
Abstract
The aim of this study was to evaluate the intra- and inter-examiner reliability and validity of neck range of motion (ROM) measurements. Thirty-five healthy subjects were assessed in all neck movements from two initial positions, sitting and standing, actively (open and closed eyes) and passively by using a 3D ultrasound-based motion analysis device (Zebris). Three tests were employed to assess intra-examiner reliability and two examiners used for the inter-examiner reliability. X-rays in neck flexion and extension were used to validate the Zebris system. The standing position yielded higher intraclass correlation coefficient (ICC) values (>0.86) with less error [smallest detectable difference (SDD) < 13.8%] than sitting (ICC > 0.79, SDD < 14%). Passive assessment of neck ROM presented better reproducibility than active assessment with open or closed eyes in both positions. The inter-examiner reliability was moderate (ICC = 0.43-0.68). The correlation between the Zebris system and X-rays was high in both flexion and extension movements. The results showed that the most reliable protocol for assessment of neck ROM is a passive measurement in the standing position. The measurements were well validiated against X-rays and the experience of the investigators must be considered before any comparison among studies is employed.
Introduction
Cervical range of motion (ROM) is a part of the dynamic component of spine evaluation and can be used as an indication of dysfunction in anatomical structures (1, 2) as well as a diagnostic aid in patients with neck pain (3–5) and headache (6–8). Many systematic reviews on neck pain and headache have demonstrated that cervical ROM is the most frequently reported outcome measure (9–11). However, three recent (critical or systematic) reviews on studies concerning the reliability and validity of neck mobility have demonstrated that most of the instruments and procedures utilized are seriously flawed (12–14).
A number of non-invasive instruments with varying degrees of accuracy and repeatability have been utilized to measure cervical ROM. These range from functional radiographs to the use of several types of goniometers, tape measures, visual estimation, ultrasonography-based systems, optoelectronic systems and computer interfaced video imaging. Most of these instruments, although cheap and easily applicable in a clinical setting, are limited as they cannot build composite pictures of combined planes of motion that also take into account velocity of movement (15, 16). Also, many of them are subject to bias from extraneous motion introduced from the thoracic spine and the palpation of anatomical landmarks for instrument application introduces an inherent source of experimenter bias (8, 17).
The development of computerized motion analysis devices has the advantages of monitoring relative changes in curvature of the spine during movement as well as limiting researcher bias, since the results are displayed graphically and in tabulated forms on screen. The new instruments are also capable of simultaneously recording coupled motions with the primary movement in real-time recordings (3, 15, 18, 19). Recently, devices employing electromagnetic (20–22) and optoelectronic (23–26) technology have allowed a complete investigation of head and neck movements and have reported moderate to high reliability values. Specifically, optoelectronic systems provide insights into the individuals’ movement patterns, can be used in biomechanical models and computerized simulations of movement with reference systems internal to the subject and also can be used for post hoc kinematic analysis. These instruments employ active or passive retro-reflective markers detected by several TV cameras and can separate the head–neck movements from the rest of the spine by using mathematical calculations (24, 26). However, despite the fact that they are valuable for accurate kinematic investigation and normative ROM values, their clinical usefulness in every day practice is limited (25), as they require complicated measurement procedures and analyses and the cost seems to be unaffordable for most clinicians (14).
Two of the instruments which have been used over the last 10 years and overcome many of the limitations mentioned above are the CA6000 Spine Motion Analyser, a device that registers motions using high-precision potentiometers, and the Zebris CMS (ultrasonography) system. Inter-examiner and intra-examiner reliability using these instruments has been evaluated in numerous studies (in both patients and healthy subjects, actively or passively), giving very high estimates (3, 19, 27–30). The criterion validity of the CA6000 has been evaluated in comparison with the Zebris CMS system and the correlation was very high (19). A limitation of the CA6000, however, is that the instrument binds on itself during FL/EXT measurements, especially in subjects with a short neck. The Zebris system therefore appears to be the best device available to measure cervical ROM.
If this device is to be adopted as the instrument of choice in further studies, standardized protocols for its use need to be developed. At present a great variety of methodologies exists that makes the comparison between studies almost impossible. Jordan (13), in his systematic review, noted that ‘the reliability of a tool can only be inferred for the protocol used. Unless a standard protocol for measurement and for movement is accepted and uniformly used, the need to detail these protocols in individual studies will continue’.
The only study which has attempted to compare different testing protocols was conducted by Dvir et al. (39). However, even this study was limited as it did not consider the effects of testing positions, stabilization of the torso, open and closed eyes and active or passive movement.
