
Abstract
Against a background of increasing demands on limited resources, health economics is gaining an increasing impact on decision making and a basic understanding of the subject is important for all those involved in headache research and service delivery at whatever level. This paper is not intended as a review of the literature in the area of headache economics but discusses some general principles of health economics from the perspective of headache, with a focus on cost of illness studies and economic evaluation.
Introduction
Against a background of increasing demands on limited healthcare resources, health economics has become an important input into decision-making at all levels of healthcare organizations. As drugs are easier to evaluate than other healthcare interventions and because of the availability of high-quality information required for licensing, the focus has been on pharmacoeconomic analysis underpinned by the rationale that it is the value of medicines that is important and not their costs. In fact, a number of countries now require a formal economic analysis before a new drug is introduced.
This paper discusses some general principles of health economics from the perspective of headache. It is not intended as a review of the literature in the area but aims to facilitate a basic understanding of the subject for those involved in the development and delivery of headache services.
The paper is constructed in five parts. The first section gives a brief overview of the discipline of health economics. The second and third sections consider the two most relevant areas of health economics – cost of illness studies and economic evaluation. The fourth section outlines some problems in undertaking economic analysis and the final section suggests how economic studies can be used when undertaking resource decisions.
What is health economics?
Health economics is the discipline of economics applied to the topic of healthcare. Broadly defined, economics concerns how society allocates its resources among alternative uses. Scarcity of these resources provides the foundation of economic theory, and from this starting point three basic questions arise:
What goods and services shall we produce?
How shall we produce them?
Who shall receive them?
The traditional economic starting point is to assume that a market offers the most effective model to address these questions. Here, resources are allocated on the basis of price and the ability to pay. However, health economists recognize the limitations of this approach in healthcare, where there are a number of problems. For example, there is a desire for an equitable distribution of resources rather than ability to pay and there are problems with information asymmetry. Doctors have greater knowledge than patients and in market situations they may use this to their own advantage.
Health economics seeks to address these ‘market failures’ and offers an explicit decision-making model based on the underlying value of efficiency – maximizing the benefits from available healthcare resources. As healthcare budgets are finite and spending in one area is inevitably at the expense of investment in another, efficiency can be seen as ensuring benefits gained exceed benefits forgone.
The importance of the economic model is that it provides useful insights into how healthcare can be organized and financed and provides a framework to address a broad range of issues in an explicit and consistent manner. It is not the only approach to decision making. Considerations of equity, public opinion and politics are also important and often conflict with economic directives.
Health economists are interested in the production of health at a number of levels, such as the influences on the demand for healthcare, the healthcare seeking behaviour of individuals and providers and alternative ways of production and delivery of healthcare. However, from the perspective of headache, this paper explores the principles of two aspects of health economists’ work that are most relevant and that form the bulk of their work: the cost of illness or measuring its economic burden; and economic evaluation – facilitating the allocation of limited healthcare resources by comparing the costs and benefits of alternative interventions.
The economic burden of headache or cost of illness
Headache, and particularly migraine, creates a burden for patients, their families and society. Cost of illness studies aim to quantify this burden by measuring the costs of a disease in monetary terms (1). An extensive review of the economic cost of migraine can be found in Lasarus (2). Three types of costs are defined:
(i) Direct costs form the cornerstone of cost of illness studies and reflect costs incurred by the healthcare system such as drugs and hospitals. Although in the UK 75% of migraine sufferers will consult their general practitioner (GP) at some time (3), the direct costs of headache are low compared with other major disease areas. Migraine care in the UK is estimated to account for 1% of NHS costs (4) and in the USA, direct medical costs are estimated at $1billion per annum (5).
(ii) Indirect costs measure the economic burden of lost production due to morbidity or premature mortality and the main burden of migraine is in this area. There remains a lack of consensus as to the best way to measure productivity losses and whether earnings are a correct measure of productivity (6). Measuring indirect costs also discriminates against those who are not at work but whose performance may still be affected, e.g. the elderly, housewives and school children.
In the UK the overall loss of productivity due to migraine has been estimated at between £611 million and £741 million a year (4) and $13 billion in the USA in 1997 (5).
