
Abstract
Willingness to pay methods measure treatment preferences and also measure the burden of illness in economic terms. We used a contingent valuation method to measure migraine sufferers' willingness to pay (WTP) for acute medication for their most severe headache attacks, based on various profiles of treatment benefits and the characteristics of the migraine sufferer. Subjects were identified from a population-based database of migraine sufferers, previously recruited by random digit dialling. Telephone interviews (n = 1428) were used to gather demographic and headache characteristics. Subjects who met the International Headache Society criteria for migraine with or without aura and satisfied the other inclusion criteria based on telephone interview (n = 312) were invited to participate in a mailed questionnaire study. The questionnaire was mailed to the 310 subjects who agreed to participate and 201 (65%) surveys were returned. The survey included questions on the demographics, the migraine characteristics, and the psychological disposition of the respondents. WTP for an acute migraine treatment with 14 different hypothetical treatment profiles was explored. Responders and non-responders to the survey were generally similar. The newly designed WTP questionnaire had high internal consistency (Cronbach's α 0.90) and test-retest reliability (Spearman's corrleation coefficients 0.71-0.77). Study subjects were willing to pay a median price of 5 for a migraine treatment that provided complete relief in 30 min and worked 100% of the time, with no side-effects and no headache recurrence. Median WTP decreased as treatment attributes deviated from this ideal. For example, WTP declined to a median of 1 for complete relief in 2 h and to $0.25 for complete relief in 4 h. All of the medication attributes powerfully influenced WTP. Several variables predicted WTP including current payment for medication, MIDAS (Grade III), and those with headaches of long duration. Subjects who employed a greater number of coping skills were less willing to pay. Patient demographics and migraine severity predict WTP, but treatment attributes were also important. As treatment improves, WTP for migraine medications is likely to increase.
Introduction
The public health significance of migraine is established by the substantial impact the disorder has both on the individual and on society. While the individual impact can be measured in terms of the frequency and severity of attacks, or by using measures of quality of life, the societal impact of migraine is often measured by the economic costs associated with the condition.
Current knowledge about the economic cost of migraine is limited because most studies have estimated lost productivity by measuring the number of lost workdays and reduced effectiveness at work, associated with migraine (1–5). Many of these studies did not translate estimates of lost work time into economic terms (i.e. money). Other studies have assessed healthcare utilization, measuring the frequency of physician and emergency department visits, but did not report the costs associated with these services. Several studies have specifically estimated the economic cost of migraine in the USA (2, 5–7).
In contrast to studies that assess either the individual or societal costs of a condition, a cost of illness analysis assesses the burden of disease on the individual and society. There are two major cost of illness techniques: the human capital and the willingness to pay (WTP) methodologies (8). The human capital method estimates direct as well as indirect costs. While direct costs include money spent on healthcare utilization and medical research, indirect costs are measured in terms of the value of output lost because of reduced productivity, absenteeism or death. In addition, the friction cost method estimates indirect costs by estimating the real amount of production losses due to disease or production gains of healthcare programmes (9–11). One study using the friction cost method estimated the indirect costs associated with eight healthcare programmes (12). In this study, the indirect costs were greatest if the healthcare programme produced health benefits quickly and resulted in frequent short-term absences from work; and when a considerable portion of the affected population was employed at the moment they benefited from the programme.
The human capital method has been used in migraine research. Hu et al. (7) used population-based methods to identify migraine sufferers, and estimated that migraine costs American employers about $13 billion per year due to absenteeism and impaired work function. Annual direct medical costs for migraine medical care were approximately $1 billion per year based on data from 1994.
Although this study provided important information about the impact of migraine, the human capital method has notable weaknesses. Most importantly, it values the indirect costs of the disease according to the sufferers’ salaries (13). Thus, the impact of the disease in a labourer or homemaker is assigned a lower value than the same disease in a business executive. The WTP method, on the other hand, assesses the burden of the disease by measuring individuals’ willingness to pay for improvement in their health status (8). Thus, individuals place their own value on the pain and other intangible costs of the illness.
WTP may vary with the attributes of treatment (e.g. efficacy, side-effects, convenience) as well as the characteristics of the patient. Subject characteristics of potential import include severity and frequency of pain and associated symptoms. Of the broad range of acute treatment attributes for migraine, we focused on speed of relief, consistency of relief, side-effects, and recurrence based on prior work suggesting that these attributes were priorities for migraine sufferers (14). Examining variation in WTP for various treatment attributes can be used to rank the relative import of these attributes to patients.
Although the WTP method has been applied to a number of conditions (15–17), there is only one published WTP study in migraine (18). Using the contingent valuation method (19, 20), the study reported herein was designed to help clarify the burden of migraine by expressing the impact of illness in standard and quantifiable terms. Estimating the cost of illness is the first step in understanding the value of diagnosis and treatment. We also sought to identify the attributes of acute treatment that were the most highly valued by particular patient segments.
Methods
Data collection
Subjects were recruited from a population-based database of headache sufferers (Fig. 1) that was compiled using random digit dialing and a computer-assisted telephone interview (CATI) (21). During the initial phone contact, a household census is taken and each age-eligible household member is interviewed. After verbal informed consent is obtained, subjects are asked whether they have had at least one headache not due to a head injury, hangover, pregnancy, or an illness such as a cold or flu in their lifetime. Next, the subjects describe each of their headache types, in their own words. The remainder of the interview focuses on the two most severe types of headaches that occurred in the last year. After gathering detailed information about the headache characteristics, diagnoses are assigned to each headache type described by the subject. Diagnoses are assigned based on International Headache Society (IHS) criteria for migraine with or without aura. The sensitivity and specificity of the telephone interview for migraine with or without aura is 85% and 96%, respectively (21).

