
Abstract
Headache is common in systemic lupus erythematosus with reported prevalence as high as 70%. The aims of this study were: to estimate the prevalence and types of headache in a sample of patients with systemic lupus erythematosus comparing it with rheumatoid arthritis, to determine clinical and serological associations. Eighty-one systemic lupus erythematosus and 29 rheumatoid arthritis consecutive patients seen in our outpatient clinic were interviewed. Headache was evaluated using the diagnostic criteria proposed by the International Headache Society. Additional evaluations were carried out in the 81 systemic lupus erythematosus patients including depression, disease activity, lupus damage, function disability, quality of life, and severity degree using a validated scales. We analysed the following autoantibodies: anti-double stranded DNA, anti-nucleosomes, anti-histones, anti-ribosomal P, anti-cardiolipin antibodies, anti-β2-glycoprotein-I (GPI), and antinuclear antibodies. Forty-one per cent of systemic lupus erythematosus and 17% of rheumatoid arthritis patients suffered from headache (P = 0.02). No significant difference for any primary headache type between the two groups was found. Frequency of headache types in systemic lupus erythematosus patients was: migraine 24%, tensional-type headache 11%, and mixed headache 5%. In systemic lupus erythematosus patients the risk factors associated with headaches were Raynaud's phenomenon (OR 3.6; 95% CI 1.3-9.5; P = 0.009) and β2GPI antibody positivity (OR 4.5; 95% CI 1.2-16.2; p = 0.016). We conclude that headache is more common in systemic lupus erythematosus than in rheumatoid arthritis patients and was independently associated with Raynaud's phenomenon and β2GP-I antibodies.
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune disease characterized by antibody-production against specific components of the cell, in association with a wide spectrum of clinical features. The most common neuropsychiatric manifestations in SLE include seizures, cognitive dysfunction, psychosis, and headache. The prevalence of neuropsychiatric affection in SLE varies greatly among studies, depending widely on the diagnostic criteria used on each study. Nervous system involvement has been found ranging from 14% to 75% (1, 2). Headache, especially of migraine type, is very common in SLE with reported prevalences as high as 65–70% in some studies (3–5). The impact of migraine on daily life is enormous. The American Migraine Study (6) found that approximately 23 million Americans suffered severe migraine; more than 85% of women and 82% of men with severe migraine had a headache-related disability. This is a chronic disorder that usually accompanies the patient from diagnosis throughout life. The impact of migraine in SLE may be even higher, due to the fact that this disorder seems to be more common in SLE patients than in the general population.
It has not been possible to determine a specific cause for the high prevalence of headache in SLE patients. Some of the proposed theories until now include: SLE central nervous system (CNS)-activity, use of several drugs, such as non steroid-anti-inflammatory (NSAIDS) drugs or prednisone, or the anti-phospholipid syndrome. On the other hand, some authors propose that there is no specific cause of headache in SLE, and that psychosocial factors and the presence of a chronic disease may be responsible for this high prevalence. However, it is still unclear whether headache in general, or only certain types of headache, such as migraine with aura, represents part of the SLE disease spectrum. Indeed, recent publications have questioned whether headache in SLE is actually more prevalent than in the general population and consider that headache may not be part of a nervous disease spectrum (5, 7, 8). Therefore, we decided to estimate the prevalence and types of headache in patients with SLE and to compare it with a group of patients suffering from another chronic and inflammatory disorder, such as rheumatoid arthritis (RA). Additionally, we studied the demographic, clinical and serological factors associated with the presence of headache in patients with SLE.
Patients and methods
This cross-sectional study was performed at the Neurology and Psychiatry Department, and the Immunology and Rheumatology Department of the Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán (INCMNSZ). The study was approved by the local IRB of our institution. Eighty-one SLE patients and 29 RA patients, who fulfilled the diagnostic criteria of the American College of Rheumatology (9, 10), were included in the study.
Patients were approached for consent to participate in our study in a consecutive manner from the Rheumatology outpatient-clinic of the INCMNSZ, where they are periodically followed-up. Through a standardized questionnaire according to the criteria of the International Headache Society (IHS) (11), we evaluated the presence of headache and its subtypes in each patient. The headache test uses 49 questions and allows classification of headache into seven subtypes accepted by the IHS; it assesses the type and frequency of pain medications used for treating headache, the degree of disability that headache produces and includes a small neurological exam to rule out secondary causes (see Appendix). It was previously validated in a healthy Mexican population (unpublished data) and has been used to study the prevalence of headache in Latin American urban communities (12).