(iii) Intangible costs represent those costs of pain, suffering or reduction in quality of life. Direct and indirect costs do not capture the impact on the quality of life of the sufferers. For example, measures of health-related quality of life in migraine are similar to patients with other chronic conditions such as arthritis and diabetes (7) and worse than those with asthma (8). However, as it is difficult to allocate a monetary value to this area, intangible costs are usually ignored in economic studies.
There are a number of methodological difficulties undertaking accurate cost of illness studies as the wide range of estimates demonstrate. Due to the high resource demands of studies themselves, results must be extrapolated from small samples and often illnesses may overlap. For example, it may be difficult to identify and allocate relevant costs where patients have coexisting disease such as depression and migraine.
Some advantages and disadvantages of cost of illness studies are shown in Fig. 1.
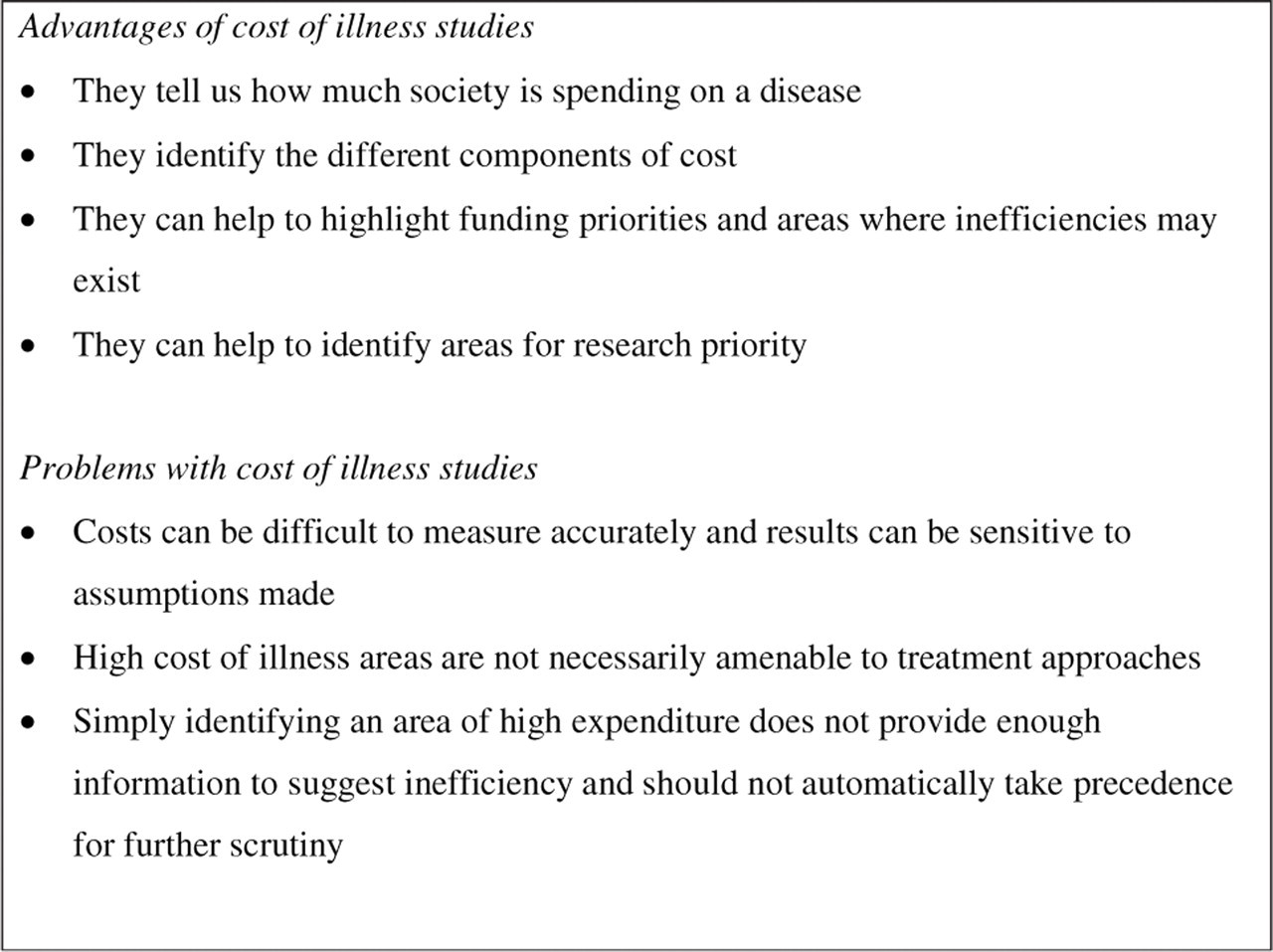
A summary of the advantages and disadvantages of cost of illness studies.
