
Abstract
Mastocytosis is a clonal disorder of mast cells in both children and adults. It is characterized by overproliferation, accumulation and activation of the mast cells in different tissues (1–3). Mast cell hyperplasia can be restricted to the skin (cutaneous mastocytosis), or may also involve extracutaneous organs (systemic mastocytosis) such as skeleton, bone marrow, gastrointestinal tract, liver, spleen, lymph nodes and the CNS. Prevalence or incidence of the disease is unknown and is probably difficult to determine because of the underdiagnosis of the systemic disease without the cutaneous manifestation (4). Occurrence of cutaneous mastocytosis has been estimated as 0.1– 0.8% of patients visiting dermatology and allergy clinics (3). Resent studies suggest that mutations in the proto-oncogene c-kit resulting in mast cell proliferation and prevention of apoptosis may be involved in the pathogenesis of the systemic mastocytosis (5, 6). Typical symptoms can include skin lesions, the most frequently being urticaria pigmentosa (3, 7), pruritus, urtication, flushing, rhinorrhea, wheezing, shortness of breath, dyspepsia and diarrhea (1–3, 8). Headache is the most frequent neurological complaint in systemic mastocytosis (2, 9). Here, we report a case of the systemic mastocytosis associated with frequent headaches.
Case report
A 47-year-old female was presented at the Danish Headache Center. She was diagnosed with the systemic mastocytosis and referred from the Department of Dermatology for the evaluation of frequent headaches. Patient's mastocytosis-related symptoms included: skin lesions (urticaria pigmentosa), pruritus, dyspepsia and diarrhoea. The patient has had skin lesions for the past 20 years, and diagnosis of systemic mastocytosis was verified by skin biopsy 9 months ago and colon biopsy 7 months ago. She had a history of frequent episodes of headache since puberty. Both the patient's mother and daughter suffer from migraine without aura. At the admission she was taking a H2-receptor blocker (cimetidine), two H1-receptor blockers (cetirizine and hydroxyzine), and a SSRI (citalopram), and was receiving ultraviolet A therapy for the skin lesions. The neurological examination was normal except known monocular temporal hemianopsia due to previous retinal detachment. Cimetidine caused partial relief of the headaches, i.e. reduction in the number of severe attacks. After the first consultation the patient was instructed to complete a diagnostic headache diary (10) for the next 6 weeks. At the second visit patient's headaches were diagnosed according to International Headache Society (IHS) Classification criteria (11). Patient experienced 27 days with headache in a 6-week period. 19% of her headaches fulfilled criteria for migraine without aura and 81% for frequent episodic tension-type headache (Table 1). CT-scan of the head did not demonstrate any lesions in the brain. A daily dose of 10 mg of montelukast (Singulair®, MSD), a specific D4 leukotriene receptor antagonist, was then prescribed. During the 11 weeks of treatment headache frequency was reduced to 2 episodes of headache fulfilling criteria for infrequent, episodic tension-type headache. The effect of the drug was already observed in the first week of the treatment. Unfortunately, montelukast was discontinued after approximately 3 months of treatment because of reported side-effects (swelling and pain in finger joints). However, it is unclear whether these symptoms were side-effects or manifestation of symptoms of systemic mastocytosis because symptoms remained after discontinuation of the drug. Patient began to complain of headaches again. Unfortunately, the diagnostic headache diary was not completed by the patient. However, she reported that frequency of her headaches gradually increased to 8 episodes per month in the following 3-months period. 80% of her headaches were like tension-type headaches (bilateral, pressing, associated with mild photophobia) and 20% of her headaches were like migraines without aura (throbbing, associated with nausea, photophobia and aggravated by physical activity). Patient is being followed at the Danish Headache Centre.
Percentages of headache characteristics in a patient with systemic mastocytosis during the 6-week period
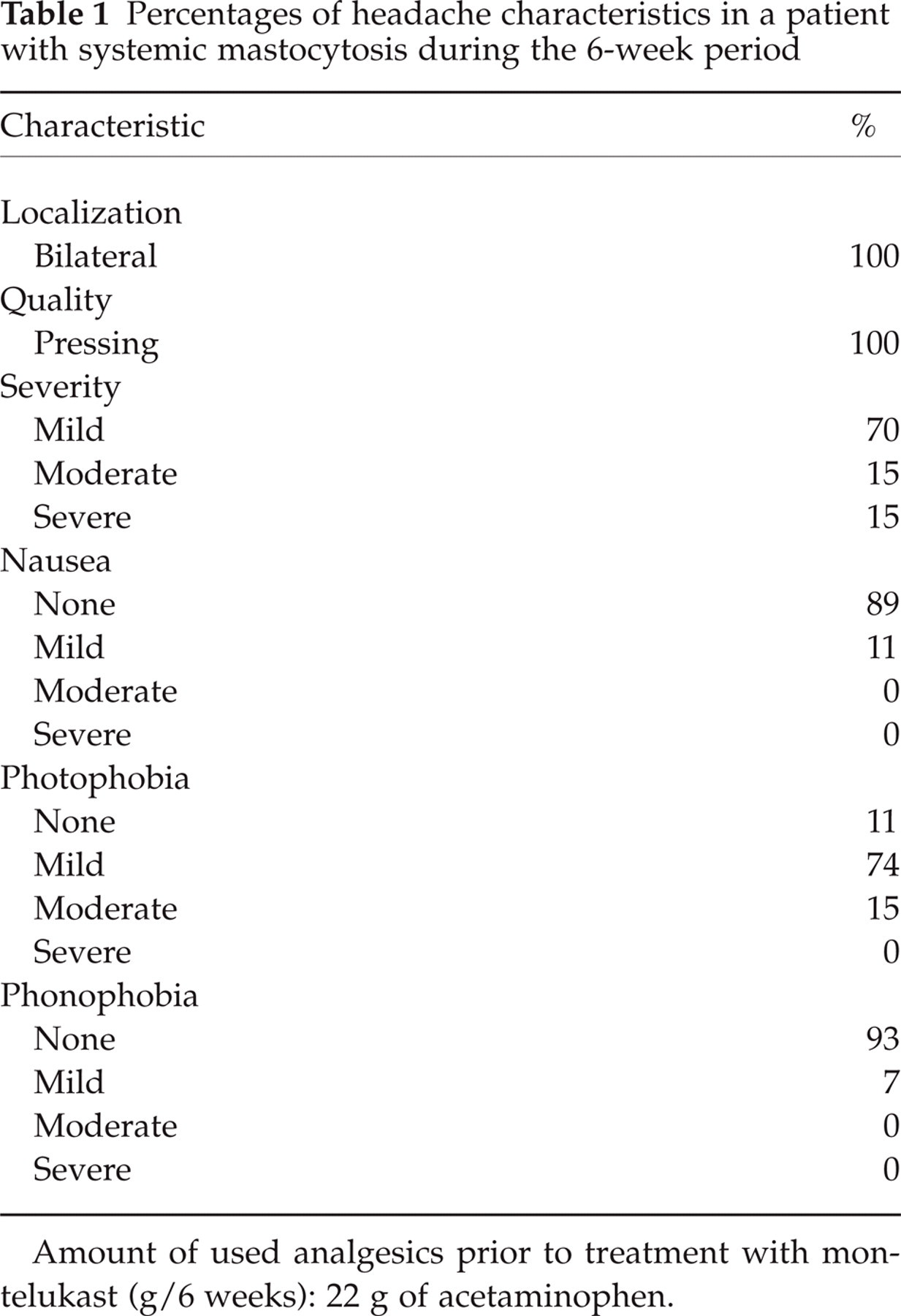
