
Abstract
The objective of this study was to identify prognostic factors and assess functional status over time among patients in a headache specialty practice. Study questionnaires were mailed to 599 patients who previously presented to a headache specialty practice. Outcome measures included headache frequency, the Headache Impact Test (HIT) and the SF-36 Health Survey. Completed surveys were received from 333 respondents (56%). Thirty-five respondents (11%) had HIT scores in the ‘little or no impact’ range at follow-up and 191 (57%) had HIT scores in the ‘severe impact’ range. A diagnosis of migraine at baseline was an independent predictor of elevated HIT scores at follow-up, but gender, age, age at headache onset, daily headache at baseline, and time to follow-up did not predict poor prognosis. A subset of headache patients continue to experience marked disability and impaired functional status, months to years after presenting for headache specialty care. A diagnosis of migraine at the time of presentation may predict prognosis, but additional cohort studies with careful attention to baseline variables are needed to help identify other prognostic factors.
Introduction
Little is known about the prognosis of patients with headache in clinical practice. This is partly due to a paucity of published longitudinal cohort studies. Despite important limitations due to lack of controls and idiosyncrasies of individual physicians and their patient populations, longitudinal cohort studies of patients from a given clinical practice can: (i) help inform physicians and patients about what to expect over time from treatment; (ii) identify clinical characteristics that predict such outcomes as treatment failure, impaired functional status, patient satisfaction, or high medical-care utilization; and (iii) identify selected subsets of patients for further study.
The objectives of this longitudinal cohort study were to: (i) estimate the frequency and intensity of headaches among patients months to years after having first presented to the practice; (ii) assess headache-related disability and functional status of the patients over time; and (iii) identify clinical characteristics measurable at the time of the initial evaluation that predict prognosis.
Methods
Study population
The study population consisted of all patients who first presented to the headache specialty practice of one of the authors (E.L.H.S.) between 1 January 1996 and 31 October 2001. This physician is a board-certified neurologist with specialty training in headache management with over 20 years of practice experience. Patients in this practice are typically referred by healthcare provider. The vast majority of patients have medical insurance.
Data collection
Patients underwent a semistructured interview and a physical and neurological examination as part of their routine care during their first visit to the headache practice. The results of the clinical evaluation were summarized and typed according to the standard ‘history and physical’ format. Information documented in the clinical evaluation included: the patient's gender; age at time of presentation to the practice; approximate age of first headache onset; frequency of headaches; the presence of associated symptoms, such as nausea, vomiting, photophobia, and phonophobia; the preliminary headache diagnosis (pending further diagnostic studies, if applicable), and the therapeutic interventions recommended.
Baseline measures
The first author abstracted the following information from each patient's medical record and entered each data item into a research database: gender; date of patient's first visit to the practice, age at time of the first visit; frequency of headaches in the past month; approximate age at first headache onset; and headache diagnosis. When information was missing, ambiguous, or conflicting, the data were analysed as missing. A judgement was made in each case, however, regarding whether the patient was experiencing daily vs. episodic headaches in the month prior to the initial visit. Patients were considered to have chronic daily headache if they reported experiencing headaches ‘daily’ or ‘nearly daily’, if they reported experiencing headaches ≥ 4 days per week, or if they reported ≥ 15 days with headache in the past month. When the information about headache frequency in the past was missing or ambiguous, patients were assumed not to have chronic daily headache. Patients were considered to have both migraine and chronic daily headache if both diagnoses were applicable.
Follow-up packet
The study design and instruments were approved by the New England Institutional Review Board. A study packet was mailed to all eligible patients. The packet included a cover letter that briefly described the study, a consent form, the study questionnaire, a self-addressed, postage-paid return envelope, and a prepaid, telephone calling card with a retail value of £2.66 ($5.00). The cover letter included a description of the study, the statement that participation was voluntary, and the assurance that individual responses would not be revealed to the treating physician. Patients were asked to complete and return the consent form and all of the study instruments if they agreed to participate. Patients who chose to decline participation were asked to indicate that choice by selecting the item, ‘I do not wish to participate in this study’, on the consent form. The postage-paid envelopes were addressed to the first author, who was not involved in the medical care of any of the patients. Eligible patients were invited to use the prepaid, telephone calling card irrespective of their decision to participate. Study packets were mailed to all eligible subjects in March 2002, using mailing addresses from the headache practice's records. Second and third mailings were directed to non-responders in April and May 2002, respectively.