Cost of illness studies offer an alternative perspective on the importance of diseases compared with other epidemiological indicators such as morbidity and mortality and are being used increasingly by pharmaceutical companies to emphasize the importance of a product area. However, there is a danger that policy makers may be misled by this approach and its importance remains contested amongst health economists. If these studies are used to allocate resources, it does not necessarily follow that benefit will follow or that resources can be utilized efficiently.
This concern is the focus of economic evaluation, an approach that stresses the importance of measuring both costs and the benefits that investment incurs.
Economic evaluation and headache management
Not everyone can have the healthcare from which they can benefit. The concept of economic evaluation facilitates choices in healthcare from the perspective of efficiency by relating the benefits of an intervention to the resources invested in it. Efficiency means either maximizing the benefit from a fixed sum of money or minimizing the resources required for a defined benefit. Unlike cost of illness studies, which focus on costs alone, economic evaluation relates the benefits of alternative interventions to the resources incurred in their production (see Fig. 2).

An economic analysis relates inputs (resources) to outputs (benefits and the values attached to them) of alternative interventions to facilitate decision making when resources are scarce.
The type of economic evaluation is characterized by the way in which benefits are measured.
Cost minimization analysis
In cost minimization analysis, the consequences of two or more interventions being compared are equivalent. The analysis therefore focuses on costs alone. For example, if two migraine medications gave equivalent benefits, a cost minimization analysis could be relevant.
Cost–benefit analysis
Here, benefit is measured in monetary terms (9). For example, a study looking at the impact of a Triptan on work loss due to migraine found that a Triptan intervention at a cost of £3.75 saved £12 in productivity losses when compared with placebo (10).
Cost–effectiveness analysis
This is the most common type of study and measures benefits in terms of a clinical measure (11), e.g. reduction in blood pressure, reduction in pain. However, it has the disadvantage that only interventions with similar outcomes can be compared. For example, Williams (12) compared Almotriptan and Rizatriptan in terms of the proportion of patients who achieved sustained freedom with no side-effects and concluded that Almotriptan was more cost effective from this perspective.
Cost–utility analysis
A cost–utility study aims to provide a generic measure of well-being (13). Ideally, a universal measure of benefit is described that encompasses both quantity and quality of life, enabling different types of healthcare interventions to be compared. For example, should a healthcare organization divert resources into headache services or cardiac rehabilitation programmes? Or does a new migraine medication represent value for money compared with investing in new drugs in other clinical areas?
The current measure of choice is the Quality Adjusted Life Year (QALY) which allocates a value to the quality of life between 0 (worse state) and 1 (best state) and combines it with the length of time in that state to obtain the number of quality adjusted life years. For example, a Canadian study found a cost of $7500/QALY for using Triptans for migraine compared with Ergotamine (14).
Figure 3 summaries the four types of economic evaluation.