Disposition of subjects screened for enrolment in the study.
From this database, a total of 1428 previously identified headache sufferers were targetted as potential subjects. All resided in the Baltimore, Maryland area. Subjects were eligible to participate if they met IHS criteria for migraine with or without aura, were between 18 and 65 years of age, experienced their first migraine before age 50, and suffered from at least six migraine attacks (with or without aura) per year. Of the 1428 potential subjects, 312 (21.8%) were recontacted by telephone and met the inclusion criteria. Summaries of participation and eligibility dispositions are presented in Fig. 1.
In the next phase of the study, the migraine sufferers were asked to complete a mailed questionnaire that collected data pertaining to willingness to pay, disability [MIDAS (22, 23)], quality of life [EuroQol (24)], optimism [Life Orientation Test (LOT) (25)], mastery (26), and coping (27). Of the 312 subjects who successfully completed the screening interview, 310 (99.4%) agreed to participate in the mail survey. A total of 201 (65%) mailed questionnaires were returned.
The WTP questionnaire elicits subjects’ willingness to pay for relief of the pain and associated symptoms of a migraine attack (Fig. 2). The survey contains a total of 17 questions divided into four sections: speed of relief (five questions), consistency of relief (four questions), side-effects (four questions), and recurrence (four questions).
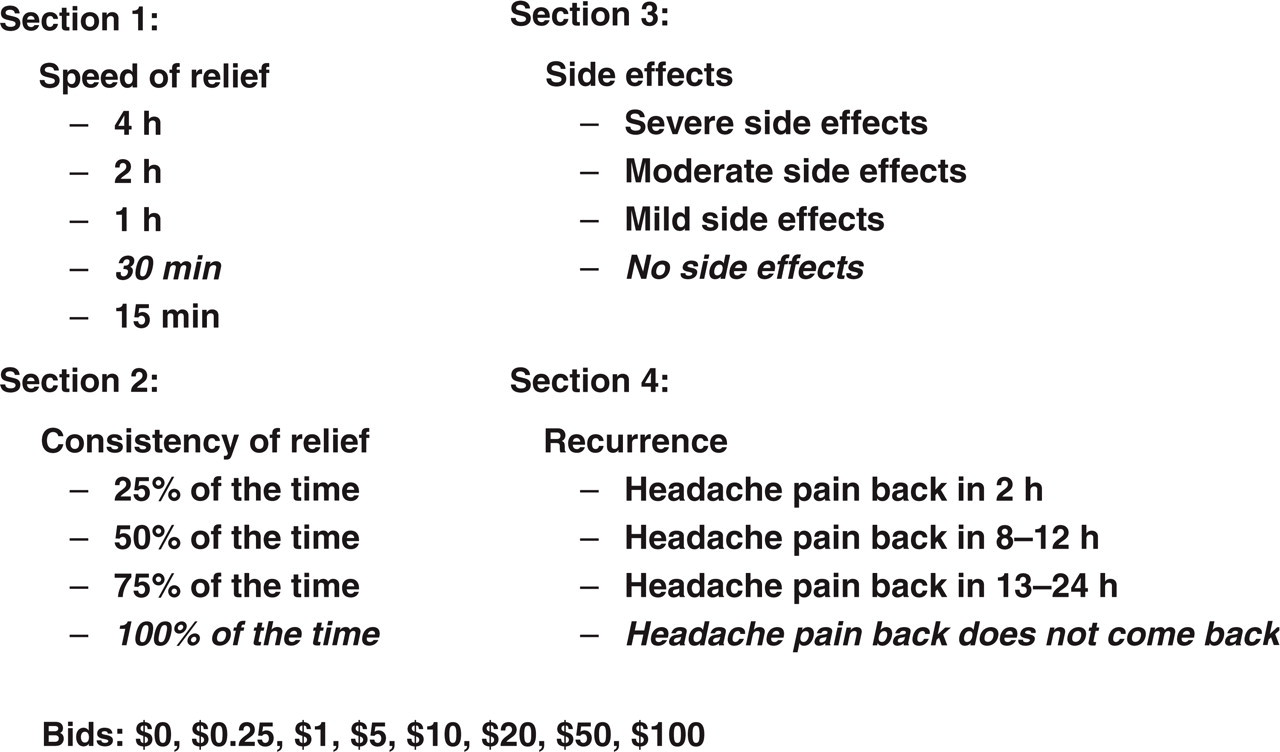
Content and organization of the willingness to pay questionnaire.
Subjects were asked to choose which dollar amount they would be willing to pay, out of pocket, for headache medications with various treatment attributes. Subjects were asked to assume that they would have to pay the entire cost of the drug with their own money.
The questionnaire is based upon the following relief scenario (base case): speed of relief (complete relief in 30 min), consistency of relief (complete relief 100% of the time), no side-effects, and no recurrence. Within each section (speed, consistency, side-effects, and recurrence), only one characteristic was varied. For example, in the speed section, speed was varied from 15 min to 4 h, but the other characteristics were held at base case value (i.e. complete relief 100% of the time, no side-effects, and no recurrence). The base case was repeated in each section to assess the test–retest reliability of the questionnaire.
