission disequilibrium test (TDT) did not reach significance, the sibling TDT revealed that the HVR haplotype harbours a susceptibility factor for Raynaud's phenomenon and migraine. Identification of the HVR gene will improve the understanding of the pathophysiology of HVR, Raynaud's phenomenon and migraine.
Introduction
Migraine is a common neurovascular headache disorder affecting up to 18% of the general population (1, 2). The aetiology of migraine is complex, with probably various environmental and susceptibility genes involved (3, 4). Migraine can also be part of autosomal dominant cerebrovascular syndromes, such as CADASIL and hereditary vascular retinopathy (HVR) (5–7). Identification of genes involved in these cerebrovascular syndromes may therefore contribute to the understanding of migraine pathophysiology as well. Recently, HVR was mapped to chromosome 3p21.1-p21.3 in a large Dutch family (8). Retinopathy in this family is characterized by microangiopathy of the retina, accompanied by microaneurysms and telangiectatic capillaries that appear preferentially around the macula and the posterior pole (9). In later stages, capillary occlusions may develop leading to retinal ischaemia and neovascularization. Leukoencephalopathy was seen on magnetic resonance imaging scans in some patients (7). Genetic testing revealed that two additional families with autosomal dominant cerebroretinal vasculopathy (CRV) and hereditary endotheliopathy with retinopathy, nephropathy and stroke (HERNS), respectively, were also linked to this locus (10, 11). Despite the fact that all three families were linked to the locus, there was a considerable variation in clinical symptoms between the families (8, 10, 11). The presence of different haplotypes suggests that the clinical variation might be related to different mutations in the same gene, although we cannot definitely exclude that different genes in the same chromosomal region may be involved in the three families.
Migraine was investigated and reported in the HERNS and HVR families (7, 11). Raynaud's phenomenon, which is an episodic pathological vasomotor reaction of the digital vessels, was investigated and reported as a predominant feature in the HVR family (7). Currently, no genes have been identified for Raynaud's phenomenon, and only one linkage study for Raynaud's phenomenon has been performed (12). Several linkage and association studies have been done for migraine, but no involvement of the 3p21.1-p21.3 region has been reported (13–20). Here we tested whether the haplotype cosegregating with HVR in the Dutch family also contributed to increased susceptibility for migraine and Raynaud's phenomenon using parent–child and sibling-based transmission disequilibrium tests (21–26).
Materials and methods
Diagnosis of patients and family members
Detailed clinical information on the extended Dutch HVR family was published previously (7, 8). In total, 198 of the 289 family members were personally interviewed and information on the other individuals was obtained indirectly through relatives. Retinopathy was diagnosed by ophthalmological examination, supplemented with fluorescence angiography of both eyes (9). Migraine diagnosis was made based on a standard questionnaire, using the criteria of the International Headache Society (IHS) (27, 28). The diagnosis of Raynaud's phenomenon was made according to standardized criteria of Miller et al. (29). All persons gave written informed consent and medical ethical approval was obtained from Leiden University Medical Centre (LUMC).
Genotyping
For genotyping, genomic DNA was extracted from peripheral blood using a standard salting out extraction method (30). To determine the presence of the HVR haplotype, DNA samples of 254 family members and spouses were genotyped for three genetic markers of the 3p21.1-p21.3 region; D3S3564, D3S1581 and D3S1289 (8). All primer sequences are available through The Genome Database (http://www.gdb.org/). Polymerase chain reactions (PCRs) were performed in 15 µl reaction volume, containing 1.5 µl 10 × PCR Buffer II (Applied Biosystems, Foster City, CA, USA), 1.5 µl MgCl2 (25 m
Statistical analysis
A parent–child trio analysis was performed based on the principle of the transmission disequilibrium test (TDT) (21, 23). In TDT analysis the probability of transmission of the HVR haplotype is compared with the expected probability of 0.5. All trios in which a single parent is heterozygous for the HVR haplotype and the child is affected with migraine and/or Raynaud's phenomenon were selected from the HVR pedigree. Trios in which an affected child was also a heterozygous parent for a trio in a subsequent generation were excluded (31). Accordingly, the TDT test is not biased by the fact that the trios are related. To evaluate significance, one-sided exact probabilities comparing the HVR haplotype transmission with the expected 0.5 a priori probability were calculated using the cumulative binomial distribution function of MS Excel 2000.