The aim of this study was, therefore, to develop the most valid and reliable protocol for measuring neck ROM using the Zebris system and taking into account: measurement of neck ROM in all primary directions with subjects stabilized in a neutral position, the effect of initial body position (namely sitting vs. standing), the effect of active or passive movements and the effect of the number of sessions of measurement.
Methods
Subjects
Thirty-five healthy subjects were recruited from the staff of a local physiotherapy department. Sex, age and anthropometric characteristics (height, weight) were recorded (Table 1). The selection criteria for the sample were ability to give informed consent and aged 19–63 years with the same ratio between males and females. Subjects had to be healthy without a history of neck pain, headache, injury or operation in the cervical spine as determined by a self-completed questionnaire. All subjects gave full informed consent prior to participation in the study.
Anthropometric characteristics of subjects for intra- and inter-examiner reliability and validity neck range of motion studies

SD, Standard deviation.
Apparatus
Neck ROM was measured with the Zebris CMS20 ultrasound-based motion analysis system (Zebris Meditechnic GmbH, Isny, Germany). When connected to the subject, it allows unrestricted three-dimensional motion of the head in relation to the thorax. Specially designed headgear (adjustable to adapt to individual head sizes) on which is attached a series of three miniature ultrasound transmitters is fixed to the subject's head. A thoracic harness comprising a plastic shoulder cap and a series of three transmitters serve as a reference and isolate the cervical spine movements from the rest of the spine (Fig. 1). Measurement is based on determination of the spatial coordinates of the miniature ultrasound transmitters positioned relative to a fixed system of three microphones positioned on a stand close by (Fig. 1). Using triangulation, the measurement is derived from the time delay between the ultrasound pulses measured at a sampling rate of 20 Hz. The spatial position of the head is calculated by the system's dedicated software and graphically displayed in real time (19, 31–33).

Zebris CMS20 motion analysis system for measuring neck range of motion. The headgear and the shoulder cap with a series of three transmitters (black arrows) and the stand with the three microphones.
A custom-made stabilization system was built to provide fixation of the subjects in a neutral position (both sitting and standing) and to isolate the cervical spine from the rest of the body. This system consisted of a thoracic and a lumbar component and a seat. Both stabilization components were connected to the subjects via concave plastic-coated, padded wood blocks and fastened with adjustable strap belts. The lumbar component moved in vertical and horizontal planes and was fastened with screws and pegs to fix the position at the level of the lower back. The thoracic component moved vertically only and was set in position with two screws at the level of the chest of each subject. The seat was located on a sliding frame and was also adjustable in both planes (34, 35).
Intra-examiner reliability of different testing protocols
Subjects were examined from two initial randomly selected positions: sitting and standing. All six primary movements (flexion, extension, right and left rotation, right and left side flexion) were examined in the same order dictated by the system's software routine. In both positions the above-described custom-made fixation system provided appropriate stabilization of the subjects’ trunk. In all movements subjects faced away from the apparatus. Before starting the experiments each subject performed three repetitions of the movement in each direction as a warm-up (15, 36). Active (with open and closed eyes) and passive examination of neck ROM was employed in all subjects after demonstration, practice and, if necessary, correction by the examiner. The order of active or passive assessment as well as the assessment with open or closed eyes was randomized. In passive movements the examiner was unable to see the computer screen. Care was taken during flexion and extension movements in order to ensure that both the upper and lower cervical spine contributed to the movements. This was done by demonstrating the movement and by asking the subjects to move their chin towards their chest for flexion and looking at the ceiling for extension.
Each movement was started in the neutral (reference) position, which was ensured by having a target in front of the subjects and asking them to gaze at it. Three separate repetitions in both directions were asked from the subjects at normal, preferred speed (3, 15, 32, 37, 38). Reciprocal movements were measured simultaneously. This means that a single measurement would consist, for example, of flexion, return to the initial position, 1–2-s pause, extension, return to initial position and pause for another 1–2 s (32, 39). Acquisition was stopped when the subjects had reached their neutral position.
For each direction the mean of three repetitions of each prime movement was recorded (3, 15, 19, 37). The time needed to record and save the data (5–10 s) from the previous movement was employed as the rest time before examination of a different plane of motion (15, 27, 32). Each subject was examined by the same examiner on three occasions with 1 week between each of them. Tests were performed at the same time of day to minimize any effect of diurnal variation. In addition, all measurements were carried out at least 2 h after getting up in the morning, to overcome the initial stiffness of the spine (40). In standing, all subjects were tested barefoot in order to avoid any change in normal spine curvature. A full report of possible factors that could influence the ROM was obtained from the participants before each measurement. For female participants all measurements fell within one full menstrual cycle. The instrument was zeroed for each trial immediately before the beginning of each of the tasks.