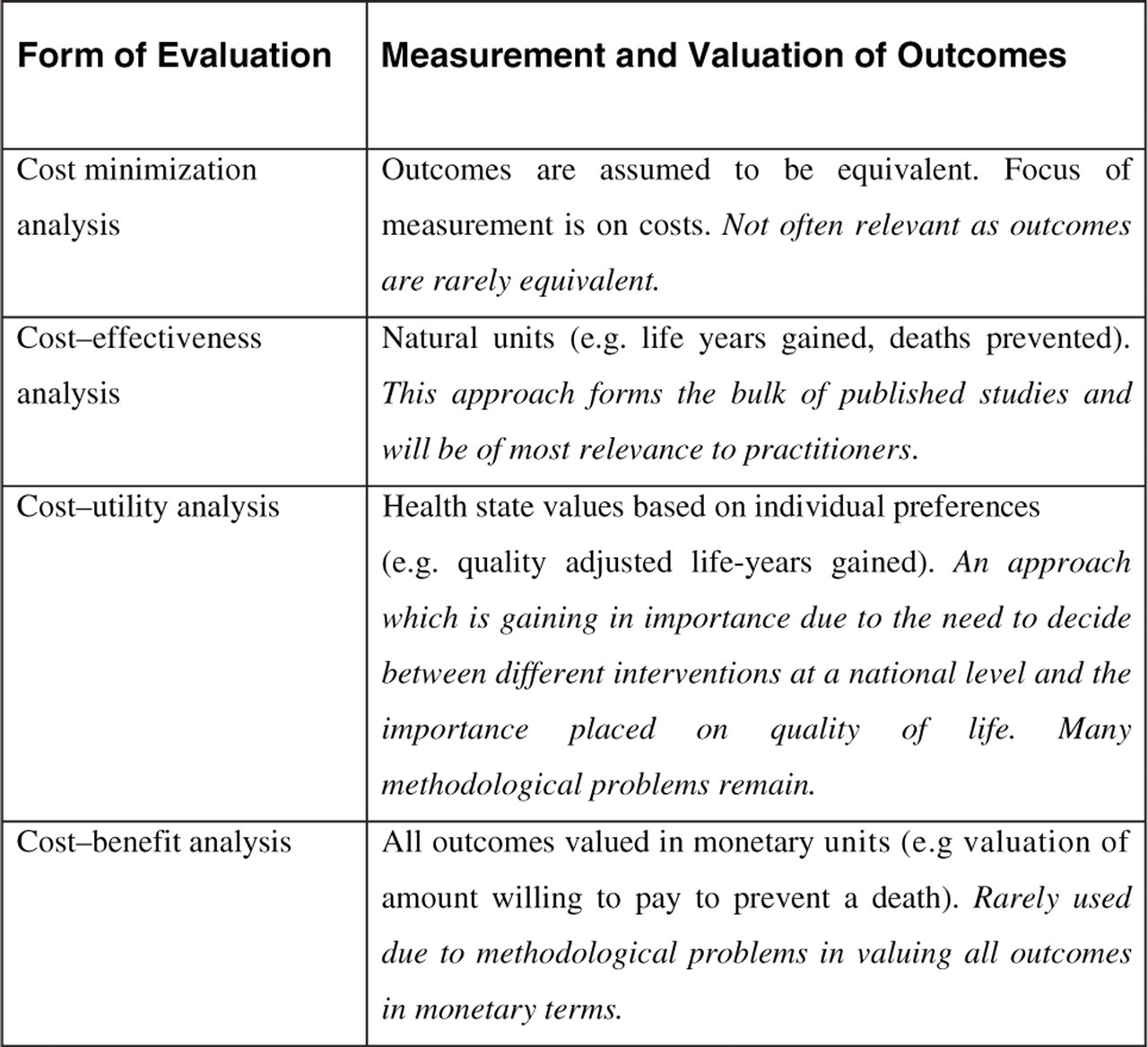
The four types of formal economic evaluation.
Cost–consequence analysis
In many cases, decisions consider multiple outcomes rather than condense benefits into a single measure. A cost–consequence analysis is not a formal method of economic analysis but has attractions for decision-makers who can apply their own weight to the various outcomes. In this approach, costs and outcomes are presented in multiple and disaggregated form, which avoids the need to represent results as a single index (15). Figure 4 shows how this approach would consider whether to expand a headache clinic service delivered in primary care.