In addition to the parent–child TDT test, sibling case–control associations were tested between the HVR haplotype and migraine or Raynaud's phenomenon using the S-TDT design (22–26). In this test the presence of the HVR haplotype is compared between sibling cases and controls from the nuclear families that make up the complete HVR pedigree. An overall statistic for the risk of carrying the HVR haplotype is subsequently calculated from the individual results of the nuclear families. From the HVR pedigree, a maximal number of nuclear families were selected in which one parent was a carrier of the HVR haplotype. From these nuclear families all the siblings were selected for the association analysis. Risk estimates and significance were calculated with the Mantel–Haenszel extension (M–H) test, using nuclear family as stratification variable (SPSS for Windows 11.5; SPSS Inc., Chicago, IL, USA) (25). Furthermore, the Z′ score approach implemented in the TDT/S-TDT 1.1 program was employed as a control statistic (24).
Results
Possible associations between Raynaud's phenomenon, migraine and the HVR haplotype were tested in the large Dutch pedigree. Parent-affected child TDT analyses were used to test for deviations of the haplotype transmission probability, which a priori is 0.5 (Table 1). For migraine 23 trios and for Raynaud's phenomenon 26 trios were analysed. Transmission probability of the HVR haplotype was only slightly increased for individuals with migraine and individuals with Raynaud's phenomenon. However, the differences from the expected transmission did not reach significance.
Transmission disequilibrium test comparing the transmission of hereditary vascular retinopathy (HVR) haplotype from a heterozygous parent to offspring with Raynaud's phenomenon or migraine

HVR T+, Transmitted HVR haplotype; HVR T–, non-transmitted HVR haplotype.
p, Transmission probability.
Next, sibling–control TDT tests were used to compare the risk of migraine and Raynaud's phenomenon in carriers and non-carriers of the HVR haplotype. In total, 71 siblings were available from 19 nuclear families in which the haplotype was segregating (Table 2). The risk of migraine was increased in HVR carriers. Of the 30 migraineurs, 13 were diagnosed with migraine without aura, three with migraine with aura, and 14 with mixed migraine with and without aura. Association analysis for the migraine subtypes separately was not meaningful due to small numbers in each group. The risk of being affected with Raynaud's phenomenon was also increased in carriers of the HVR haplotype (Table 2). Although there was a strong increase in risk in HVR haplotype carriers for having migraine and/or Raynaud's phenomenon, the frequency of both disorders was also high in non-carriers of the HVR haplotype; 11 out of 37 had migraine and 10 out of 37 had Raynaud's phenomenon. This clearly indicates that other migraine and Raynaud factors must be present in the HVR family.
Associations of Raynaud's phenomenon and migraine in relation to the presence of the hereditary vascular retinopathy (HVR) haplotype in siblings of nuclear families
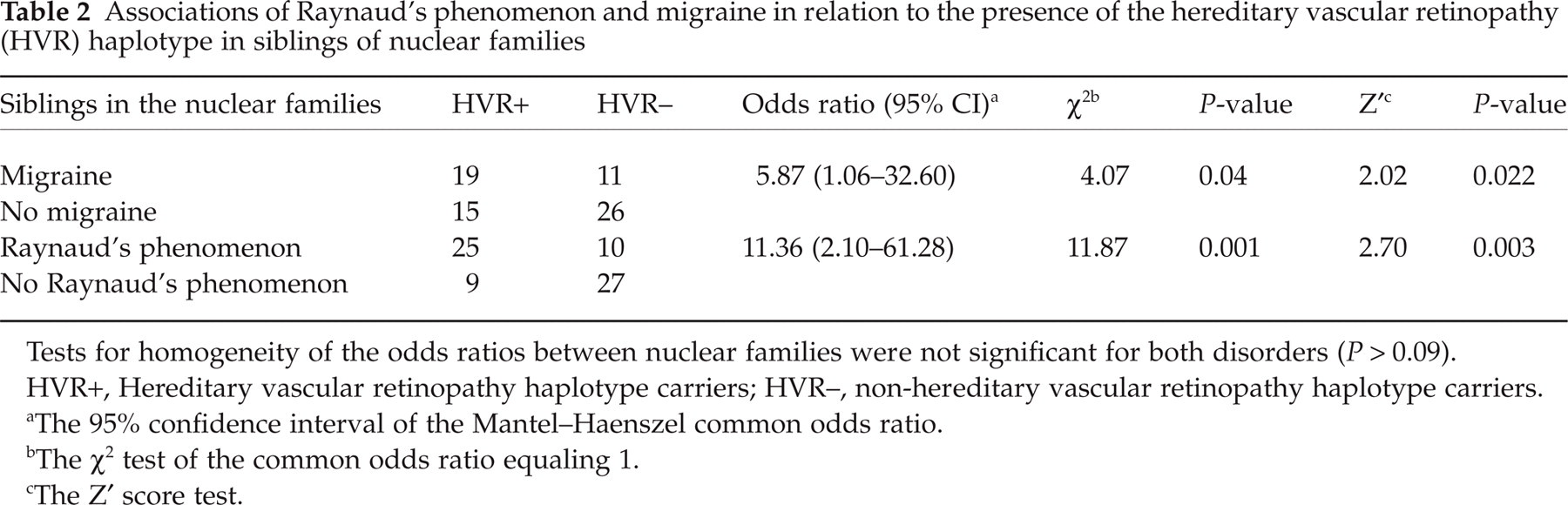
Tests for homogeneity of the odds ratios between nuclear families were not significant for both disorders (P > 0.09).
