
Abstract

Spontaneous intracranial hypotension may be complicated by persistence of headaches, subdural haemorrhage and, rarely, cerebral venous thrombosis. We describe a case of a 31-year-old female who developed cerebral venous thrombosis after spontaneous orthostatic headache, followed later by the development of a dural arteriovenous fistula. This combination of complications after orthostatic headache has not been previously described. Physicians managing patients with orthostatic headaches should consider these complications if patients develop a change in the headache quality or pulsatile tinnitus.
Case report
The patient is a 31-year-old healthy woman who woke with a shooting pain in her right eye followed over 1 h by a holocephalic headache. This led to an emergency room visit where a CT scan of the head was performed and was negative. She was treated for presumptive migraine. The quality of the headache changed over the course of the next 24 h. She developed a severe posterior occipital headache provoked by sitting, standing, or bending forward. The headache would come on within seconds of an upright position and would be accompanied by nausea. She returned to the emergency room again for persistent orthostatic headaches. She was hospitalized. A noncontrast MRI was performed and was normal. She was again treated with general analgesics for presumed migraine.
Over the next one week, the patient had a change in her headache. She no longer had the orthostatic quality to the headache. She developed a severe, persistent holocephalic headache associated with nausea.
By three weeks, in addition to the headaches, patient was experiencing a nonpulsatile noise in her head and alteration in hearing. A repeat MRI of the head revealed a hyperintense region along the sagittal sinus suggestive of thrombosis in addition to diffuse dural meningeal enhancement. An MRV revealed thrombosis of the sagittal and right transverse sinus. A spinal tap demonstrated an opening pressure of 3 cm of water. A radionuclide cisternogram was negative for a CSF leak. Patient was treated with warfarin for the thrombosis and analgesics and caffeine for her headaches.
After approximately four weeks of therapy, her headaches dramatically improved. She was first seen by the authors at that time. She had no family or personal history of clotting disorders and laboratory tests for hypercoagulable states were negative. She was not pregnant and not on oral contraceptives. Her neurologic examination was normal. Repeat MRI demonstrated partial recanalization of the right transverse sinus and a normal sagittal sinus (Fig. 1). Treatment was continued.
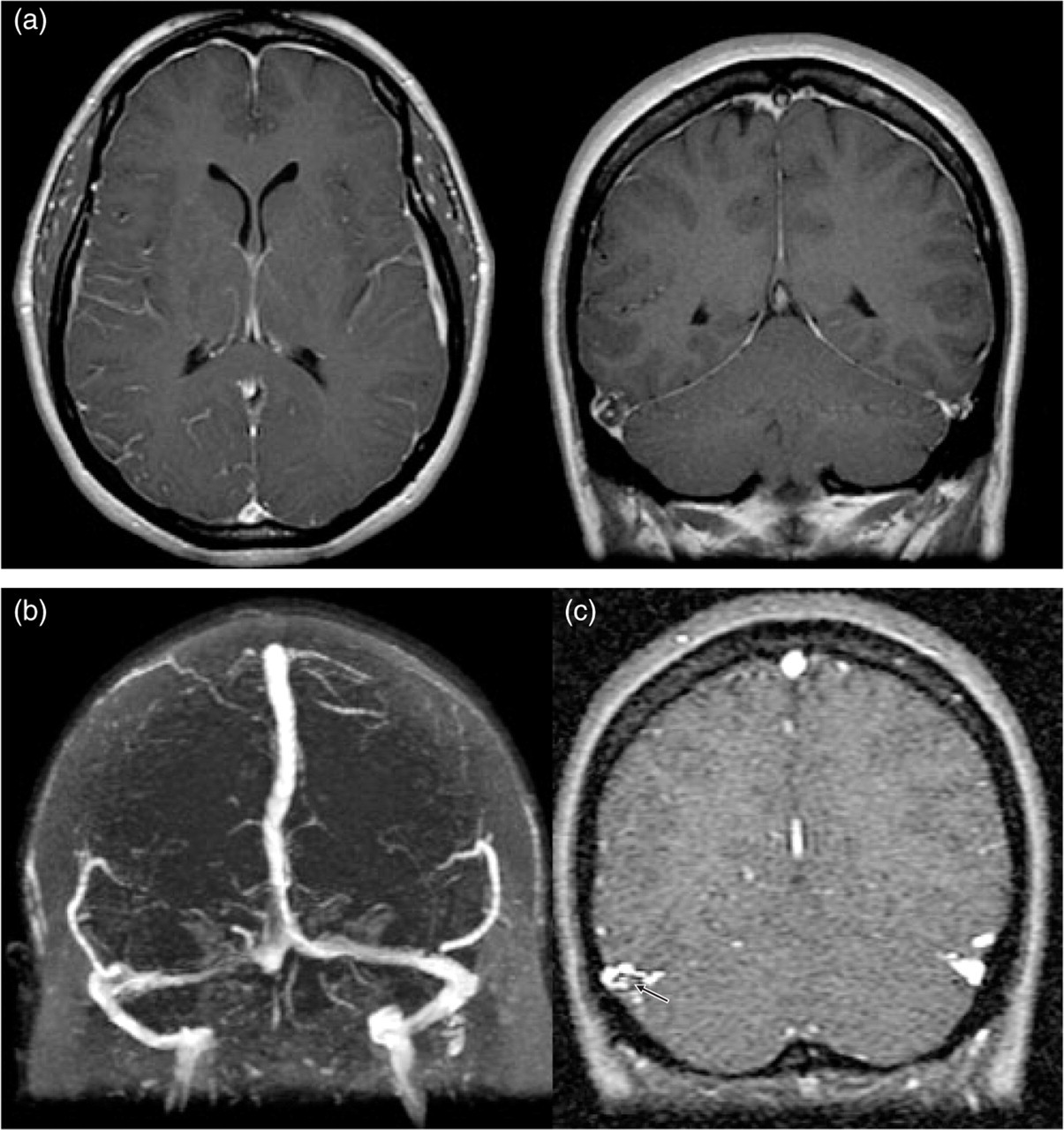
(a) T1 sequences with gadolinium reveals diffuse pachymeningeal enhancement. (b) MR Venogram reveals the partial recanalization of the right transverse sinus. (c) MR venogram source images show the partially recanalized right transverse sinus with small amount of remaining clot (arrow).
Approximately one month later, over the course of a single day, patient felt like a balloon was blowing up in her head. She continued to have a pressure sensation in her head. She also developed right-sided pulsatile tinnitus. Examination revealed a bruit over the right mastoid region. Warfarin was discontinued. Angiography revealed a right transverse sinus dural arteriovenous fistula (DAVF) (Fig. 2). There was no evidence of cortical venous drainage, however, due to the persistent, disabling pulsatile tinnitus she was treated with Gamma KnifeTM radiosurgery followed by particulate embolization of the accessible external carotid feeding vessels.