Inter-examiner studies
Ten of the 35 subjects were examined by a second independent investigator on the same day to evaluate the inter-examiner reliability of the measurements. The examiners performed a pilot study to ensure adequate training in utilizing the Zebris CMS20 system. The evaluations on each subject were performed from the more reliable passive standing position (see Results) and one after the other in random order. An interval of 15 min was allowed between the two assessors. All investigators had to reposition the device on the subject and they were blind to the results obtained from the previous examiner.
Validity study
A criterion validity study took place comparing the Zebris CMS20 with functional X-rays during flexion and extension of the cervical spine. All measurements were done from the more reliable standing position (see Results) in 10 subjects. A total of three radiographs per subject were performed: one exposure each for the neutral, flexion and extension positions. Three full ROM movements were employed as a warm-up before measurements. A radiograph was then taken in the neutral position and in full flexion and extension with simultaneous recording by the Zebris system. Two independent radiologists undertook the calculation of the ROM obtained by the radiographs. A method suggested by previous investigators was employed for these calculations (41).
Data analysis
The measuring system generates an evaluation in which the curves depicting the motion sequence are recorded for each of the movements performed in real time. The average angular values for each primary motion were read off the screen, using cursors provided by the dedicated software of the system. These values were recorded manually. The calculated angular degrees of each plane of motion (sagittal plane for flexion/extension; coronal or frontal plane for lateral flexion; and transverse plane for rotation) were added for statistical evaluation, i.e. the total range of each plane of motion was used for the analysis (31).
The ROM measurements on the radiographs were performed in three steps: tracing the lines of reference, measuring the angles between these lines of reference, and calculating the range of motion performed with the appropriate formula (41). For all subjects, each radiologist traced the following reference lines on the radiographs taken in neutral position, in flexion and extension.
Statistical analysis
ROM values were transferred to the SPSS statistical program (Version 10.1; SPSS Inc., Chicago, IL, USA) for subsequent analysis. All data was normally distributed (Kolmogorov–Smirnov test) and thus parametric tests were employed for analysing the results.
The intraclass correlation coefficient (ICC1,1), the standard error of measurement (SEM) and the smallest detectable difference (SDD) reliability indices were used in both the intra- and inter-examiner reliability studies for all parameters being tested (namely sitting and standing positions, active and passive movements, open and closed eyes).
A paired samples t-test was employed to compare mean ROM between positions, active and passive movements as well as open vs. closed eyes. The same test was used for identifying significant differences regarding ROM means between the two examiners for the inter-examiner reliability study and also differences between values obtained from the X-rays and Zebris system for the validity study.
In order to examine the level of agreement between the two examiners in inter-examiner reliability study the method recommended by Bland and Altman (42) was used. The agreement between the two measurements is given by the mean and SD of the differences. A non-zero value suggests a systematic error or bias, and negative values indicate lower values for the second examiner. The same technique was used for demonstrating differences between the two radiologists and between the two instruments (Zebris and X-rays) in the validity study. Statistical significance was accepted at the 5% level.
Results
The anthropometric characteristics of the subjects assessed in the intra- and inter-examiner and validity study are displayed in Table 1.
Intra-examiner studies
All reliability indices for the intraexaminer studies are shown in Table 2. The ICCs between all trials and movements for both positions ranged between 0.73 and 0.90 for active movements with open eyes, between 0.75 and 0.92 for active movements with closed eyes and between 0.83 and 0.97 for data obtained from passive assessment. Regarding positions, the standing position generally yielded higher ICC values than sitting. When the results obtained in the first trial were excluded, the ICCs exhibited higher values in most cases.
Reliability values for intraexaminer range of motion (ROM) data (all subjects)

ICC, Intraclass correlation coefficient; SEM, standard error of measurement; SDD, smallest detectable difference (expressed as percentage of grand mean).
Significant difference between tests.
The passive assessment of neck ROM yielded the least SEM with the lowest SDD in both positions (SEM = 4.7°−7.8° and 2.9°−7.2°; SDD = 8.1–13.4% and 5.4–13.4% for sitting and standing, respectively) than the active movements (with open or closed eyes) in most movements. Regarding the movements, side flexion presented the highest error in any assessment as indicated by the SDD estimates (>12% in any case), whereas the movements in other planes presented a mixed picture. Significant statistical differences between trials were obvious in most movements in active assessment and also in rotation in passive assessment, indicating a training and/or learning effect among trials (Table 2).