Additional evaluations were carried out in the 81 SLE patients. We measured depression with the Beck Depression Inventary (13), which has already been validated in a Mexican population (14). Perception of disease severity with SLE activity was assessed with the Mexican Systemic Lupus Erythematosus Disease Activity Index (MEX-SLEDAI) (15), that is a modified version of the SLEDAI index and has also been previously validated in a Mexican population (15, 16); this index evaluates the activity of several target organs (i.e. neurological and renal disorders) in SLE. Functional disability was measured with the Disability Index of the Health Assessment Questionnaire (HAQ-Di) (17), quality of life with the Arthritis Impact Measurement Scales (AIMS) (18), SLE severity with the Severity of Disease Index in SLE (19), and SLE damage with the SLICC-ACRT Index. Patient's and physician's global assessments were obtained in 0–10 visual analogue scales, in which 10 was the best state. Sociodemographical data, current use of drugs, and clinical data were also obtained. A blood sample was taken from 70 of 81 SLE patients to measure the following autoantibodies by ELISA, according to the manufacturer's recommendations (The Binding Site, Ltd; Birmingham, UK; Orgentec Diagnostika GmbH, Germany): anti-double stranded DNA, anti-nucleosomes, anti-histones, anti-ribosomal P, anti-cardiolipin antibodies, anti-β2-glycoprotein-I (β2GP-I); and anti-nuclear antibodies (ANA’s), by indirect immunofluorescence in Hep-2 cells. Laboratory studies were not performed in 11 other SLE patients because they were from the countryside and refused to return to our laboratory for blood sampling.
Statistical analysis
Analysis of headache questionnaires was carried out blinded to the rheumatological diagnosis. A descriptive analysis was used in accordance with the level of measurement of the variables. Chi square or Fisher's exact tests was used to compare the differences in the prevalence of headache and its subtypes among the patients with SLE and RA. SLE patients were grouped according to the presence or absence of headache to compare the associations between headache and several sociodemographic, clinical and serological variables. Mann–Whitney's or χ2 and Fisher's exact tests were performed to evaluate associations with quantitative and categorical variables, respectively. Laboratory data were analysed as quantitative variables and as categorical (positive or negative tests). Odds ratio (OR) and its 95% confidence intervals (95%CI) were calculated to estimate the degree of associations between the former variables and the presence of headache. Statistical analysis was performed with SPSS v10 for windows.
Results
Prevalence of headache in SLE and RA patients
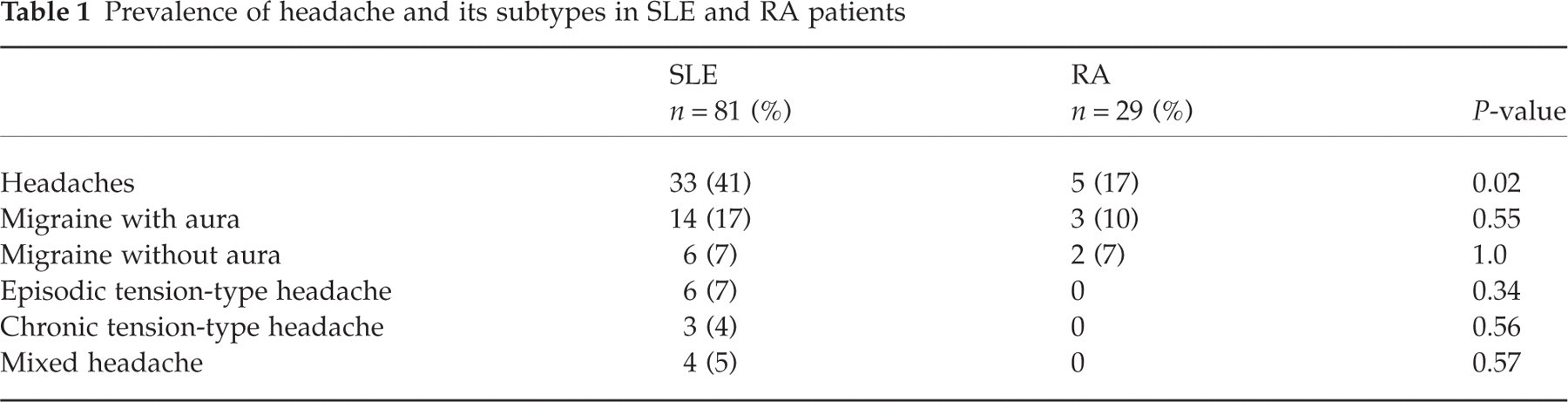
The mean age of the 81 SLE patients was 31.2 ± 9.7 years; 74 (91.4%) patients were female and 7 (8.6%) male. The mean duration of the disease in these patients was 97.0 months (range 6–348 months). On the other hand, the mean age of the 29 RA patients was 45.7 ± 12.6 years; 26 (89.7%) patients were female and 3 (10.3%) male. The mean duration of the rheumatic disease was 162.4 months (range 18–528 months). There was an age difference between our both groups (P = 0.02). Thirty-three (41%) of 81 SLE patients had headache, compared to only 5 (17%) of 29 RA patients, with a statistically significant difference (P = 0.02). Table 1 shows the prevalence of different headache-subtypes in both rheumatological diseases. Migraine was the most common type of headache in SLE patients (24%), especially of migrainous with aura type (17.5%), followed by tensional-type headache (11%) and mixed headache (5%). Among patients with RA, all 5 (17%) patients with headache fulfilled criteria for migraine.
