
Abstract
Case Report
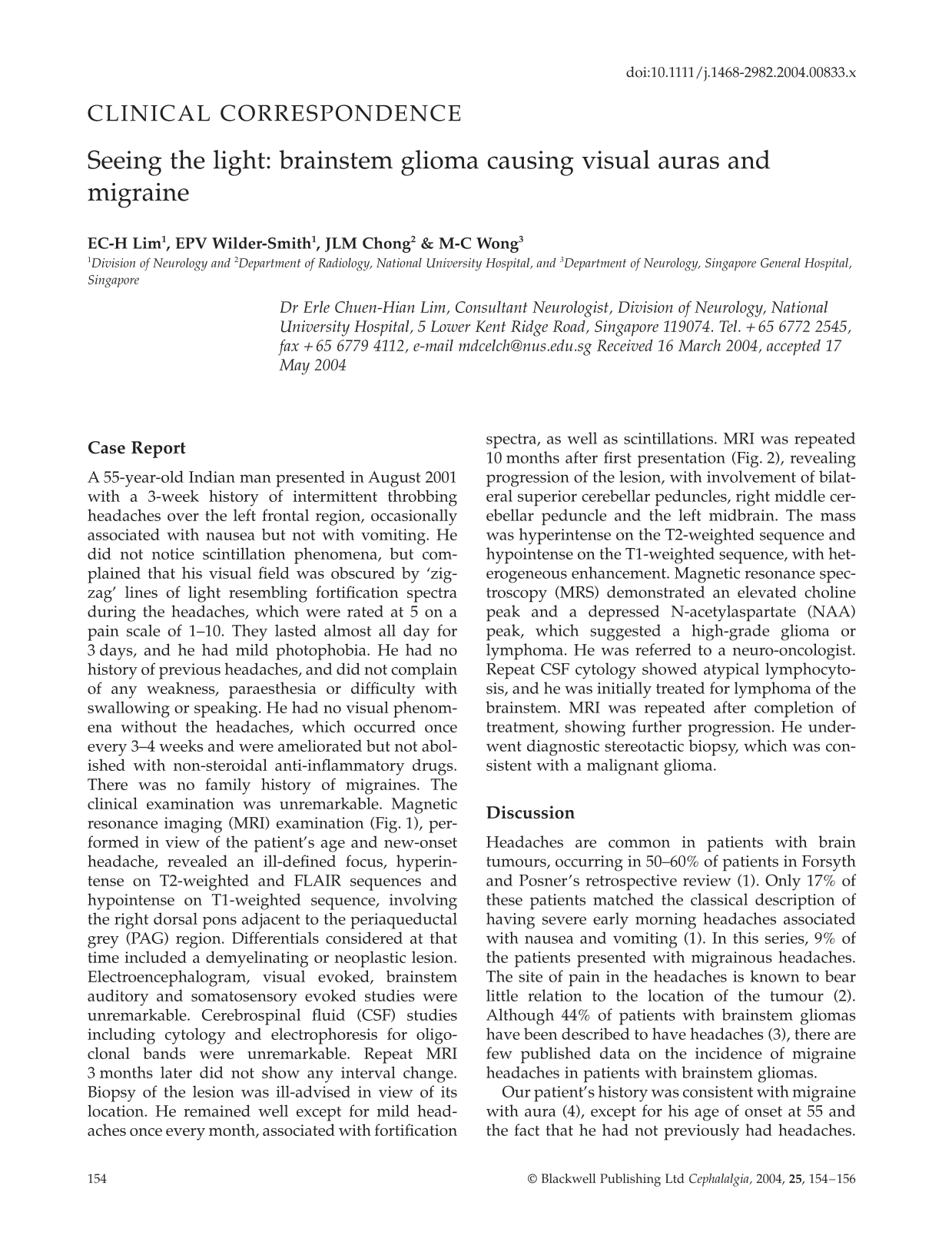
A 55-year-old Indian man presented in August 2001 with a 3-week history of intermittent throbbing headaches over the left frontal region, occasionally associated with nausea but not with vomiting. He did not notice scintillation phenomena, but complained that his visual field was obscured by ‘zig-zag’ lines of light resembling fortification spectra during the headaches, which were rated at 5 on a pain scale of 1–10. They lasted almost all day for 3 days, and he had mild photophobia. He had no history of previous headaches, and did not complain of any weakness, paraesthesia or difficulty with swallowing or speaking. He had no visual phenomena without the headaches, which occurred once every 3–4 weeks and were ameliorated but not abolished with non-steroidal anti-inflammatory drugs. There was no family history of migraines. The clinical examination was unremarkable. Magnetic resonance imaging (MRI) examination (Fig. 1), performed in view of the patient's age and new-onset headache, revealed an ill-defined focus, hyperintense on T2-weighted and FLAIR sequences and hypointense on T1-weighted sequence, involving the right dorsal pons adjacent to the periaqueductal grey (PAG) region. Differentials considered at that time included a demyelinating or neoplastic lesion. Electroencephalogram, visual evoked, brainstem auditory and somatosensory evoked studies were unremarkable. Cerebrospinal fluid (CSF) studies including cytology and electrophoresis for oligoclonal bands were unremarkable. Repeat MRI 3 months later did not show any interval change. Biopsy of the lesion was ill-advised in view of its location. He remained well except for mild headaches once every month, associated with fortification spectra, as well as scintillations. MRI was repeated 10 months after first presentation (Fig. 2), revealing progression of the lesion, with involvement of bilateral superior cerebellar peduncles, right middle cerebellar peduncle and the left midbrain. The mass was hyperintense on the T2-weighted sequence and hypointense on the T1-weighted sequence, with heterogeneous enhancement. Magnetic resonance spectroscopy (MRS) demonstrated an elevated choline peak and a depressed N-acetylaspartate (NAA) peak, which suggested a high-grade glioma or lymphoma. He was referred to a neuro-oncologist. Repeat CSF cytology showed atypical lymphocytosis, and he was initially treated for lymphoma of the brainstem. MRI was repeated after completion of treatment, showing further progression. He underwent diagnostic stereotactic biopsy, which was consistent with a malignant glioma.