When comparing the mean ROM values (second & third trials) between the sitting and standing positions for merged data (Table 3), paired samples t-test revealed significant differences in all passive movements and also in flexion/extension and rotation when subjects were assessed actively with open eyes. In each case, the sitting position yielded greater ROM values than standing (except for side flexion in active movements with open and closed eyes). Despite the significant differences between positions, however, their greatest mean difference was only 4.7° in rotation during passive assessment. No significant differences were found between positions when subjects were assessed actively with closed eyes.
Comparison between positions regarding the mean range of motion (ROM) values for all subjects (second and third tests)
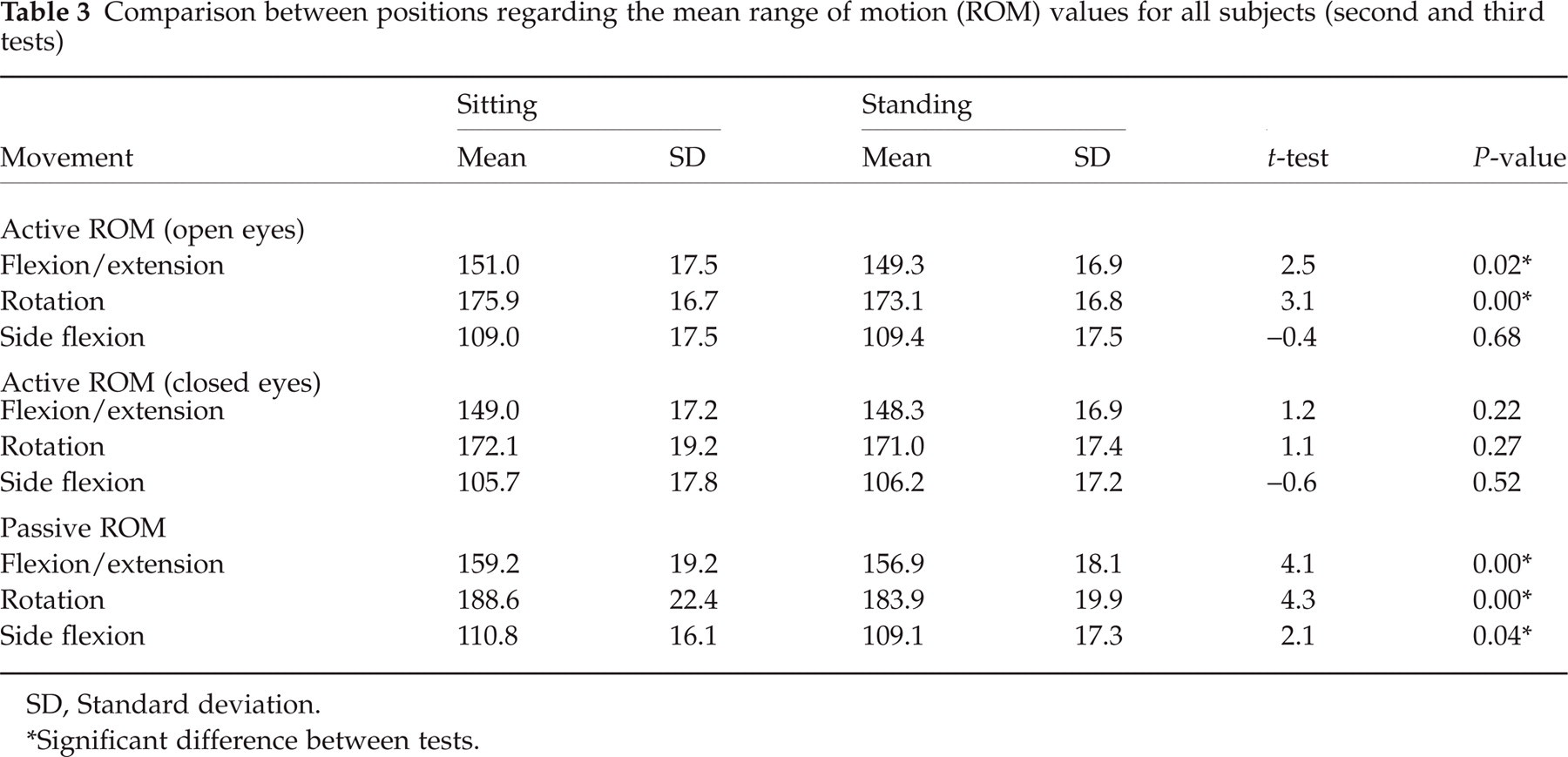
SD, Standard deviation.
Significant difference between tests.