Since this survey was designed to be a self-administered mail survey, the questions were presented in a multiple-choice format. Subjects indicated how much they would pay for each relief scenario; the range of bids ($0, $0.25, $1, $5, $10, $25, $50, $100) was selected to encompass the retail prices of currently available prescription and over-the-counter migraine treatments.
Statistical analysis
Pearson's χ2 statistic (categorical data) and
The cumulative proportion of subjects willing to pay each price was calculated for each question of each scenario. Friedman's χ2 statistic was used to test for significant differences in the WTP distributions within each section, and to test for significant differences in the WTP distributions of parallel questions across sections.
In order to measure the internal consistency reliability (correlation between answers to different questions about the same concept), Cronbach's α was calculated on the 14 unique questions of the WTP questionnaire. Only the first response to the repetitive question was included in the Cronbach's α calculation.
Friedman's χ2 test, which is appropriate for testing for differences in variables that involve repeated measures, was used to determine the concordance in WTP for relief among the four repetitive questions. In order to better understand the differences between subjects who increased the amount they were willing to pay, decreased the amount they were willing to pay, or held constant the amount they were willing to pay, Fisher's exact test was used to conduct subgroup analyses based on demographic variables, migraine characteristics, and psychological variables. Change in willingness to pay was based on the difference between the first and last response to the repeated question. The following categories were used to define the subgroups: age (0–24, 25–34, 35–44, 45–54, ≥ 55), gender (male, female), race (Caucasian, non-Caucasian), education (high school, some college, college, graduate school), income (10 000–19 000, 20 000–39 000, 40 000–59 000, ≥ 60 000), headache duration (0–24 h, ≥ 25 h, always medicates/don’t know), headache frequency (per year) (6–25), MIDAS (I/II, III/IV), EuroQol (≥ median healthstate, < median healthstate), LOT [optimists (≥ median of mean LOT), pessimists (< median of mean LOT)], mastery [high mastery (≥ median of mean mastery), low mastery (< median of mean mastery)], coping (≥ median number of coping responses, < median number of coping responses).
In order to asses whether the questionnaire represented the concepts it was intended to measure (content validity), we looked at the subjects’ responses to see if they understood the differences between the relief scenarios within each section, and found each section meaningful.
A series of logistic regression analyses were conducted using the base case scenario (Section 1, Question 4) as the dependent variable. The dependent variable was defined as a dichotomous variable: low ($0, $0.25, $1, and $5) and high ($10, $20, $50, and $100). The dependent variable was not analysed by comparing those willing to pay ($0.25–$100) vs. those unwilling to pay ($0) because the sample size in the group unwilling to pay ($0) (n = 7) was too small for analysis. Variables were considered significant predictors of WTP if P < 0.2 because this was an exploratory data analysis. Since this was one of the first studies of WTP in migraine, more relaxed criteria were permitted to learn as much as possible about the subject area.
Results
Responders vs. non-responders
Of the 310 subjects who received the mailed questionnaire, there were 201 responders and 109 non-responders (Fig. 1). The responders were similar to the non-responders for most demographic features, including gender, education, and marital status. However, responders were slightly older (mean age: responders 41.7 years, non-responders 37.7 years; P < 0.002) and more likely to be Caucasian (responders 80.1%, non-responders 66.1%; P = 0.008) than non-responders (Table 1). There were no significant differences between the responders and non-responders for any of the migraine characteristics (Table 2).