Outcome measures
Headache frequency and intensity were assessed at follow-up with the following questions (answer choices, when provided, are reported in parentheses):
Do you still suffer from severe headaches? (yes or no).
When was the last time you had a severe headache? (right now, within the past 7 days, within the past month, within the past 3 months, within the past year, or more than a year ago).
On how many days in the past month did you have a headache?
On a scale from 0 to 10, on average, how painful were these headaches? (0 = no pain at all, and 10 = pain as bad as it can be).
On how many days in the past 3 months did you have a headache?
Headache-specific disability was assessed with the Headache Impact Test (HIT; version 2) (1). The HIT is a standardized, six-item questionnaire designed to assess headache burden in the previous month from the patient's perspective (1). Six questions comprise the HIT: (i) When you have headaches, how often is the pain severe? (ii) How often do headaches limit your ability to do usual activities, including household work, work, school, or social activities? (iii) When you have a headache, how often do you wish you could lie down? (iv) In the past 4 weeks, how often have you felt too tired to do work or daily activities because of your headaches? (v) In the past 4 weeks, how often have you felt fed up or irritated because of your headaches? (vi) In the past 4 weeks, how often did headaches limit your ability to concentrate on work or daily activities? Response options for each item are ‘never’, ‘rarely’, ‘sometimes’, ‘often’, and ‘always.’ Point values assigned to these responses are 6, 8, 10, 11, and 13, respectively, with a HIT total score range of 36–78. A HIT score of ≤ 49 is considered to reflect ‘little or no impact’ on headache-related quality of life, a score from 50–55 ‘some impact’, a score from 56–59 ‘substantial impact’, and a score of ≥ 60 ‘severe impact’ (1). The within-person minimum important difference of the HIT among patients with chronic daily headache is approximately four units (2).
Functional status was assessed with the Medical Outcomes Study Short Form 36 (SF-36; version 2) (3). The SF-36 is a widely used, health-related quality of life instrument that assesses eight different health domains: physical functioning; bodily pain; role limitations due to physical problems; role limitations due to emotional problems; general mental health; social functioning; vitality; and general health perceptions (4).
Patients were considered to have chronic daily headache at follow-up if they reported experiencing headaches ‘daily’ or ‘nearly daily’, if they reported experiencing headaches ≥ 4 days per week, or if they reported ≥ 15 days with headache in the past month, according to the criteria for chronic daily headache proposed by others (5).
Statistical analysis
Data were entered by a research assistant and analysed using the statistical software program, Stata, Version 7 (College Station, TX, USA). A t-test for independent samples was used to assess differences in baseline variables between two groups and χ2 analysis was used for categorical variables. All significance tests were two-sided, using an α of 0.05. General linear regression using the Stata binreg function was used to calculate the relative risks of having a HIT score in the ‘little or no impact’ and the ‘severe impact’ range for selected baseline measures. The binreg function calculates the relative risk (as opposed to the odds ratio) of a dichotomous outcome.
Handling of missing data
A research assistant contacted the patients by telephone to complete the follow-up questionnaire whenever an incomplete questionnaire was received. Consequently, the final dataset included very few missing data. Missing data values were analysed as missing (i.e. estimated values for missing data were not imputed).
Results
Six hundred and six new patients presented to the headache practice between 1 January 1996 and 31 October 2001. Six patients were excluded because their addresses were outside of the USA (thereby making it difficult to provide postage-paid return envelopes), and one patient presented for a reason other than headache. The 599 remaining patients were mailed a follow-up questionnaire. Of these, 333 (56%) returned a completed questionnaire. Two hundred and sixty-six patients (44%) either did not receive the study packet or chose not to participate in the study. Time from baseline to follow-up ranged from 6 months to 6.3 years, with a mean and median of 47 and 41 months, respectively.