Tables 3 and 4 show that passive assessment of neck ROM yielded significantly greater mean values than active assessment (with open or closed eyes) in all movements and positions except in side flexion with open eyes. Significant differences were also found between protocols with open and closed eyes in both positions with the exception of flexion/extension in standing (Table 4). Assessment of neck ROM with closed eyes yielded smaller mean values than open eyes. Furthermore, ROM in the transverse plane (rotation) was greater than the sagittal (flexion/extension) or coronal (side flexion) planes with side flexion presenting the lowest mobility in both positions with either passive or active ROM evaluation.
Comparison between protocols regarding the mean range of motion values for all subjects (second and third tests)

SD, Standard deviation.
Significant difference.
As far as gender differences were concerned, independent t-test showed that females had significantly greater ROM in the cervical spine than males for most movements in both positions either with active or passive evaluations.
Inter-examiner studies
All reliability indices for the interexaminer studies are summarized in Table 5. The ICCs between the two examiners were moderate(0.43–0.68) for all three planes of movement. The SEM ranged from 4.8° to 6.8° whereas the SDD was found to be between 9.8 and 13.6%. The paired t-test revealed that the differences between the two examiners were significant in all movements (P < 0.01), with the second examiner always yielding lower ROM values than the first examiner.
Inter-examiner reliability and range of motion values (passive movements)
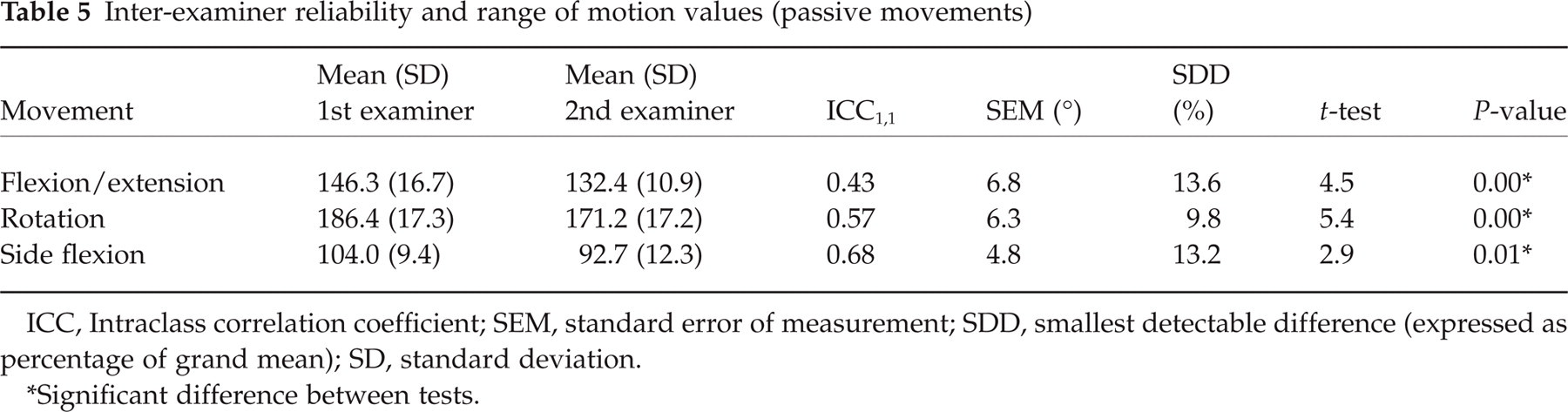
ICC, Intraclass correlation coefficient; SEM, standard error of measurement; SDD, smallest detectable difference (expressed as percentage of grand mean); SD, standard deviation.
Significant difference between tests.
The levels of agreement plots for each movement are displayed in Fig. 2 (dashed lines are confidence intervals). The reference lines in all plots are negative and away from zero, indicating the systematic error between the examiners. However, any difference between the examiners was not related to the magnitude of the measured ROM.

Discrepancies between trials in the inter-examiner study assessed by Bland and Altman technique presenting the amount of agreement of the means of two trials against the difference between the trials in (a) flexion/extension; (b) rotation; and (c) side flexion.
Validity study
High ICCs (>0.85) with no statistically significant differences were found between the two radiologists in calculating the ROM in neck flexion and extension from the X-rays. Table 6 shows the correlations and the paired t-test between X-rays (mean of the two radiologists) and Zebris readings regarding neck flexion and extension. The ICCs were excellent (>0.88) and although there was a significant difference between the two measurement tools in flexion, this difference was only 3.5° (Table 6). In both flexion and extension movements the X-rays yielded lower ROM values than the Zebris system. Figure 3 represents graphically the discrepancies between the Zebris and X-rays and indicates a small systematic error between them (the mean difference is negative in both movements).