Demographic features, responders vs. non-responders

P-value calculated using χ2 statistic.
The following categories were used to calculate the χ2 statistic: Caucasian, non-Caucasian.
The following categories were used to calculate the χ2 statistic: married, non-married.
Migraine characteristics, responders vs. non-responders
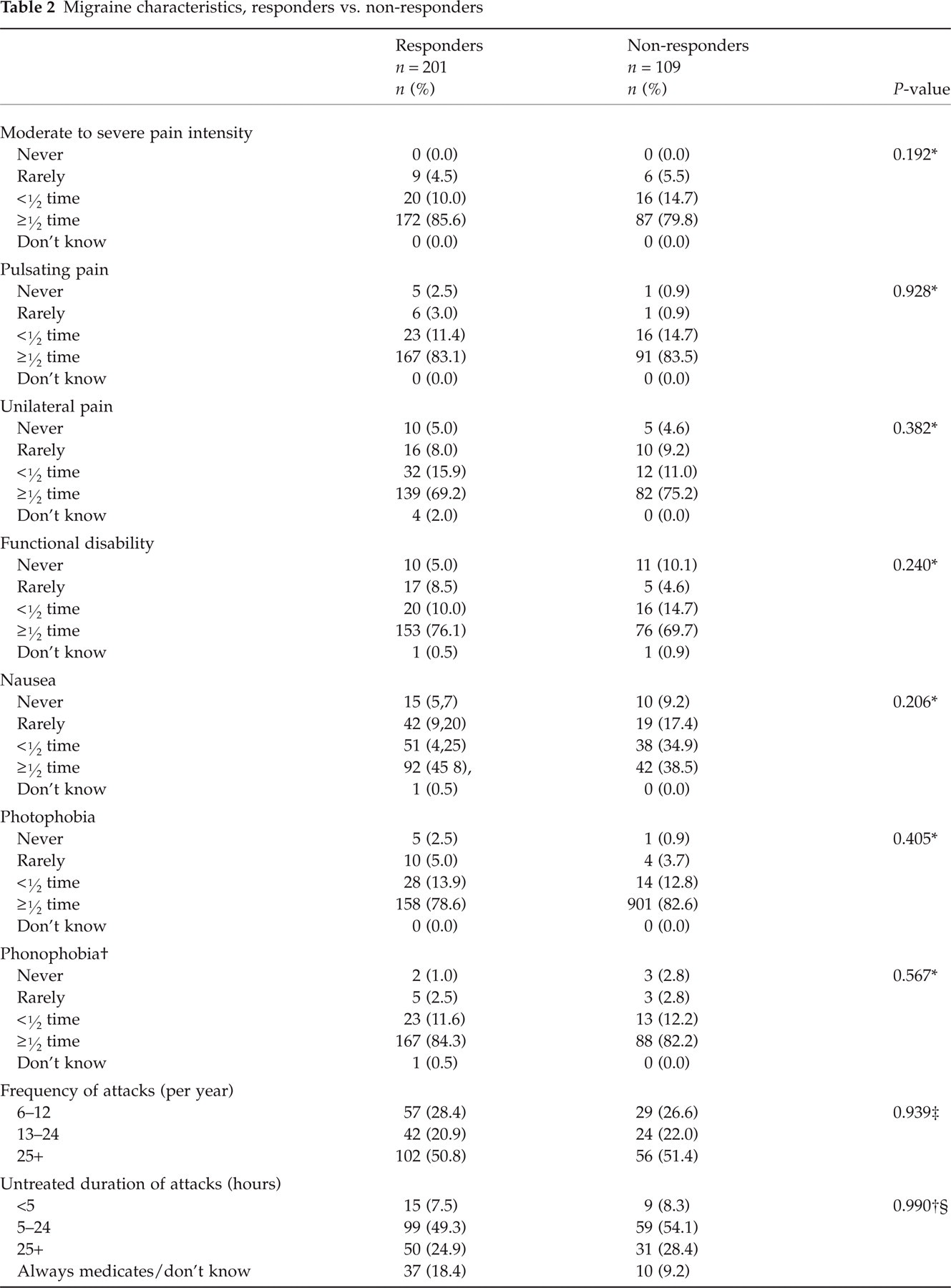

P-value calculated using χ2 statistic and the following two categories: (i) never/rarely, less than half the time, and (ii) ≥ half the time.
Responders n = 198; non-responders n = 107 due to missing data.
P-value calculated using χ2 statistic.
The following categories were used to calculate the χ2 statistic: < 5, 5–24, and 25 +.
P-value calculated using
Migraine characteristics
The overwhelming majority of subjects reported moderate to severe pain (85.6%), pulsatile pain (83.1%), unilateral pain (69.2%), and functional disability (76.1%) with their migraine attacks. Associated symptoms were also common: 45.8% of subjects reported nausea, 78.6% reported photophobia, and 84.3% reported phonophobia with the majority of their attacks. Approximately 50% of subjects experienced more than 25 migraine attacks per year. Most subjects’ (49.3%) migraine attacks lasted between 5 and 24 h. The mean age at onset was approximately 21 years. Based on the total MIDAS score, approximately one-quarter of the population fell into each of the four MIDAS grades. According to the MIDAS scale, higher scores indicate increased disability. Approximately 23% of the responder population was classified as Grade I (MIDAS score 0–5), 22.7% Grade II (MIDAS score 6–10), 25.9% Grade III (MIDAS score 11–20), and 28.1% Grade IV (MIDAS score > 20) (Table 2).
Reliability and validity
The Cronbach's α for the WTP questionnaire was 0.90, indicating high internal consistency reliability, and that the questionnaire was measuring the broad concept of willingness to pay for migraine relief. The Spearman's correlation coefficients comparing the responses to the four repetitive questions were also high, ranging in value from 0.71 to 0.77. All correlations were statistically significant (P < 0.001), indicating good test–retest reliability.
The Friedman's χ2 statistic was used to determine the concordance between the proportion of subjects willing to pay for relief in each of the four repetitive questions. There were significant differences (P < 0.001) in the proportions of subjects willing to pay for relief each time the base case scenario was asked.
To explore this relationship further, WTP was analysed in various subgroups defined by demographic, headache, and psychological characteristics. There was no significant difference in the proportion of subjects willing to pay in the subgroups defined by age, gender, education, income, headache duration, pain intensity, mastery, LOT, coping, or EuroQol. However, non-Caucasians, people with more frequent headaches, and people with more disability (MIDAS Grades III and IV) were significantly more likely to increase their bid.
The content validity of the questionnaire is evidenced by the fact that the proportion of subjects willing to pay for relief increased significantly as the relief scenario improved (see below). Furthermore, based on the questionnaire responses, subjects understood the differences between relief scenarios within each section, and found each scenario meaningful.
Cumulative number and proportion of subjects willing to pay
Speed of relief (complete relief by specified time points)
Subjects were willing to pay significantly increasing amounts of money for relief that occurred sooner. Approximately 45% of subjects were willing to pay at least $1 for complete relief in 4 h. For complete relief in 2 h, 58.8% were willing to pay $1 or more. For complete relief in 1 h, 77.8% were willing to pay at least $1 and 41.2% of subjects were willing to pay at least $5. For complete relief in 30 min, 87.8% were willing to pay at least $1, 60.7% were willing to pay $5 or more, and 31.6% were willing to pay $10 or more. For complete relief in 15 min, 75.9% were willing to pay $5 and 45.6% were willing to pay $10 (Fig. 3).