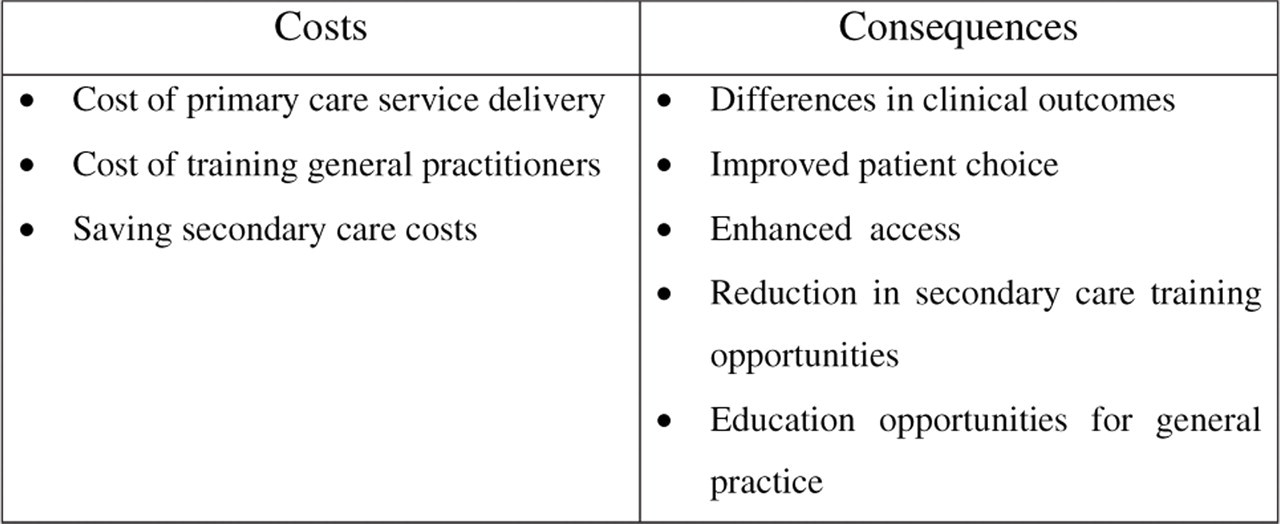
A cost–consequence analysis for transferring headache services to an intermediate primary care-based service. Decision makers apply their own values to the data.
Problems undertaking economic analysis
When undertaking a decision, it is important to be clear about the viewpoint of the evaluation. The study perspective determines which costs and in some cases which benefits to include in an evaluation (16). Different results may be obtained from the perspective of the patient, primary care, secondary care, the health system or society, and perspectives often conflict. For example, a GP who holds a prescribing budget will be less concerned about economic impact on work loss and reluctant to prescribe Triptans due to their high unit cost, despite the fact that they may allow a migraneur to remain more economically active. A different perspective can also give very different cost estimates. For example, the cost of a GP's time can range between £21/h from a practice perspective and £69/h from the perspective of the health service where all overheads including training are considered (17).
A societal economic perspective incorporates all the costs and benefits regardless of who incurs or obtains them. In practice, it is rare that a societal perspective is undertaken but more restrictive perspectives may mask the fact that costs have simply been shifted to another sector rather than being saved.
Ideally, economic analysis should be carried out alongside a clinical controlled trial, but this is not always possible or practical (18). Often, modelling studies are undertaken, drawing upon evidence where it is available and expert opinion where it is not (19). Given the problems associated with economic studies, it is important to identify assumptions and wherever possible test the sensitivity of any conclusions drawn to any assumptions made across the range of cost estimates that are found. Sensitivity analysis allows the outcome of an analysis to be tested over a range of situations likely to be found in practice to determine the robustness of analysis to potential change Key variables (20).
Finally, there can also be problems with statistical manipulation of economic data and the power requirements from an economic perspective are often different from clinical requirements (21).
Making the decision following economic analysis
With cost minimization and cost–benefit analysis, making the decision is straightforward. With cost minimization, the cheapest option is chosen and in cost benefit, if the monetary benefit outweighs the investment in resources then that option is accepted. However, with cost effectiveness and cost utility exercises there is invariably additional benefit but at extra cost, and a decision will have to be made as to whether the extra benefit is worth paying for.
One approach has suggested a threshold value for the QALY that society is willing to pay. Figure 5 shows one possible framework based on the quality of evidence on which the economic study is based, suggesting that interventions based on good evidence and costing up to £20 000 for each additional QALY are worth paying for (22). However, this approach overlooks affordability. If a new intervention delivers QALYs under the threshold there could be uncontrollable healthcare expenditure – just because an intervention is efficient it does not follow it is affordable. There is also the likelihood that manufacturers will price their products at the threshold value, again leading to budgetary pressures.

A suggested framework to decide whether an intervention should be adopted based on the strength of evidence and cost/QALY.
A further complication is that many decisions in healthcare are concerned with the expansion or contraction of interventions or services (i.e. changes at the margin). As the relationship between costs and benefits can rarely be expressed by a simple proportional relationship, health economists stress the importance of analysing changes in terms of their marginal effects (23). A marginal analysis identifies how increments in benefit change with increments in cost, as shown in Fig. 6. Note that at any point of resource investment, the marginal cost per unit of benefit differs from the average cost per unit of benefit. For example, the return on brain imaging in headache will decrease as increasing numbers of patients are targeted.