Discrepancies between measurement tools in the validity study assessed by Bland and Altman technique presenting the amount of agreement of the means of two measurements against the difference between the measurements in (a) flexion, (b) extension.
Reliability values and paired t-test between X-rays (mean of two radiologists) and Zebris system
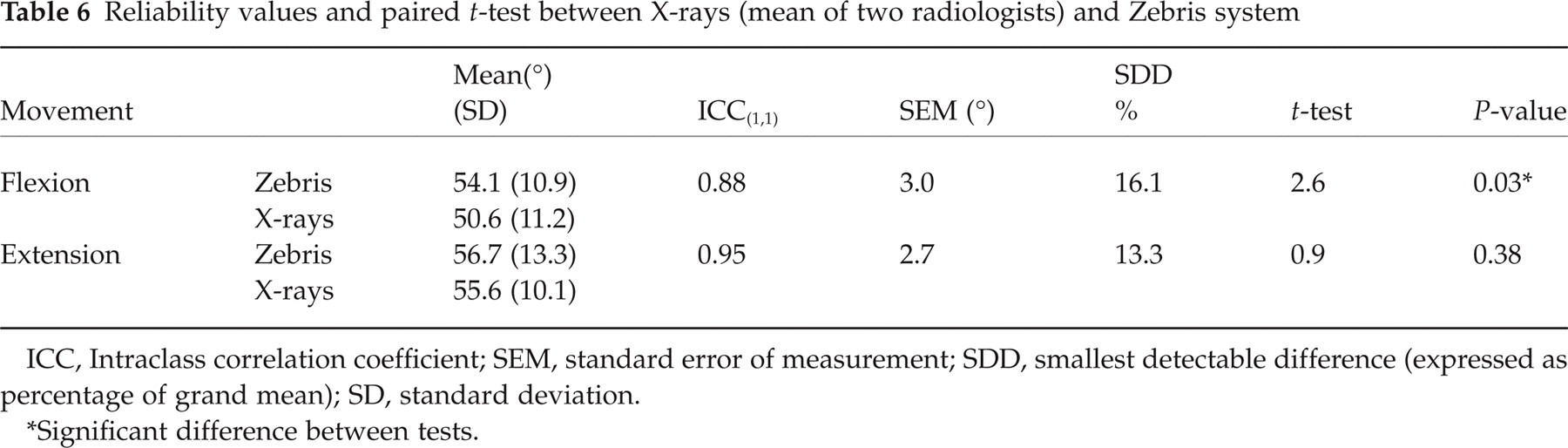
ICC, Intraclass correlation coefficient; SEM, standard error of measurement; SDD, smallest detectable difference (expressed as percentage of grand mean); SD, standard deviation.
Significant difference between tests.
Discussion
A considerable number of reliability and validity studies examining cervical mobility have been identified in the literature and from this point of view the present study cannot claim novelty. This is, however, the first study to examine in detail the optimum testing protocol by employing the same sample to compare neck ROM from two different initial body positions (namely, sitting and standing) and examining the participants’ ROM actively with open and closed eyes as well as passively. Furthermore, no other study was identified in the literature that validated the neck ROM against radiographs with the Zebris motion analysis system.
Intra-examiner reliability study
All three ROM protocols (namely, active with open eyes, active with closed eyes and passive) examined in the present intra-examiner study yielded high ICC values (>0.79 in all assessments for the second and third trials). The most reliable protocol was passive assessment of neck ROM from a standing position. The greatest within-session error was 14% in side flexion with closed eyes (Table 2).
The SEM as a reliability index was used in only a few previous studies employing the same (39) or different instruments in sitting position (29, 43, 44) and was similar or even greater than the present results. No other study used the SDD clinical applicability index in order to compare the current findings, but this index can be calculated if the SEM and the mean of the measurements are known (SDD = 1.96 √2 × SEM). Thus, making these calculations, the SDD values obtained from the present experiments (<14% in any test) are comparable to some previous reports and in most cases are considerably lower (SDD ranged between 6.4% and 55.2% in previous studies) (a table with previous studies is available on request by the authors). These results indicate acceptable clinical applicability of each protocol for most movements.
Only full cycle ROMs were calculated and analysed in this study because an extensive literature review demonstrated that assessment of movement over the whole plane yields higher reliability than when separated into its component parts (15, 27, 32, 45–47). The main reason for this trend is the inability of the subjects to assume reliably the same neutral head position relative to the thorax in measuring half-cycle ROM. This fact is a serious limitation for clinical application of ROM assessment (decreases sensitivity and raises difficulties in distinguishing the affected side) and more efforts have to be made to overcome this shortcoming.