Cumulative per cent of subjects willing to pay for complete relief at specified time points.
Consistency of relief
The proportion of subjects willing to pay for consistency of relief increased significantly as the consistency of relief increased. Only 58.2% were willing to pay $0.25 or more for complete relief within 30 min that occurred only 25% of the time. For complete relief that occurred 50% of the time, 51.0% were willing to pay at least $1. Approximately 44% of subjects were willing to pay $5 or more for complete relief that occurred 75% of the time, while 73.2% were willing to pay $1 or more. For complete relief that occurred 100% of the time, 66.2% of subjects were willing to pay $5 or more (Fig. 4).

Cumulative per cent of subjects willing to pay for consistency of relief at specified time points.
Lack of side-effects
Subjects were willing to pay significantly greater amounts of money for less severe side-effects. Only 26.3% of subjects were willing to pay $0.25 or more for a migraine medication that caused severe side-effects, despite the promise of complete relief in 30 min, 100% of the time, with no recurrence. For a migraine medication associated with moderate side-effects, 59.9% of subjects were willing to pay $0.25 or more. More than half of the subjects (57.2%) were willing to pay $1 or more for a migraine medication that caused mild side-effects. For a migraine medication with no side-effects, 41.2% of subjects were willing to pay $10 or less, and 70.6% were willing to pay at least $5 (Fig. 5).
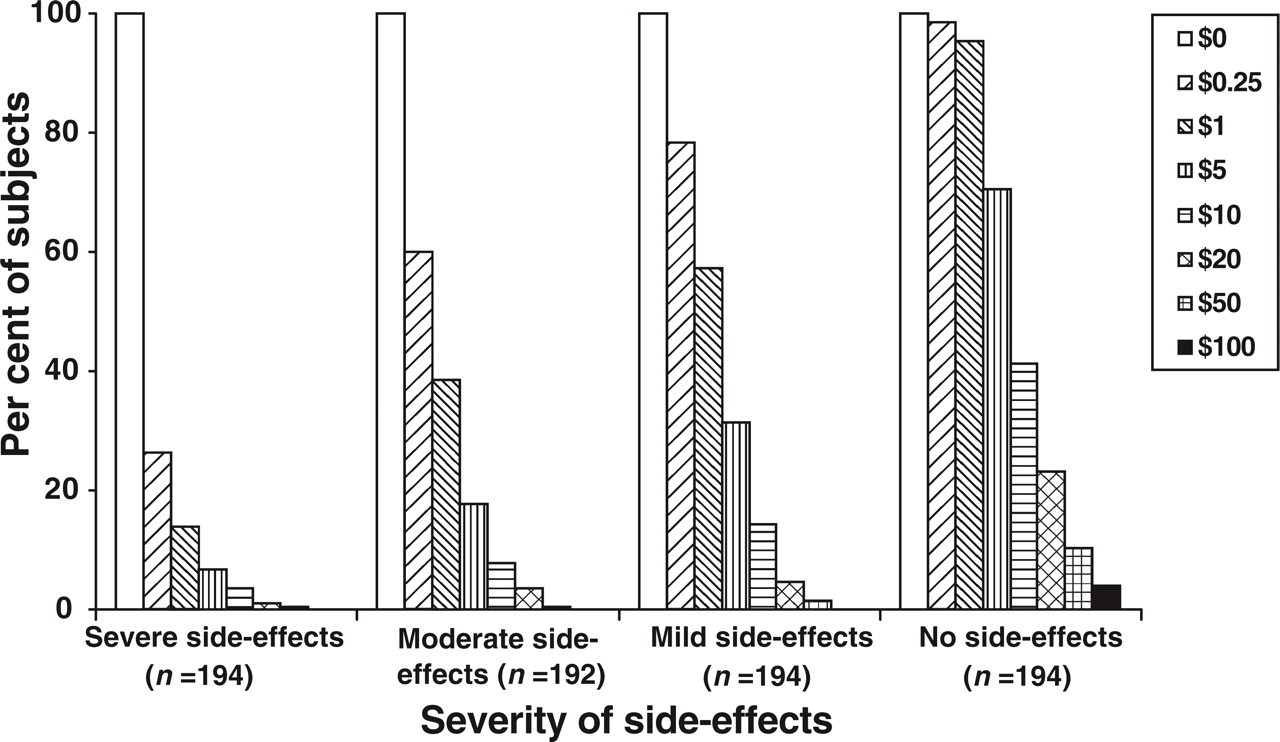
Cumulative per cent of subjects willing to pay for lack of side-effects at specified time points.
Lack of recurrence
Subjects were willing to pay significantly more money for a migraine medication that would relieve the pain for a longer period of time. Fifty-seven per cent of subjects were willing to pay only $0.25 or more for a migraine medication that worked for 2 h, while 84.5% would pay the same amount for a migraine medication that relieved the pain for 8–12 h. If the migraine medication relieved the pain for 13–24 h, 42.0% would pay $5 or more and 72.5% would pay $1 or more. Almost 50% of subjects (45.6%) would pay $10 or more for a migraine medication which relieved the pain for the entire duration of the attack (Fig. 6).

Cumulative per cent of subjects willing to pay lack of recurrence at specified time points.