HVR+, Hereditary vascular retinopathy haplotype carriers; HVR–, non-hereditary vascular retinopathy haplotype carriers.
The 95% confidence interval of the Mantel–Haenszel common odds ratio.
The χ2 test of the common odds ratio equaling 1.
The Z′ score test.
Discussion
We tested whether the HVR haplotype, harbouring the retinopathy gene, contributed to an increased susceptibility to migraine and Raynaud's phenomenon in the Dutch family. Siblings with the HVR haplotype did show a significant increased risk of migraine and Raynaud's phenomenon compared with non-carrier siblings. We found no significant increase in transmission of the haplotype with less powerful parent-affected child TDT tests. We have provided genetic evidence that the HVR haplotype harbours a factor that increases the susceptibility to both vascular disorders in the Dutch family. However, the high incidence of these vascular diseases in non-HVR carriers suggests the presence of additional causative factors in this family.
Since retinal cerebrovascular disorders are rare, a sufficiently large sample of unrelated individuals for association analysis is difficult to obtain (8). Testing for associations between the HVR haplotype and migraine and Raynaud's phenomenon gave us a unique opportunity using a within-family approach. The fact that the rare autosomal dominant HVR haplotype is present in only one of the parents of the nuclear families allowed us to study the transmission unambiguously. Since only a single family was studied, a potential problem for testing significance is that the observations may be related (23–26). Because transmission of the HVR haplotype from parents to offspring is random (e.g. Hardy–Weinberg equilibrium), the use of the applied parent-affected child TDT tests circumvents this potential bias. Furthermore, the results of the TDT test are independent of the disorder prevalence in controls (23). Unfortunately, parent–child TDT tests lack sufficient detection power because of the low number of tested individuals. Moreover, small changes in the number of transmitted haplotypes have large effects on the significance of the outcome and we therefore tend to give less weight to these results.
For the sibling-based TDT test, taking case–control siblings from the same family provides a perfect match for confounding risk factors like population stratification, but it may increase the risk of false-positive results (32, 33). Mantel–Haenszel statistics for related samples, and the Z′ score approximation of Spielman and Ewens were used to adjust for the effects of related observations. Because the limited number of samples in each stratum may affect the P-values of the Mantel–Haenszel test, we used two tests (34).
In conclusion, we provided evidence that, within the HVR disease haplotype on chromosome 3p21.1-p21.3, a gene is present that enhances susceptibility to both Raynaud's phenomenon and migraine. Future analysis will have to show whether it is the retinopathy gene itself that is associated with migraine and Raynaud's phenomenon, or whether it a closely linked gene within the HVR haplotype.
Footnotes
Acknowledgements
We are indebted to the contribution of L.A. Sandkuijl (deceased in December 2002). We thank J. H. van Houwelingen and C. M. van Duijn for their support and comments on the manuscript. We would also like to thank the family for their cooperation. This work was supported by grants of the Netherlands Organization for Scientific Research (NWO) (903-52-291, M.D.F., R.R.F.), The Migraine Trust (R.R.F., M.D.F.), and the European Community (EC-RTN1-1999–00168, R.R.F. and A.M.J.M.v.d.M.) and the Centre for Medical Systems Biology (CMSB).