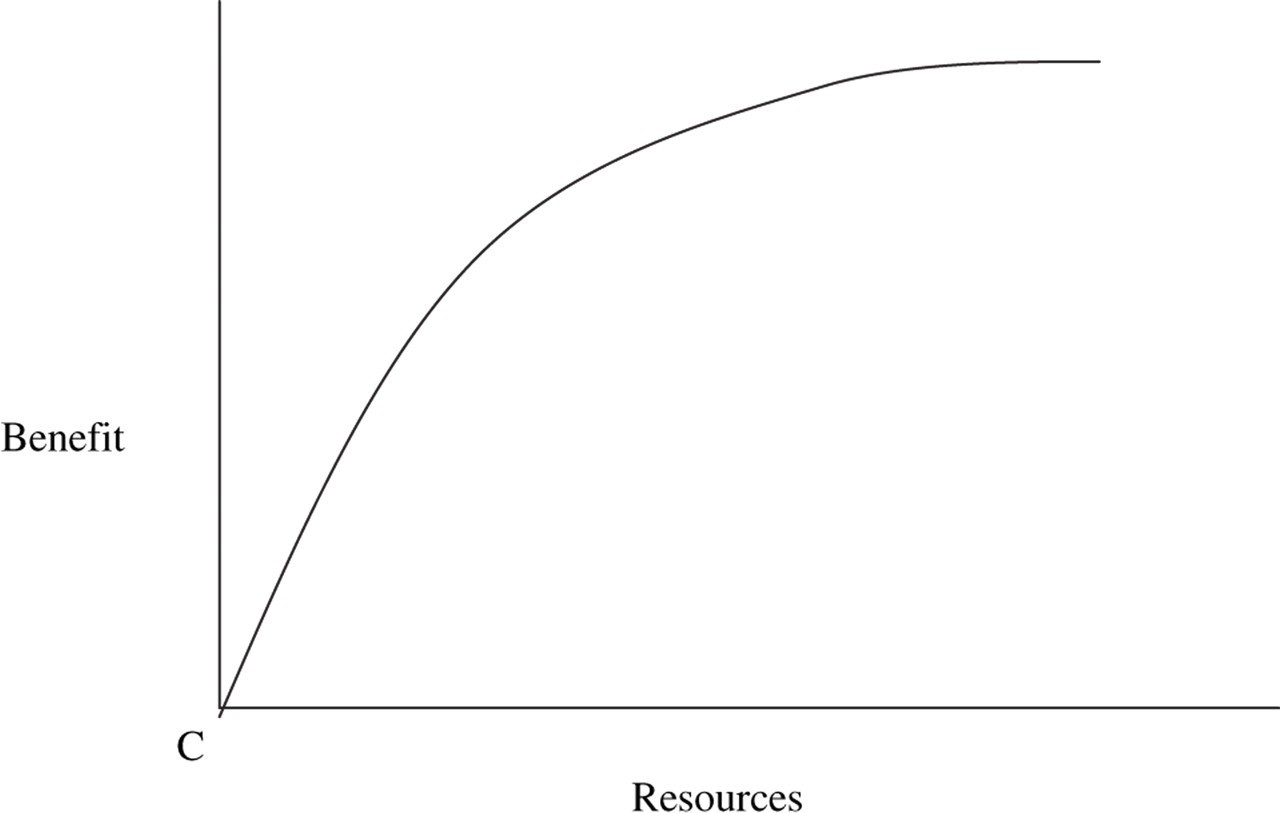
Marginal analysis and the law of diminishing marginal return. Benefits do not continue to increase in a simple proportional relationship as more resources are invested in any healthcare intervention.
Conclusion
What things cost is becoming an inevitable fact of life. However, health economists stress that costs should not stand alone but be related to the benefits that they incur. By offering a framework in which costs and benefits of competing interventions can be compared in an explicit manner, health economics can facilitate the difficult decisions that are inevitable in healthcare. However, there are relatively few economic evaluations in the field of headache and there is a general concern over publication bias (24). Many studies are promoted by the pharmaceutical industry and there is a natural tendency to publish favourable studies at the expense of those that may not show products in such a favourable light.
Just because a headache intervention is effective does not mean it offers an efficient utilization of healthcare resources. Against a background of increasing demands on limited resources, health economics is gaining an increasing impact and a basic understanding of the subject is important for all those involved in headache research and service delivery at whatever level.