All sections
The WTP distributions were significantly different for each set of parallel questions in different sections. The comparison between complete relief in 4 h, complete relief 25% of the time, severe side-effects, and headache back in 2 h demonstrates that the subjects were significantly less likely to pay for severe side-effects or complete relief that took 4 h. The subjects were also significantly less likely to pay for moderate side-effects, in comparison with complete relief in 2 h, complete relief 50% of the time, and headache back in 8–12 h. Comparing the third question in each section (complete relief in 1 h, complete relief 75% of the time, mild side-effects, and headache back in 13–24 h) reveals that the subjects were least likely to be willing to pay for mild side-effects, in comparison with the other relief scenarios.
Logistic regression analysis
Logistic regression analyses were conducted using the first question that assessed the base case scenario. The dependent variable was defined as a dichotomous variable: category 1 represented the willingness to pay variables $0, $0.25, $1, and $5, while category 2 included the willingness to pay categories $10, $20, $50, and $100. A series of models were run (see Methods) to create the final model that contained the following variables: race, graduate school, high income (≥$60 000), currently pays ≥ $5 or ≥ $11 for headache medication, MIDAS Grade III, long duration (>24 h), unknown duration, EuroQol, coping, and direct action. The following variables were significant predictors of high willingness to pay: graduate school, currently pay $5, pay $11, MIDAS Grade III, headaches of long duration and unknown duration, and use of few coping mechanisms (Table 3). Subjects who typically paid $5 for each prescription migraine refill were much more likely to be in the high WTP category compared with subjects who did not report using prescription migraine treatments [odds ratio (OR) 3.4, 95% confidence interval (CI) 1.25, 9.41]. Subjects who typically paid $11 for each prescription migraine refill were more likely to be in the high WTP category compared with people who did not report using prescription migraine treatments (OR 5.42, 95% CI 1.30, 22.54). Similarly, MIDAS Grade III subjects were 3.03 times more likely to be willing to pay higher amounts compared with subjects in MIDAS Grade I (OR 3.03, 95% CI 1.24, 7.37). Subjects who attended graduate school were 0.20 times less likely than those who had completed high school or less to be in the high willingness to pay category (OR 0.20, 95% CI 0.05, 0.90). Compared with those with headaches of short duration (24 h), subjects with headaches of long duration were more likely to be in the high WTP category (OR 1.99, 95% CI 0.78, 5.08). In contrast, subjects with headaches of unknown duration were one-third as likely to be willing to pay higher amounts for relief (OR 0.25, 95% CI 0.07, 0.97). Subjects who reported using many coping methods were 0.40 times less likely to be in the high WTP category compared with those who reported using fewer coping mechanisms (OR 0.40, 95% CI 0.18, 0.90).
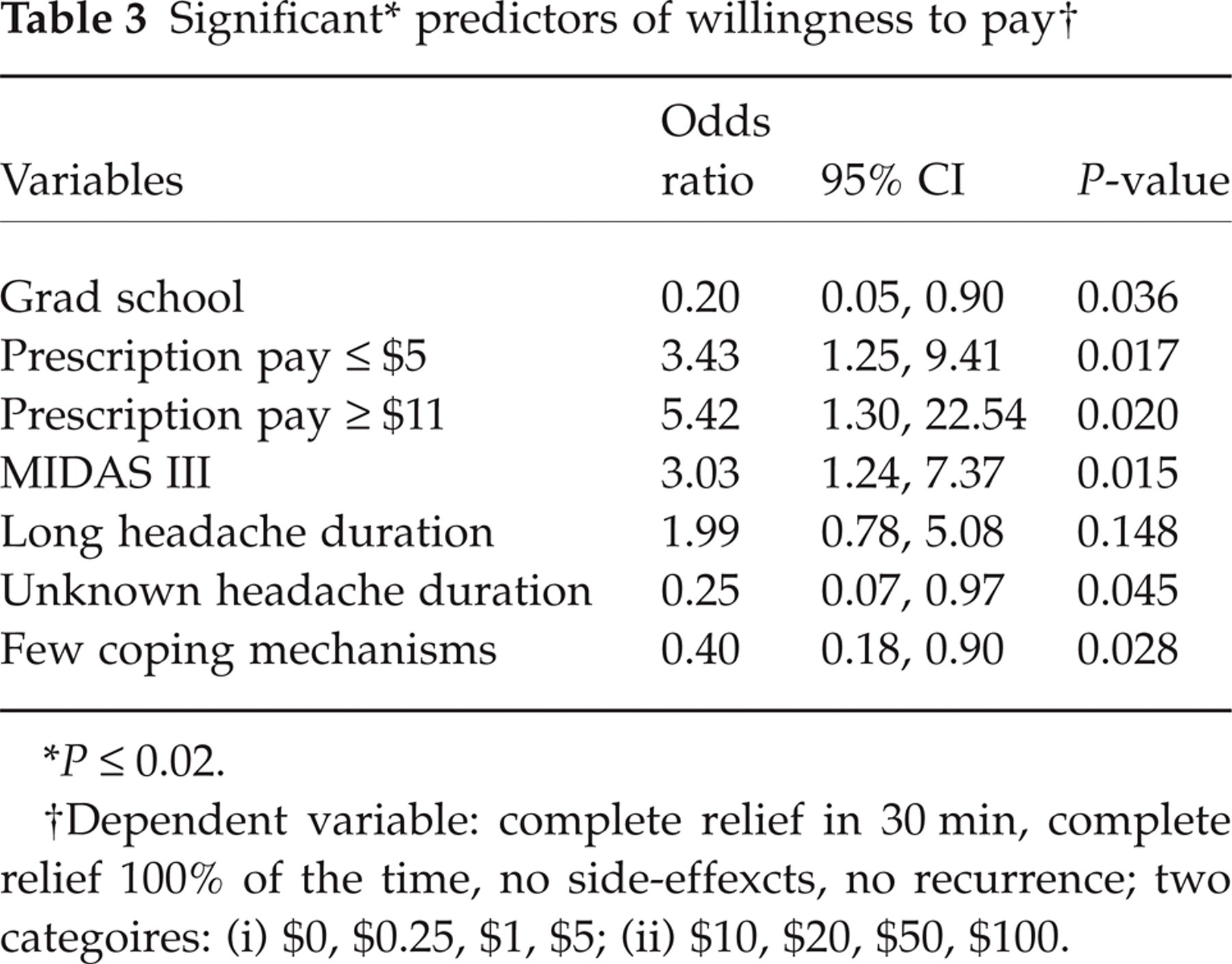
P ≤ 0.02.