Baseline data from all eligible patients, respondents who completed the follow-up questionnaire, and patients lost to follow-up (non-respondents) are reported in Table 1. Among eligible patients, 469 (78%) were females, the mean age at presentation was 39 years, 378 (63%) had chronic daily headache and 514 (86%) had migraine headaches at the time that they first presented to the headache practice. The migraine headaches either occurred by themselves or were part of the chronic daily headache presentation. Respondents did not differ significantly from non-respondents by gender, age of headache onset, or prevalence of daily headache and migraine. The age at time of presentation to the headache practice was, however, higher among respondents compared with non-respondents (41 vs. 37 years; P < 0.001). The difference in age between respondents and non-respondents may be due to the fact that eligible patients who were adolescents or young adults at baseline are more likely to have changed addresses during the follow-up period, thereby making it less likely that they received the study packets. This explanation is supported by the finding that 15% of respondents (n = 49) and 22% of non-respondents (n = 57) were younger than 25 years at the time of their baseline evaluation (P = 0.03).
Baseline characteristics of all eligible subjects, respondents, and non-respondents

Estimated using the χ2 test, comparing study respondents with non-respondents.
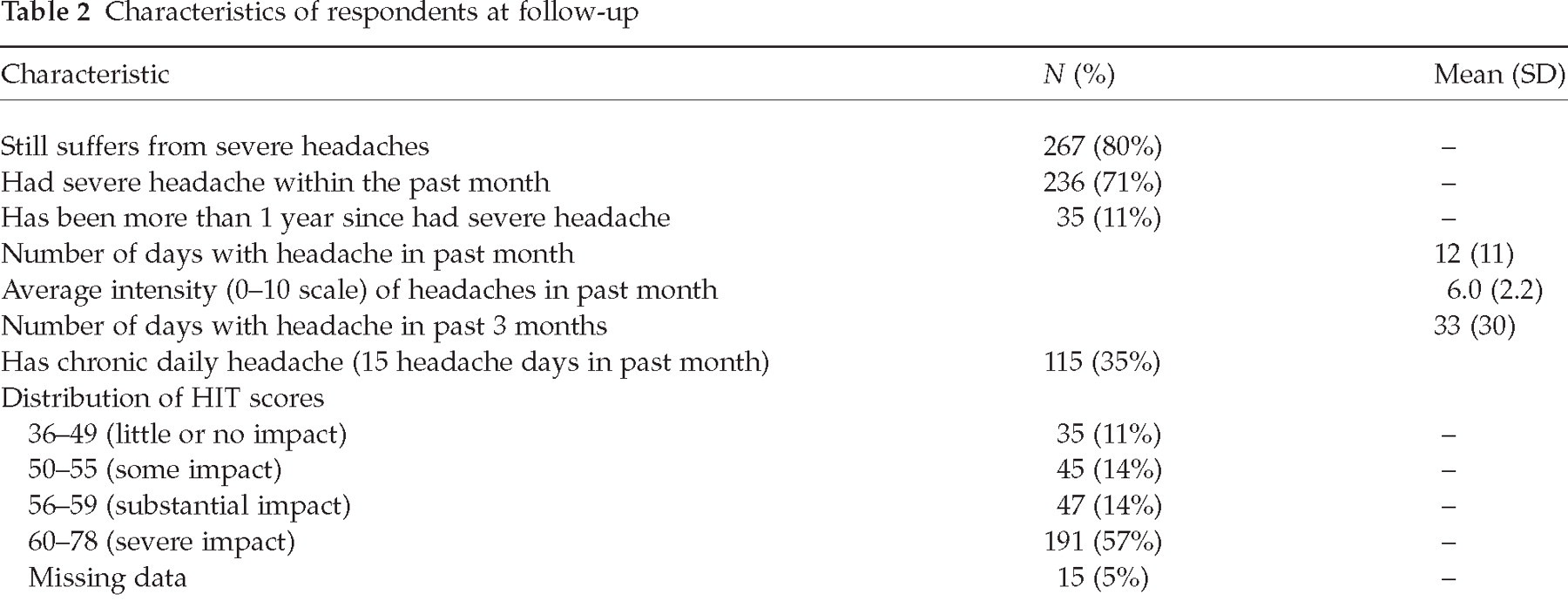
The clinical characteristics of the respondents at follow-up are reported in Table 2. Two hundred and sixty-nine respondents (80%) reported that they still suffered from severe headaches, and 237 (71%) reported having at least one headache within the past month, with a mean number of headaches in the past month of 12 and a mean intensity score of 6.0 on a scale from zero to 10. One hundred and fifteen (35%) respondents met criteria for chronic daily headache at follow-up. The mean HIT score at follow-up in our study sample was 60 (SD = 8). The majority of patients (n = 191; 57%) scored in the ‘very severe impact’ category, 47 (14%) in the ‘substantial impact’ category, 45 (14%) in the ‘some impact’ category, and 35 (11%) in the ‘little or no impact’ category. HIT scores could not be calculated for 15 respondents (5%) because of missing data.