Angiography reveals a right transverse sinus dural arteriovenous fistula fed by the right occipital, ascending pharyngeal, and middle meningeal arteries.
Discussion
We believe this is a unique case of symptomatic spontaneous CSF leak followed by venous thrombosis and subsequent development of a DAVF.
Our patient developed a typical low–pressure headache clinical syndrome with posterior head pain aggravated in the upright position. In the upright position, intracranial CSF pressure falls and results in traction of the supporting structures. Traction on the meninges results in pain. Traction on the dural venous sinuses results in compensatory venous sinus dilatation due to the Monroe-Kellie doctrine (1). Thus it is theoretically possible that stasis in the venous system may predispose to venous thrombosis in this situation.
Approximately 20 cases in the literature have reported venous sinus thrombosis after spinal tap, myelography, or epidural injection confirming this theoretical possibility. In most of these cases, patients developed a low-pressure headache which then lost its postural component (2). In addition, most had contributing risk factors including hypercoagulable states. Three case reports describe venous thrombosis after spontaneous CSF leaks (3, 4). In two of these cases there were potential contributing risk factors. We believe our case adds to this literature as a case of spontaneous CSF leak followed by venous thrombosis, although our patient had no identified hypercoagulable state.
While it is known that venous thrombosis may predispose to formation of DAVF (5), the sequence of events described in this case have not been previously documented. Awad et al. (6) have previously described the potential relationship of venous thrombosis and DAVF. Thrombosis of the dural venous sinuses results in altered flow such that embryonic arteriovenous connections open. Subsequently arterial feeders are recruited. Venous hypertension may result and alter venous drainage patterns. Cortical venous drainage may predispose to potential haemorrhage.
One important limitation to our theory is that patient did not meet I.H.S. criteria for low pressure headache. This diagnosis requires the clinical syndrome in addition to either MRI, CSF, or myelography/cisternography findings compatible with this syndrome. In addition resolution of headache after blood patching is required in this diagnosis. Unfortunately our patient did not have a contrast MRI at the time of her clinical presentation and only had one after her venous thrombosis. We believe on the basis of her clinical symptomatology and subsequent sequence of events, however, that she did have a spontaneous CSF leak headache.
Physicians should consider venous thrombosis as a possible complication of low-pressure headaches especially in those where there is a change in the quality of the headache. In addition, development of DAVF may occur in this scenario and is usually heralded by change in headache quality and/or unilateral pulsatile tinnitus.