Dependent variable: complete relief in 30 min, complete relief 100% of the time, no side-effexcts, no recurrence; two categoires: (i) $0, $0.25, $1, $5; (ii) $10, $20, $50, $100.
Discussion
As expected, migraine sufferers in this study were willing to pay increasing amounts of money for migraine medications with improved treatment attributes. Subjects were willing to pay a median price of $5 per attack for a migraine medication that promised complete relief in 30 min, 100% of the time, with no recurrence and no side-effects. In addition, if one compares parallel questions across scenarios, it is clear that subjects were more likely to pay for speed of relief and least likely to pay for a drug associated with side-effects. Several variables were strong predictors of WTP. These variables included: headaches of long duration, headaches of unknown duration, MIDAS Grade III, graduate school, use of few coping mechanisms, and current payments of $5 or $11 for headache medication.
Since the WTP questionnaire was a newly developed survey, we examined its reliability and validity. The high Cronbach's α (0.9) for this survey demonstrates a high level of internal consistency reliability. That is, the various treatment characteristics measured by the questionnaire reflect a broad underlying construct (willingness to pay for better treatment) regardless of the specific treatment attributes. However, the Cronbach's α tends to be high when there are high correlations between the questions, and when there are many questions asked about a topic, especially if the questions are similar to each other (28). This may contribute to the very high Cronbach's α we report.
The Spearman's correlation coefficient demonstrated good test–retest reliability. Further exploration of the relationship between the repetitive questions demonstrated that the proportion of subjects willing to pay higher amounts increased each time the question was asked. In general, people with more severe migraine attacks were more likely to increase their willingness to pay bid each time the question was asked. Results from the subgroups who were more likely to increase their bid may be less reliable.
In this version of the questionnaire, questions within each section were ordered so that the relief scenario went from worst to best within each section. Because we did not vary order, we cannot determine if the sequence of the questions impacted participants’ responses. In the future, the questions within each section should be presented in random or counterbalanced order.
Within each section, the proportion of subjects willing to pay for relief increased significantly as the relief scenario improved. This finding helps establish the content validity of the questionnaire. Subjects understood the differences between relief scenarios within each section, and found each scenario meaningful.
The WTP figures reported in this study are lower than those reported in the other published WTP study in migraine (18). Lenert conducted an internet-based WTP study among self-identified migraine sufferers. In this study, the out of pocket monthly cost for an ‘ideal’ migraine therapy was $130. The difference in the median willingness to pay values may be accounted for, in part, by the different subject populations. Lenert's population was highly educated (88% with college education), had relatively high household income levels, and a large number (28%) of participants reported daily or continuous headaches. In addition, participants who self-select for an internet survey may have more severe migraine and a higher level of motivation to find relief than migraine sufferers in general. The authors state that these subject characteristics may have upwardly biased the WTP values compared with an epidemiological sample.
It is difficult to compare the WTP figures for migraine reported in this study with those of most other conditions. Other healthcare-related WTP studies focused on life-threatening conditions (15–17), issues that are highly emotional, such as in-vitro fertilization (29) or chronic disorders (30) present on a daily basis.
These WTP results are consistent with data on migraine-related healthcare utilization. In a recent study, Lipton et al. (31) reported that 31% of migraine sufferers had never consulted a doctor for headache, 21% had not consulted for at least 1 year (lapsed consulters), and only 48% had seen a doctor for headache in the past year. Given that migraine is characterized by severe pain and frequent disability, low rates of medical consultation are surprising. In addition, the use of prescription medication for migraine occurs at lower than expected rates, based on the pain profile of the disease. Lipton et al. reported that approximately 50% of migraine sufferers reported using over-the-counter medications to the exclusion of prescription drugs, 23% reported using prescription medications only, 23% reported using both prescription and over-the-counter, and 4% reported using no medication at all. Migraine sufferers in the study reported herein were only willing to pay a median price of 55p ($1) for a drug that matches the profile against which migraine treatments are measured, according to IHS clinical trial guidelines (32). This relief scenario promised complete relief in 2 h, complete relief 100% of the time, no side-effects, and no recurrence. The WTP results in this study are consistent with patterns of treatment use by migraine sufferers in the general population.
