
Abstract
This study aimed to compare (i) migraineurs' diagnosis, treatment strategies and satisfaction when treated by community care physicians (CCPs) and at the specialist headache clinic; (ii) migraineurs' knowledge of migraine treatments and outcomes at baseline and at 3 months' interval. Thirty-eight patients were interviewed at baseline visit and 3 months after neurologist consultation, using a survey form which consisted of a series of self-designed questions, the MIDAS questionnaire and the SF-36 Health Survey. More patients were informed of the diagnosis of migraine by the neurologist than by CCPs. Compared with CCPs, the neurologist was more likely to employ preventive therapies, prescribe triptans and ask patients to keep a headache diary. Patients' number of days with headaches in the last 3 months, pain intensity, MIDAS score and five out of the eight SF-36 domain scores were significantly improved at the 3 months' interval (P < 0.05) compared with baseline at the specialist headache clinic. More patients recognized migraine-specific therapies and reported satisfaction with treatment after the neurologist consultation. This is the first study detailing significant improvements in patients' clinical outcomes, knowledge of migraine treatments and satisfaction after consultation at a specialist headache clinic in Singapore.
Introduction
Migraine is a chronic heterogeneous neurovascular disorder that affects 9.3% of the Singapore population (1). In addition to severe, debilitating headache, migraineurs may experience nausea, vomiting, and sensitivity to light and sound. Migraine greatly affects the quality of life and has been ranked nineteenth above diabetes mellitus among the world's most disabling medical illness by the World Health Organization (2). In the USA, migraine's yearly cost to employers is about US$13 billion (£6.75 billion), of which only US$1 billion (£0.52 billion) accounts for direct medical costs and most is indirect medical costs such as decreased work productivity and sick leave (3). Despite this burden of illness, physicians often do not diagnose (4, 5) and treat the illness effectively (6).
The Singapore General Hospital (SGH) Headache Clinic is a specialized clinic which provides a comprehensive service for the diagnosis, evaluation and treatment of headache patients. Appointment at the clinic is strictly by referral from the other medical practitioners. To our knowledge, no studies examining the care of the patients referred to the SGH Headache Clinic for migraine treatment by the community care physicians (CCPs) has been reported to date. However, studies examining the differences in migraine care services provided by CCPs and HEADACHE SPECIALISTS in the UK (7), USA (8) and Italy (9) have been reported.
The present study was undertaken (i) to compare the differences in migraineur's diagnosis, treatment strategies and satisfaction when treated by CCPs and at SGH Headache Clinic; (ii) to assess the differences in migraineur's knowledge of migraine treatments and treatment outcomes at baseline and 3 months’ interval.
Methods
Eligibility
Patients who met all of the following criteria were considered for enrolment: (i) referred to the SGH Headache Clinic for the first time by a CCP; (ii) diagnosed of having migraine by the SGH neurologist; and (iii) possessed the ability to give informed consent. Patients with non-migraine headaches or who did not receive a confirmed diagnosis for migraine on their first visit to the SGH Headache Clinic were excluded.
Data collection
Data collection at baseline and 3 months’ interval was through the use of a survey form which comprised: (i) a series of self-designed questions querying migraineur's diagnosis, treatment strategies, knowledge of migraine treatments and satisfaction; (ii) Migraine Disability Assessment (MIDAS) questionnaire and Short Form 36 (SF-36) Health Survey for measurement of treatment outcomes. The survey form was administered by an independent interviewer through face-to-face interviews for patients who were referred to the Headache Clinic for the first time by the CCP, before consultation with the neurologist. History taking and physical examination were then conducted by the neurologist. Only patients who had been diagnosed with migraine were selected for follow-up at the 3 months’ interval and the survey was administered over the telephone by an independent interviewer.
MIDAS Questionnaire
The MIDAS questionnaire is a well-validated instrument which exhibits high internal consistency, test–retest reliability, accuracy and validity (10, 11). It measures headache-related disability by five disability questions that assess missed days from work or school, from household work, from family, social, or leisure activities and additional days with significant limitations to activity (defined as at least 50% reduced productivity) in domain of employment and household work as a result of headache. A MIDAS score is derived as a sum of the lost days recorded in the five questions. It can be higher than the actual number of lost headache days because more than one domain of activity can be affected on the same day. Although the MIDAS score is a continuous measure, it can be classified into four categories based on disability: (i) minimal disability, 0–5 points; (ii) mild disability, 6–10 points; (iii) moderate disability, 11–20 points; (iv) severe disability, 21+ points. The MIDAS questionnaire also collects information on the number of days the patient experiences a headache over the preceding 3 months as well their average pain score (on a 0–10 scale).
SF-36 Health Survey
The SF-36 Health Survey is a 36-item questionnaire that measures quality of life in eight domains of perceived health using a single multi-item scale: physical functioning (PF); role limitations due to physical problems (RP); bodily pain (BP); vitality (VT); general health perceptions (GH); social functioning (SF); role limitations due to emotional problems (RE) and mental health (MH) (12). These eight domains were grouped into two health dimension scales: physical component score (PCS) (PF, RP, BP and VT), and mental component score (MCS) (SF, GH, RE and MH). The SF-36 Health Survey was scored in accordance with published standards, with higher scores (range 0–100) reflecting better perceived health. The UK English standard version of the SF-36 Health Survey with 4-week recall and metric measurements has been validated in Singapore (13) and was used in this study.
The definitions of SF-36 scores are summarized in Table 1 (12). The PF scale measures the impact of health on limitations to any physical activity, including dressing, bathing, running or lifting heavy objects. The RP scale assesses the impact of health on work and related activities. The BP scale evaluates the severity of bodily pain in the past month and its impact on work or chores. The GH scale summarizes current health status overall. The VT scale captures general energy levels by assessing feelings of ‘pep and energy’ and of being ‘worn out and tired’. The SF scale reflects the impact of health on participation in social activities. The RE scale assesses the impact of emotional health on work and other activities. Lastly, the MH scale evaluates the frequency of feelings of nervousness, depression, happiness and calm.
Definition of SF-36 health survey scores