Amount of used analgesics prior to treatment with montelukast (g/6 weeks): 22 g of acetaminophen.
Discussion
It has been reported that headache in systemic mastocytosis has heterogenic presentation (2). It may be a mild frontal, dull, nonpounding headache; a headache with migraine characteristics; and a headache associated with rhinorea, pruritus, and lacrimation suggestive of cluster variety (9, 12–16). However, headaches in systemic mastocytosis have never been classified according to IHS criteria (11). In our patient we describe two types of headaches: tension-type-like and migraine-like (migraine without aura).
The pathophysiological mechanisms of headache in patients with systemic mastocytosis are unknown. It is believed that release of inflammatory mediators from mast cells may be responsible for development of headache (2). Histamine and leukotrienes are among many mediators of mast cell that might be implicated in pathogenesis of headache in systemic mastocytosis (17). Animal migraine models have shown that histamine infusion cause immediate and reproducible dilation of meningeal blood vessels (18) and that H1-receptor antagonist inhibits neurogenic vasodilatation of meningeal blood vessels (18). In addition, substance P and calcitonin gene-related peptide, two major neuropeptides involved in nociceptive processing in migraine, can stimulate release of histamine from mast cells in dura mater in rats (19). It has also been reported that patients with migraine have increased plasma levels of histamine (20, 21). Systemic administration of histamine elicited an immediate headache during the infusion in healthy subjects, in patients with tension-type headache and migraine (22, 23). Patients with migraine experienced more severe throbbing/pulsating headache compared to patients with tension-type headache, who developed intermediate and more pressing headache, and healthy subjects with pressing headache (22). Moreover, intravenous histamine may induce a migraine attack in migraineurs several hours after the infusion (11, 23). It has been demonstrated that both H1- and H2-receptor blockers may abolish migraine attacks induced after the systemic administration of histamine (22, 23).
Leukotrienes may be involved in the pathogenesis of systemic mastocytosis (17). Bouchelouche et al. (24) have reported that the treatment with montelukast, a specific D4 leukotriene receptor antagonist, resulted in a decrease in suprapubic or perineal pain in patients with interstitial cystitis and detrusor mastocytosis. The authors suggested that mast cells might be involved in bladder neurogenic inflammation by releasing mediators such as leukotrienes (24). This may lead to the immune cell infiltration and sensitization of sensory neurons (24). Plasma levels of leukotriene may be increased during migraine attacks (17, 25). In an open-label study (26) with 17 patients with migraine it has been shown that montelukast may be effective as preventive treatment. Fifty-three percent of patients showed more than 50% reduction in frequency of severe attacks, and 41% showed a reduction greater than 60% (26). In another small open-label study (27) in children and adolescents with migraine and comorbid asthma, montelukast resulted in a decrease in headache frequency by approximately 12% per week. In summary, these data suggest that both tension-type-like and migraine-like headaches in systemic mastocytosis may be due peripheral sensitization induced by release of histamine and leukotrienes from mast cells. Our observation of reduced headache frequency by treatment with montelukast in the patient with systemic mastocytosis suggests that leukotriene antagonists may be effective in the treatment of headaches associated with this disorder.
In conclusion, we report two types of headache in a patient with systemic mastocytosis: tension-type-like and migraine-like headaches. Mediators of mast cell, histamine and leukotrienes, may be involved in development of frequent episodes of headache in patients with systemic mastocytosis and a specific D4 leukotriene receptor blocker, montelukast, may be tried as preventive treatment.
Footnotes
Acknowledgements
The patient kindly gave verbal consent so that this case could be reported. We are grateful for the critical comments on this manuscript given by Dr Rigmor Jensen and Dr Peer Tfelt-Hansen. The authors have no conflicts of interest.