Axial T2-weighted image demonstrates an ill-defined area of abnormal parenchymal signal (arrowed) associated with minimal mass effect in the dorsal right pons.

Axial T2-weighted image. Follow-up magnetic resonance image 10 months later shows progression of the lesion (arrowed). with extensive abnormal signal hyperintensity involving the dorsal pons, superior and middle cerebellar peduncles, tectum and periaqueductal grey matter.
Discussion
Headaches are common in patients with brain tumours, occurring in 50–60% of patients in Forsyth and Posner's retrospective review (1). Only 17% of these patients matched the classical description of having severe early morning headaches associated with nausea and vomiting (1). In this series, 9% of the patients presented with migrainous headaches. The site of pain in the headaches is known to bear little relation to the location of the tumour (2). Although 44% of patients with brainstem gliomas have been described to have headaches (3), there are few published data on the incidence of migraine headaches in patients with brainstem gliomas.
Our patient's history was consistent with migraine with aura (4), except for his age of onset at 55 and the fact that he had not previously had headaches. These red flags (5) prompted early neuroimaging. The identification of a brainstem lesion in the region of the PAG matter in our patient lends support to its purported role in the pathogenesis of both migraine headaches and visual auras.
Migraines are essentially a neurovascular disorder, with both interrelated neuronal and vascular elements playing important pathophysiological roles (6, 7). Damage to the PAG, which is the centre of one of the most potent antinociceptive neuromodulator systems in the brain, is thought to account for increased central sensitization to pain in migraines (8). This increased excitability of the cell membranes of the cerebral cortex, especially the occipital cortex (8), is fundamental to the brain's susceptibility to migraine attacks.
Visual auras in migraines have been described in the literature for more than a century (9). Twenty per cent of migraineurs describe auras, usually visual (8), which are predominantly scintillation phenomena (10). The locus of visual auras seen in migraines is believed to lie in the primary visual association cortex (11, 12), and is the result of the cortical spreading depression of Leao. Whether the occipital spreading depression is primary or a result of brainstem activation is not clear. Cortical excitation and subsequent spreading depression are associated with blood flow changes in the brain (13). Functional MRI studies of visually stimulated migraine attacks have shown that following activation, there is spreading neuronal depression accompanied by vasodilation and hyperoxygenation (14), after which there is oligaemia (15). This cortical spreading depression activates the trigeminal nucleus caudalis, a part of the central pathway mediating the pain of migraine (7). Trigeminal afferents innervating meningeal vessels are activated during the migraine attack, with the result that afferents within the ophthalmic branch of the trigeminal nerve release neuropeptides, causing vasodilation, focal neurogenic inflammation and a lowered threshold for the involved trigeminal afferent nerve (16). The trigeminovascular activation, cortical spreading depression and central sensitization are likely to involve glutamatergic mechanisms (17).
It is well established that structures in the brainstem modulate activity within nociceptive pathways (18). These structures include the periaqueductal grey, locus coeruleus and raphe nuclei (19, 20), which have been shown in animal studies to exhibit descending modulatory effects on the trigeminal nociceptive system (21). Brainstem lesions have been described to cause migraines (22, 23). Patients implanted with brainstem electrodes for the treatment of refractory pain have developed migraine-like headaches (24), as have patients with demyelinating lesions in the PAG region (25). Animal studies have shown that the visual cortex receives afferent inputs from the locus coeruleus and dorsal raphe nuclei (26). Likewise, in humans, there are serotonergic (inhibitory) projections from the dorsal raphe nuclei to the brain, including the visual association cortex. Thus, in our patient, it would be reasonable to postulate that the rostral pontine glioma might have disrupted the ascending inhibitory pathways, leading to disinhibition or hyperexcitability of the trigeminocervical system and visual association cortex and thus the development of migraines.
This case highlights the importance of neuroimaging in patients with new-onset migraines in the older patient, as well as illustrating the pivotal role of the brainstem in the pathogenesis of migraine headaches and visual auras.