Statistical analysis
Continuous variables data were analysed using paired Student's t-test. P-values < 0.05 were considered to be statistically significant.
Results
Demographics
Data were collected for 38 patients. Baseline demographic characteristics of the patients are summarized in Table 2. The majority of the patients were women (74%) and Chinese (73%). The most common concurrent medical condition reported by the patients was hypertension (18%).
Baseline demographic characteristics of the patients

Diagnosis
As shown in Fig. 1, 100% and 32% of the patients were informed of the diagnosis of migraine by the SGH neurologist and CCP, respectively. Sixty-three per cent of the patients reported that their CCP did not inform them of the types of headache from which they were suffering. The differences in the patients’ perceptions of their headache causes at baseline and 3 months’ interval are summarized in Fig. 2. Most of the patients at baseline (50%) and 3 months’ interval (68%) were not aware of their headaches’ precipitating factors.

Types of headache described to the patients by the community care physicians (□) and Singapore General Hospital Headache Clinic (▪).

Comparison of patients’ perceptions of the precipitating factors of headache at baseline (□) and 3 months (▪).
Treatment strategies
The differences in treatment strategies employed by the SGH neurologist and CCP are shown in Fig. 3. Patients reported that they received both abortive and preventive therapies from the SGH neurologist (82%) and CCP (8%). Eighty-seven per cent of the patients were prescribed only abortive therapy by the CCP compared with only 8% of the patients seen at the SGH Headache Clinic. The most commonly used abortive therapy by the SGH neurologist was triptans, while CCP used simple analgesics (acetaminophen/acetaminophen combination products) most frequently (Fig. 4). As shown in Fig. 5, tricyclic antidepressants, anticonvulsants and riboflavin were among the most widely used preventive therapies by the SGH neurologist, while the most commonly used preventive therapy by the CCP was tricyclic antidepressants. Thirty-four per cent and 18% of the patients reported the use of alternative therapies after consulting the CCP and SGH neurologist, respectively. Five per cent of the patients reported that they informed the CCP of the use of alternative therapies, while only 11% of patients informed the SGH neurologist. It is shown in Fig. 6 that the most widely used alternative therapy was traditional medicine (31%) at baseline and acupuncture (11%) at the 3 months’ interval.

Comparison of the treatment strategies used by the community care physicians (□) and Singapore General Hospital Headache Clinic (▪).

Comparison of the types of abortive medications used by the community care physicians (□) and Singapore General Hospital Headache Clinic (▪).

Comparison of the types of preventive medications used by the community care physicians (□) and Singapore General Hospital Headache Clinic (▪).

Comparison of the types of alternative therapies used at baseline (□) and 3 months (▪).
Treatment outcomes
The differences in treatment outcomes are summarized in Fig. 7. The MIDAS score, number of days with headaches in the last 3 months, pain intensity and PF, RP, BP, VT, SF, PCS and MCS SF-36 Health Survey scores were significantly improved at 3 months’ interval when compared with baseline (P < 0.05). There was a reduction in the number of days with headaches in the last 3 months (61%), pain score (22%) and MIDAS score (87%) at 3 months’ interval when compared with baseline. An improvement in PF (8%), RP (90%), BP (39%), VT (14%), SF (35%), PCS (15%) and MCS (7%) SF-36 Health Survey scores was observed at 3 months’ interval when compared with baseline. Sixteen per cent of the patients visited other physicians for headache treatment after referral at the SGH neurologist. The main reason for visiting other physicians was that they were still having headaches.