Initial body position effect
The new stabilization system designed and developed by the authors in combination with the Zebris motion analysis system permits the assessment of neck ROM from two initial positions (i.e. sitting and standing) while subjects are secured in neutral position with wide velcro belts. This system overcomes many of the limitations of other instruments and protocols identified in the literature. Results of the recent experiments showed that both initial positions yielded high reliability estimates with standing being slightly better in most movements (Table 2). The only other study comparing neck ROM between sitting and standing positions was conducted by Lantz et al. (48), who utilized the CA6000 SMA without any stabilization of the trunk, but the authors did not assess the reliability for each position in order to compare them. They reported only that the sitting position yielded consistently significantly (P < 0.03) higher active ROM values than standing position regardless of the plane of motion (mean difference 2.6°). These results are in accordance with the results of the current study except in lateral flexion, where both positions yielded similar values (Table 3).
Lantz and colleagues (48) explained these systematic differences between positions probably as the result of the leverage of the hands when they placed them on the knees in sitting. In the present experiments, however, all participants had their hands hanging by their sides in both positions and the above differences still existed, so this explanation seems inadequate. A more probable cause for these discrepancies could be the change of the normal spine curvatures when different initial positions are utilized, resulting in different ROM values.
Active vs. passive neck ROM
As mentioned in Results, passive assessment of cervical ROM was shown to be more reliable than active assessment in both sitting and standing positions. These differences were more obvious when the participants were examined actively with the eyes open (Table 2). Similar results were also reported by other authors utilizing the same or other instruments (e.g. CA6000 SMA) in sitting (3, 31), although there is no consensus in the literature regarding which protocol (active or passive) is best, with some studies demonstrating the active assessment being more reliable (48), and others showing no differences between the protocols (8, 21).
Passive examination of neck ROM resulted in significantly larger motions (P < 0.05) in comparison with active assessment in all movements except in lateral flexion with open eyes (Table 4). These differences are comparable to those reported by previous investigators (3, 27) and have to be considered when different studies and protocols are compared. However, provided that both active and passive protocols proved quite reliable, as in the present study, and having definite advantages over each other in certain situations (e.g. the passive ROM assessment provides information for the passive structures of the spine whereas the active assessment offers information for coupled movements and muscles), clinicians or researchers choose either protocol according to their aim.
Open vs. closed eyes
The influence of vision on reliability of cervical ROM has not been examined by any study previously. Although neck mobility with closed eyes has been investigated to a lesser extent than with open eyes, the results showed better reliability with less within-session error when the vision is eliminated in standing position (Table 2). The opposite happened, however, when the participants were examined in the sitting position. The suggestion therefore that the use of vision can give better reproducibility regarding the ROM estimates (39) cannot be supported by the present results.
Regarding the mean ROM values, the protocol with open eyes yielded significantly higher values (P < 0.01) than with closed eyes in all movements and positions except the flexion/extension in standing (P = 0.10). The greatest mean difference, however, was only 3.8°. Despite the above inconsistencies in results, no protocol seems to be significantly superior over the other, suggesting that both can be used in clinical research.
Mean neck ROM values and direction effect
The mean ROM values obtained from the present experiments could be compared only with studies utilizing similar instruments and protocols. In general, the present values were higher than previous reports using another type of the Zebris system from a sitting position and without stabilization of the trunk (19, 39). The only study which yielded similar results with the current values in both active and passive measurements was conducted by Castro et al. (31), who measured their subjects in sitting position with also a lack of any stabilization procedure. Even in this study, however, the mean estimates in lateral flexion were considerable lower than in the present study (91.9° and 109.0°, respectively) and the authors did not conduct any study to validate their results. No adequate explanations could be found for these discrepancies among similar studies employing similar devices (except the differences in trunk stabilization), as the sample size characteristics were not very different. This fact highlights the concerns regarding the comparison between different investigations as well as the published normative data and cut-off points between healthy subjects and patients.
The differences among the planes of motion are in agreement with all previous reports in spite of the technologies or protocols utilized. Neck mobility was greatest in the transverse plane followed by the sagittal plane, whereas the coronal plane movements presented the smallest ROM. The reliability values, however, were better in the sagittal plane than in the other two planes (Table 2), being in agreement with some previous reports (8, 15, 22, 27). In contrast, other authors found the flexion and extension movements to be the least reliable (32, 43).