Characteristics of respondents at follow-up
Mean HIT and SF-36 health domain scores are reported in Table 3. SF-36 scores representative of the general US population in 1998 (4) are included for comparison. A difference of ≥ 10 points between two groups of individuals on any SF-36 health domain score is considered to be clinically significant (4). Mean health domain scores were ≥ 10 points lower (reflecting greater impairment in quality of life) than scores derived from the general adult US population for role-physical, bodily pain, social function, role-emotion, and mental health domains, with the greatest disparity (18 points) observed with social function. Somewhat surprisingly, physical function health domain scores were identical in both populations.
Mean HIT and SF-36 health domain scores: respondents vs. general US adult population

Indicates the SF-36 health domains for which respondents had scores ≤10 points lower than the mean for the general US population. Lower SF-36 scores reflect greater functional impairment.
HIT and SF-36 scores stratified by gender, age at baseline, age of headache onset, presence of chronic daily headache at baseline and at follow-up, and presence of migraine headaches at baseline are reported in Table 4. There were few significant differences in HIT or SF-36 health domain scores between females and males, respondents in various age groups at baseline, or respondents with childhood-onset vs. adult-onset of headaches. In marked contrast, there were statistically significant differences in all but one (mental health) of the SF-36 health domain scores between respondents with chronic daily headache and those with episodic headaches at either baseline or follow-up. Interestingly, there was no relationship between the presence of chronic daily headache at baseline and HIT scores at follow-up, but the presence of chronic daily headache at follow-up was associated with a 5-point increase in the HIT as well as large differences in several SF-36 health domain scores at follow-up. The same is true for respondents who had migraine headaches at baseline; the mean HIT score among this group was 61, compared with a mean score of 56 (P = 0.0003) among respondents who did not have migraine headaches at baseline.
Mean HIT and SF-36 health domain scores, stratified by subgroups

P < 0.05.
P < 0.001.
The relationship between baseline variables and headache-related disability as assessed by the HIT was further investigated using linear regression. Two outcomes were assessed: (i) HIT score ≤ 49 (i.e. in the ‘little or no impact’ range); and (ii) HIT score ≥ 60 (i.e. in the ‘severe impact’ range). Covariates included all of the baseline variables for which complete and relevant data were available. The unadjusted relative risks of HIT scores for each covariate are reported in Table 5.
Relative risk (RR) of HIT scores in the ‘no impact’ and ‘severe impact’ ranges for selected baseline measures

Referent: HIT scores > 49.
Referent: HIT scores < 60.
Predictors of favourable prognosis, as assessed by low HIT scores, included both male gender [relative risk (RR) associated with female gender = 0.51, 95% confidence interval (CI) 0.27, 0.97] and the absence of migraine headaches at baseline (RR associated with the presence of migraine headaches = 0.45, 95% CI 0.31, 0.66). Age at presentation, headache onset in adulthood, chronic daily headache at baseline, and time to follow-up were not associated with low HIT scores. When gender, migraine headaches, age, and time to follow-up were included in the regression model as covariates, the relative risks associated with migraine headaches (RR = 0.54; 95% CI 0.26, 1.10) and gender (RR = 0.60; 95% CI 0.31, 1.19) remained low, but the 95% confidence interval for both includes 1.0. This can be explained, in part, by the fact that adding covariates to a regression model results in loss of precision, as demonstrated by a wider confidence interval. It is also likely, however, that the relationship between migraine headaches and HIT scores is confounded by gender. A higher proportion of female respondents had migraine headaches (n = 232, 91%) than did male respondents (n = 54, 69%; P < 0.001).