Comparison of patient outcomes. Results are expressed as meands ± SEM. ∗P < 0.05 (paired t-test). □, Baseline; ▪, 3 months. (a) Midas score. (b) Number of days with headache within the last 3 months. (c) Average pain score of headache within the last 3 months. (d) SF-36 quality of life scores at baseline and 3 months at Specialist Headache Clinic. PF, Physical functioning; RP, role limitations due to physical problems; BP, bodily pain; GH, general health perceptions; VT, vitality; SF, social functioning; RE, role limitations due to emotional problems; MH, mental health; PCS, physical component score; MCS, mental component score.
Knowledge of migraine treatments
The differences in migraineurs’ knowledge of migraine treatments are summarized in Fig. 8. There was an increase of 53% and 79% in patients who recognized and knew how to use migraine-specific abortive and preventive therapies, respectively, after referral at the SGH Headache Clinic. Compared with baseline, there was an increase of 68% and 3% in patients who had heard of triptans and ergots derivatives, respectively, at 3 months’ interval. At baseline, 60% of the patients who had heard of ergot derivatives knew that they are migraine specific compared with 100% of the patients at 3 months’ interval. At baseline, 50% of the patients who had heard of ergot derivatives still continued to use ergot derivatives, while only 33% of the patients continued to use them at the 3 months’ interval. After referral at the SGH Headache Clinic, 85% of patients who had heard of triptans knew that they are migraine-specific agents. Of those who had heard of triptans at the 3 months’ interval, 59% still continued to use triptans, while 22% discontinue their use and 19% of them did not start the use of triptans even when information had been provided. The reasons for discontinuing the use of triptans are summarized in Fig. 9. At the 3 months’ interval, the main reason for not starting the use of triptans when they had been heard of is that the headaches could be treated with other medications. The main reasons for discontinuing the use of triptans at the 3 months’ interval were that the triptans were too expensive and not effective.
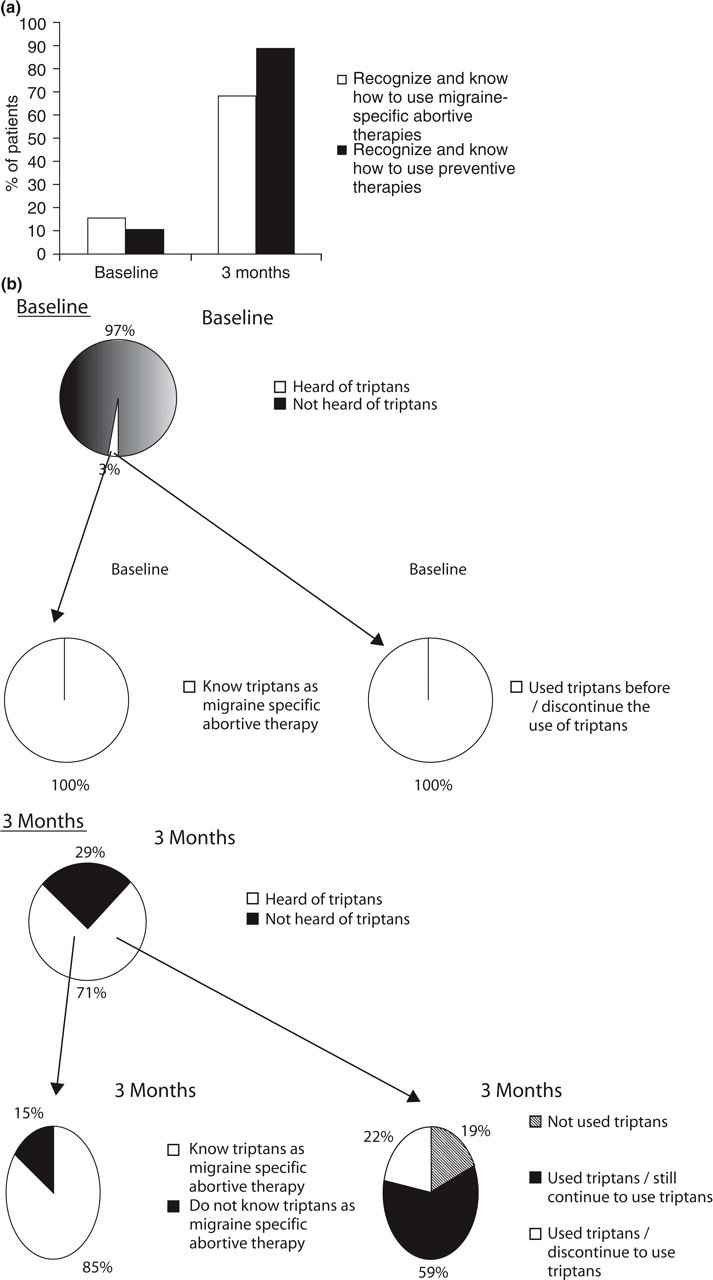
Comparison of patients’ knowledge and usage of (a) abortive (migraine specific) and preventive therapies, (b) triptans at baseline and 3 months, and (c) ergot derivatives at baseline and 3 months.