In all protocols (active with open and closed eyes and passive) lateral flexion yielded the highest within-session error with lowest correlation coefficients in both positions. One explanation for this trend may be the stabilization system which is efficient enough for stabilizing the trunk in the sagittal plane but not in the coronal plane. Furthermore, the shoulder cap of the Zebris system, which serves as a reference in order to isolate movements of the cervical spine from the rest of the body, is always located on the right shoulder and seems to be inadequate for preventing shoulder elevation, especially from the left side. As a result, the system may record larger lateral flexion mobility than what actually exists and may generate greater variability in test–retest assessments. Stabilization straps fixing both shoulders may prevent additional movements from the spine and shoulders, permitting more reliable and valid results.
Inter-examiner reliability study
The results showed poor to moderate reliability for the inter-examiner study (ICC = 0.43–0.68), whereas the between-measurements error was similar to the intra-examiner study (SDD = 9.8–13.6%). The Bland and Altman analysis showed that there was a systematic bias among tests, with one examiner yielding significantly lower neck ROM values in all assessments than the other (P < 0.01). These results were in contrast to previous reports (22, 27, 48), which published very high inter-examiner reliability values, although none of them used the same instrument, protocol or stabilization procedure as the present study.
An explanation for the current findings may be the fact that the second examiner, although an experienced research physiotherapist, had no experience of passively measuring neck ROM and therefore could have been more protective (yielding lower ROM values) with the subjects than the first examiner (who had previously conducted all measurements in the intra-examiner study). The relatively small SEM and SDD values give confidence that with more training the differences between examiners would be smaller. This issue has also been highlighted previously in a systematic review which noticed that examiner training may be a factor in reliability, particularly for examiner-assisted procedures such as passive ROM (12). The use of experienced manual therapists in ROM measurements, at least in research environment, would probably resolve this shortcoming.
Validity study
Although radiographic measures of range of motion are commonly considered the gold standard, concerns have been raised regarding their reliability. The main problem is the identification of specific landmarks on the X-rays in order to draw the reference lines for further calculations. In the present study two radiologists made the reference lines and calculations independently, and the results showed no statistically significant difference between them. Furthermore, the ICCs between the two radiologists were very high (0.87 and 0.85 for flexion and extension, respectively) and the Bland and Altman levels of agreement did not show any systematic error or bias.
Comparisons between the ranges of motion measured using the two devices in the present study yielded acceptable concordant results for both flexion and extension, with the latter demonstrating the best correlation between methods. The differences in mean values for each measurement tool, although statistically significant in flexion (P = 0.03), were mostly small (<3.5°) and systematic (the X-rays in most cases yielded smaller values). These results ensure the validity of the neck ROM measurements when the Zebris device is employed.
Limitations and side-effects
The Zebris system is a very capable tool and convenient in its application to subjects. However, there are a number of limitations. Apart from the stabilization problems mentioned above and the lack of randomization due to the software routine, another serious limitation is that in very mobile subjects the contact between the transmitters and the stable microphones can be lost (especially in axial rotation and lateral flexion) and thus the user must move the stand with the microphones accordingly during the recording.
Furthermore, although the measurement of range of motion is a very easy assessment even for patients, some participants (all of them female) experienced a sensation of dizziness or inconvenience during the tests, especially in the standing position. Dvir et al. (39), using the same system, has also reported similar symptoms in the sitting position. The cause for these symptoms is not clear, but the continuous movements of the head as well as the head part of the Zebris system (which is put on the subjects’ head like spectacles) may play a role.
Conclusion
Range of motion is the most well-investigated physical parameter in the cervical spine. Despite extensive research, however, there is no universal consensus as far as the normative neck ROM values or the protocols and tools for detecting these values are concerned. The results of the current experiments show that the passive assessment of neck ROM in standing position is more reliable than the active assessment with either open or closed eyes. Furthermore, small differences between neck ROM estimates measured with the Zebris motion system and X-rays give confidence in the validity of the results. The moderate reliability between different examiners highlights, however, the need to consider the experience of the investigators before any comparison among studies is employed. Some limitations of the study, especially with the stabilization system, indicate also the use of more rigorous procedures for obtaining better results. Therefore, the present data demonstrate that the optimal measurement protocol for cervical ROM investigation requires a passive assessment by an experienced examiner from a standing position with a stabilization system to isolate the neck–head motion from the rest of the body and with the use of a measurement instrument that is precise, able to measure in all planes of motion, well-fixed on the subjects’ head and able to provide valid information for comprehensive kinematic analysis.
Footnotes
Acknowledgements
We gratefully acknowledge the help from all the volunteers.