The patient preference for speed of relief and freedom from side-effects reported herein is broadly similar to patient preference data reported elsewhere. To better understand the treatment preferences of migraine sufferers, three studies surveyed participants regarding the treatment characteristics they considered most important in a migraine medication (14). Participants in all studies expressed a preference for a migraine therapy that provided rapid, complete relief. Lipton and Stewart (14) showed that the participants who were not completely satisfied with their migraine treatment complained that pain relief took too long (87%), was inconsistent (84%), or that the pain recurred (71%). Only 35% complained of side-effects. Luciani et al. found that migraine sufferers ranked ‘how well it works’, and ‘how fast it works’ among their top four preferences. Similarly, three of the top four preferences in the Caro et al. study were: a medication which ‘decreases the pain from the unbearable level in 30 minutes’, ‘starts to relieve the pain within 30 minutes’, and ‘relieves the pain completely in two hours’. While participants in the Luciani et al. study felt that the safety of the drug was important (‘how safe it is’ and ‘side-effects’), side-effects were of little importance in the Caro et al. study group. The Luciani et al. participants ranked the ‘cost of the drug’ as the least important attribute.
We identified a number of predictors of willingness to pay in multivariate models. Not surprisingly, subjects with headaches of long duration were more likely to be willing to pay higher amounts of money for relief. Subjects with more coping mechanisms were less likely to be willing to pay high amounts for relief.
Surprisingly, moderate (MIDAS Grade III), but not severe disability (MIDAS Grade IV) was a significant predictor of willingness to pay. These groups may differ in certain headache and personality characteristics that might influence willingness to pay. MIDAS Grade IV sufferers are more likely to be depressed (33) and may have given up on the possibility of excellent relief.
While it is logical that subjects who pay for prescription migraine treatment were more likely to be willing to pay than those who do not use prescription treatments, it was surprising that paying $5 or less or $11 or more were significant predictors of willingness to pay, but the intermediate payment ($6–$10) was not. The typical copay amount for those with prescription coverage is approximately $6–$10. Therefore, although subjects were instructed not to consider insurance coverage when valuing scenarios, it is possible that those with prescription coverage valued the scenarios with a different set of criteria than those without prescription coverage. The amount they currently pay for prescription treatment may not be a predictor of willingness to pay because they will always pay the same amount, regardless of the treatment attributes.
It is unclear why people who attended graduate school would be less likely to pay high amounts of money for relief. In this study, neither high income nor higher education, a surrogate for high income, were significant predictors of high WTP values. Based on other healthcare-related WTP studies, high income is usually expected to be associated with a high likelihood of being willing to pay (29, 34–36). The association between income and willingness to pay may be less dramatic in this study compared with other studies because the amount of money to treat one migraine attack may have been too small to be affected by income level. In addition, some of the other WTP studies concerned life-threatening conditions that might be associated with greater willingness to pay.
Because of population-based recruiting methods, the present results should be applicable to migraine sufferers in the general population. There were few inclusion and exclusion criteria, and participants in this study were selected from a population-based database of headache sufferers. The enrolment criteria for the study required that subjects were between 18 and 65 years of age, experienced their first migraine before age 50, and suffered from at least six migraine attacks (with or without aura) per year. This age range was chosen because headaches that begin after age 50 are more likely to be attributable to a secondary cause and less likely to be migraine. A minimum migraine frequency of six per year was chosen so that the WTP questions would be relevant to the participants. A migraine sufferer with less frequent headaches might be unable to recall accurately the feelings associated with a migraine attack. The imposition of these enrollment criteria limits the generalizability of study results. It is unlikely that the minimum migraine frequency inhibited enrollment because most migraine sufferers experience approximately one to two attacks each month (21).
Approximately 65% of subjects returned the survey. Given the potential selection bias, it is reassuring that the demographic features and migraine characteristics of the study subjects were consistent with those found in the general population of migraine sufferers (37, 38). Although the subjects in this study reported migraine characteristics similar to those of the general population, they are probably not representative of migraine patients in the doctor's office. Since migraine sufferers who visit the doctor usually have more severe disease characteristics, these patients may have been willing to pay more money for relief than the subjects included in this study.
Those who returned the survey were generally similar to those who did not respond. However, responders tended to be older (P = 0.002), and were more likely to be Caucasian (P = 0.008) than non-responders. This finding is consistent with the literature, which demonstrates that, in general, research participants are more likely to be older and Caucasian (39). There were no significant differences in the migraine characteristics reported by the responders and non-responders.
Contingent valuation studies are sometimes subject to relational bias, i.e. the attributes of the product being valued can be compared with similar goods. This study attempted to avoid relational bias by asking subjects to answer the questions as if they were using their own money to pay for the treatments. However, the prices that subjects previously paid for migraine treatments were a significant predictor of willingness to pay, suggesting that relational bias remains an issue. Relational bias might also be an issue in countries where migraine sufferers do not traditionally pay for their healthcare out of pocket. While subjects in those countries could be asked to make the same assumption that they must pay out of pocket for the drugs being offered, the results would probably still be influenced by previous experiences in paying for healthcare.
Application of the contingent valuation method to a migraine population further explained the burden of migraine on individual sufferers by expressing the impact in quantifiable terms. Future research should improve upon the methodology employed here. For example, including a control group in the study would help put the willingness to pay amounts reported by migraine sufferers into context. In addition, it would be helpful to redesign the questionnaire in such a way to enable more direct comparison of the migraine treatment attributes.
Footnotes
Acknowledgements
This research was supported by Bristol-Myers Squibb (New York, NY, USA). These findings were presented at the American Headache Society Scientific Meeting, June 2001.