The presence of migraine headaches at baseline was associated with a relative risk of 1.64 (95% CI 1.12, 2.41) of having a HIT score in the ‘severe impact’ range, but gender, age, age at headache onset, and daily headache at baseline did not predict poor prognosis. The relative risk associated with migraine headaches was essentially unchanged after controlling for gender, age, and time elapsed between baseline and follow-up assessments (RR = 1.62; 95% CI 1.10, 2.41).
Discussion
To our knowledge, this represents the largest cohort reported to date of consecutive patients who have accessed headache specialty care. The findings suggest that while many patients with headache experience clinical improvement over time, a substantial proportion of patients with access to headache specialty care continue to experience frequent headaches and experience continued disability and impaired health-related quality of life. The findings corroborate previously published reports of marked impairment in health-related quality of life among patients with frequent headache (6–8), as well as reports of a high prevalence of chronic daily headache among patients seeking headache specialty care (9, 10).
The longitudinal nature of this study makes it possible to identify clinical characteristics that may help physicians and researchers identify, early on, which patients are likely to experience clinical improvement and which are at high risk for significant impairment in functional status despite usual medical care. The presence of migraine headaches emerged as the single independent predictor of prognosis. Non-migraineurs were twice as likely to demonstrate little or no impact from their headaches at follow-up compared with migraineurs. Conversely, patients with migraine headaches were more likely than non-migraine headache sufferers to demonstrate severe disability from headaches months to years after first being seen by a headache specialist, even after adjusting for gender and other covariates. Surprisingly, the presence of chronic daily headache at baseline does not appear to be associated with headache-related disability over time; patients with chronic daily headache at baseline were not more likely to demonstrate severe headache-related disability at follow-up, and those without chronic daily headache at baseline were not more likely to have lower HIT scores at follow-up. The presence of chronic daily headache at follow-up, however, was strongly associated with marked headache-related disability and impaired health-related quality of life at follow-up. There appears to be a relationship between gender and clinical prognosis, but this relationship is confounded by the gender differential in the baseline presence of migraine headaches.
Our findings are consistent with those of a recently published, prospective study that demonstrated significant improvement in migraine-related disability among 84 patients who received treatment for chronic migraine with medication overuse (11). In our study, neither the HIT nor the SF-36 were administered at baseline; consequently, we do not know if these patients experienced similar improvements in functional status or migraine-related disability. Our data demonstrate that most patients reported fewer headaches at follow-up compared with baseline, which suggests that as a group these patients demonstrated clinical improvement over time after having received headache specialty medical care. Our findings clearly demonstrate that a subset of patients remain impaired after treatment; our findings also suggest, but do not prove, that there may be prognostic factors measurable at baseline that can help predict which patients are at particularly high risk of not responding well to medical treatment.
Limitations of the study include the fact that only 56% of eligible patients responded to the follow-up questionnaire. Relatively low follow-up rates raise the possibility that respondents and non-respondents represent two different samples of the study population. However, we have the benefit of having baseline data on all eligible subjects, and the only difference found between respondents and non-respondents was age at presentation. Since age was not associated with HIT scores and respondents did not differ from non-respondents by other baseline measures, it is reasonable to assume that the data obtained from the respondents can be generalized to the study population as a whole.
This study is further limited by the fact that our data were obtained from a single headache practice. It is possible that the study physician or his patients are idiosyncratic in respect to other headache specialists or headache patient populations. However, there is no compelling reason to suspect that the population studied is markedly different from other headache practices, and the treating physician is a board-certified neurologist with headache-specialty training whose clinical practice is consistent with the standard of care. The fact that each subject was systematically and thoroughly evaluated by a single, highly experienced neurologist can be considered a strength of the study. The systematic way in which the baseline data were collected in the study eliminates many of the significant biases present in studies that report clinical data collected by multiple physicians.
We had few baseline variables that could be included in our linear regression models. We wish to encourage other investigators to conduct similar longitudinal studies that include standardized assessment tools, such as the HIT and SF-36, as both baseline and follow-up measures for all subjects. Such studies would further elucidate the natural history of severe headache and may help physicians identify, early on, which of their patients with headache may ultimately not respond adequately to usual medical care. Knowing how to identify such at-risk patients may help physicians decide which patients might benefit from more frequent follow-up, or from alternative or supplementary therapeutic interventions.
Footnotes
Acknowledgements
This research was funded by an investigator-initiated grant by GlaxoSmithKline.