Reasons for discontinuing the use of triptans. □, Baseline; ▪, 3 months.
Satisfaction
The differences in migraineurs’ satisfaction with CCP and SGH migraine care services are summarized in Fig. 10. Compared with CCP, 18% more of the patients were satisfied with the SGH Headache Clinic's waiting time, 8% more were satisfied with consultation time, 13% more were satisfied with explanation about the condition, and 26% more were satisfied with treatment. The main reason for dissatisfaction of treatment provided by the CCP and SGH neurologist was that the headaches still persisted (Fig. 11).

Comparison of percentage of patients who are satisfied with the care services received from the community care physician (□) and Singapore General Hospital Headache Clinic (▪).

Reasons for dissatisfaction with treatment received from the community care physician (□) and Singapore General Hospital Headache Clinic (▪).
Discussion
Diagnosis
In 2000, the Ministry of Health (MOH) in Singapore published a clinical practice guideline on the diagnosis and management of headache (14). The guideline recommends that physicians should always make an accurate diagnosis of the type of headache and its cause. The guideline also recommends the physicians to use the International Headache Society diagnostic criteria for headache disorders (15) to aid in their diagnosis. Interestingly 63% of the patients reported that their CCP did not inform them of the types of headache from which they were suffering. This result indicates two possibilities. First, some of the CCPs were not familiar with the diagnosis of various types of headaches, probably due to inadequate training on headache management provided during their medical school and internship. Second, there could be a lack of effort or time for some of the CCPs to communicate clearly to their patients regarding their headache conditions.
Most of the migraineurs were not aware of any precipitating factors associated with their migraines at baseline and at the 3 months’ interval. Some of the possible reasons for this observation may be that these patients did not have any triggers, failed to take note of triggers or neglected to note these down. Some of these failures may be due to inadequate patient education by the attending physician (16). Physicians should encourage migraineurs actively to identify precipitating factors for headache so that the patients know which behaviours or foods should be avoided in managing their headaches.
Treatment strategies
The American Academy of Neurology (AAN) has published evidence-based guidelines for the diagnosis and management of migraine headaches (17). It recommends that the intensity of care should be linked with the level of disability and symptoms such as nausea and vomiting (stratified care) for the acute treatment of symptoms of an ongoing attack. Preventive treatment should be considered for patients whose migraine has a substantial impact on their lives and who have not responded to acute care, or where the frequency of migraine attacks is such that the reliance on acute care medications would increase the potential of rebound headache. The Singapore MOH guidelines recommend preventive therapies for patients with headaches occurring more than four times a month. The AAN guidelines recommend migraine-specific agents (triptans and ergot derivatives) and non-steroidal anti-inflammatory drugs or combination analgesics containing caffeine to be used as first-line agent for moderate–severe migraines and mild–moderate migraines, respectively. Acetaminophen alone is not recommended for migraine treatment. However, the Singapore MOH guideline has classified acetaminophen alone as a medication with Level I/II evidence for efficacy in the acute treatment of migraine. The AAN guidelines reported that amitriptylline, sodium valporate and propranolol have the highest level evidence-based efficacy. Riboflavin has been reported to have moderate level evidence-based efficacy in the AAN guidelines.
Despite the recommendations of the above-mentioned guidelines, it is surprisingly to observe a low usage of migraine-specific abortive and preventive therapies by the CCP on the same group of patients when compared with the SGH Headache Clinic. There are several possible explanations. First, the patients’ conditions might not have been severe enough to warrant the use of triptans and ergot derivatives and preventive therapies when seen by the CCP. Second, the CCP may have difficulty in making an accurate diagnosis of migraine and thus increase the tendency to prescribe non-migraine-specific treatments. Third, the CCP may have different evaluation criteria for the severity of the migraine compared with the SGH neurologist.
Wide usage of triptans, tricyclic antidepressants, anticonvulsants and riboflavin by the SGH neurologist could be attributed to the recommendations of the AAN guidelines. The classification of acetaminophen alone as a medication with Level I/II evidence for efficacy in the acute treatment of migraine by Singapore MOH could have explained its frequent use by the CCP.
The reduction in the usage of alternative therapies after consultation at the SGH Headache Clinic may be for the following reasons. First, the patients’ conditions may have improved after using mainstream medications, thus decreasing the likelihood of using alternative therapies. Second, the SGH neurologist may have reinforced compliance on the patients to keep to the medications prescribed. The low rate of reporting to the physician of the use of alternative therapies by the patients is worrying. Adverse drug interactions with the alternative therapies could be a potential problem. This result indicates that the physicians have to play a more active role in querying their patients on the usage of alternative therapies. At the same time, pharmacists could also contribute to the prevention of such adverse drug interactions by spending more time querying the patients on alternative therapy usage during dispensing. Patient compliance and proper usage of abortive and preventive medications could also be reinforced by the pharmacists during dispensing.
Treatment outcomes
Quality of life and disability measurement have emerged as important complementary approaches to the evaluation of the burden of headaches (18–20). Migraineurs have been found to score significantly lower on all eight SF-36 Healthy Survey domains compared with non-migraineurs (21–23). Quality of life was reported to be inversely related to migraine attack frequency (23). Thus, improvement in the quality of life and reduction of attack frequency, severity and disability have been included as goals of migraine treatment by the AAN (17). The present study shows improvement in patients’ treatment outcomes as measured by the MIDAS questionnaire and SF-36 Health Survey after referral at the SGH Headache Clinic. This was probably due to the usage of both abortive (migraine specific) and preventive therapies. However, it should be noted that 42% of the patients were unemployed and this could affect the MIDAS scoring.
It is interesting to note that 16% of the patients visited other physicians for headache treatment after consultation at the SGH Clinic. The main reason for this was that the patients were still having headaches.
Knowledge of migraine treatments
The increase in the number of patients recognizing and knowing how to use migraine-specific abortive and preventive therapies after referral at the SGH Headache Clinic suggests that more in-depth patient education on migraine treatment was provided by the SGH neurologist than by the CCP. Also, 22% of the patients who had heard of triptans discontinued their use. The main reasons for discontinuing the use of triptans were that triptans were too expensive and not effective. These reasons are to be expected, as triptans are indeed much higher priced than other headache medications. Ferrari has reported in his meta-analysis of triptan trials that the average percentage of patients experiencing a 2-h headache response after triptan use ranged from 42% to 69% (24). Silberstein has also mentioned that the response to triptans is often idiosyncratic. One triptan might work for one patient and cause no adverse events, while a different triptan might work for another patient (25). Thus, it is to be expected that some patients may find triptans to be ineffective. Another interesting point is that 19% of the patients who had heard of triptans did not start using them, the main reason being that the headache could be treated with other medications. This may mean that these patients may be over-cautious in trying new medications and probably have doubts over the safety and efficacy of triptans.
Satisfaction
The increase in the proportion of patients satisfied with the migraine care services at the SGH Headache Clinic when compared with the CCP could be attributed to the improvement in their headache conditions and having a better understanding of their headache conditions.
Comparison with other studies
Our study shows similar results to those of other overseas studies (7–9) in that triptans and preventive therapies are more widely used by headache specialists than CCPs in migraine treatment. This indicates a possible international consensus among headache specialists with regard to migraine treatment.
Limitations
This study has several limitations. First, it does not allow an unbiased comparison of care by CCP and SGH neurologist. A study design in which patients were randomly allocated to either CCP or SGH neurologist would allow such a comparison. Second, there is an underlying sample bias, as the patients being studied had already been screened by a primary care physician. These results apply only to patients referred to the SGH Headache Clinic by CCPs. Extrapolation of these results to headache patients treated by other neurologists would not be appropriate. Third, further validation of these results is warranted due to the small sample size.
Conclusion
This is the first study detailing the significant improvement in patients’ clinical outcomes, knowledge of migraine treatments and satisfaction after referral at a Singapore Headache Clinic by the community care physicians. These improvements could be due to the usage of both abortive (migraine specific) and preventive therapies. This study also shows that there is a need for the community care physicians to provide more patient education on headache and its management.
Footnotes
Acknowledgements
The authors thank Quality Metric for authorizing royalty free use of the SF-36 Health Survey.