Prevalence of headache and its subtypes in SLE and RA patients
Determinants of headache in patients with SLE
There were not differences with regard to demographic data and other general features according with the presence or absence of headache in SLE patients (Table 2).
Sociodemographic data in patients with SLE according to the presence of headache

N/S, not specified.
Clinical features
Table 3 describes the frequency of clinical manifestations in both groups. Sixteen (48.5%) patients with headache had Raynaud's phenomenon, in comparison with only 10 (20.8%) patients without headache, with an odds ratio of 3.58 (95% CI 1.35–9.49; P = 0.009). Raynaud's phenomenon was similarly associated with both types of headache: migraine (OR 3.8; 95% CI 1.3–10.9; P = 0.01) and tensional type (OR 6.1(95% CI 1.6–22.7; P = 0.01). There were no other significant differences among other studied variables.
Clinical features of SLE patients according to the presence of headache

Values in parentheses represent percentages.
Depression
A score above 13 points in the Beck Depression Inventory test was considered as depression. The average score of the SLE patients with headache was 18.3 ± 13.9 and 12.5 ± 11 in patients without headache (P = 0.004). Seventeen of 33 (51.5%) patients with headache had depression in comparison with 16 (33.3%) of 48 patients without headache (OR = 2.1; 95% CI 0.85–5.2; P = 0.11). A subgroup analysis of migraine and depression revealed that 15 (62.5%) of 24 migraine-suffering patients were depressed, with an estimated association of 3.6 (95% CI 1.3–9.8; P = 0.018). The Beck Depression Inventory average score reached 21.8 ± 14.4 points in migraine patients (P = 0.002).
Rheumatological scales
The results of the different scales (HAQ-Di, AIMS, SEVERITY, SLICC, patient's and physician's global assessment and MEX-SLEDAI.) applied to SLE patients are shown in Table 4. The Patient's global assessment scores were significantly lower in patients with headache (7.1 ± 2.3 vs. 8.0 ± 2.2; P = 0.02). Function (HAQ-Di) and daily activities (AIMS) indexes showed a tendency towards a higher average score in headache sufferers (0.36 ± 0.45 vs. 0.22 ± 0.28; P = 0.065) and (1.06 ± 0.3 vs. 1.18 ± 0.63; P = 0.055), respectively. There were no statistical differences in the SLE activity (MEX-SLEDAI) scores. Function measured with the HAQ-Di also showed a tendency towards a higher score in patients with migraine (0.42 ± 0.51 vs. 0.22 ± 0.29; P = 0.09).
Comparison of the SLE scales according to the presence of headache

Values represent Mean ± SD.
Laboratory data
Table 5 shows that several significant associations among specific antibodies and the presence of headache were found: anti-β2GP-I was observed in 10 (33%) patients with headache and in 4 (10%) patients without headache, with an OR of 4.5 (95% CI 1.25–16.22; P = 0.016). The IgA isotype of the β2GP-I was present in 9 (30%) headache-sufferers, and in 4 (10%) nonheadache sufferers, with an estimated association of 3.86 (95% CI 01.05–14.08; P = 0.033). The grossly speckled pattern of the ANA's was present in 13 headache sufferers (43.3%), and only in 7 (17.5%) patients without headache, with an OR of 3.61 (95% CI 1.08–12.43; P = 0.02).
Association between the presence of antibodies and headache in SLE

Values in parentheses represent percentages.
Drug use
Fifteen (45%) patients with headache were using chloroquine in comparison 10 (21%) patients without headache (OR = 3.17; 95% CI 1.19–8.41; P = 0.02). On the other hand, only one (3%) patient with headache was using hydroxychloroquine, while 10 (21%) patients without headache were taking it (OR 0.12; 95% CI 0.01–0.98; P = 0.022).
Multiple logistic regression
Variables that have statistical significance in the previous analyses were included in a Forward-Wald model (Raynaud's phenomenon, chloroquine, hydroxycloroquine, depression, and anti-β2GPI). Raynaud's phenomenon (P = 0.05) and anti-β2GP-I (P = 0.01) remained independently associated to the presence of headache in SLE patients, whereas hydroxycloroquine use was associated to the absence of headache after controlling with the other variables (P = 0.05).
Discussion
The main finding of the present study is the high frequency of headache in our patients with SLE. The prevalence of headache and migraine in SLE varies greatly among several published studies, mainly due to design problems or to the criteria used to diagnose headache. Since the implementation of the IHS criteria (11), it has been easier to standardize the presence of this common feature in a more accurate manner. Through a Spanish language standardized questionnaire of headache we evaluate the presence of headache and its subtypes in each patient. The headache prevalence around 40% that was found in our SLE patients is similar to other recently published case-control studies (7, 8). In these studies using otherwise healthy subjects as a control group, no statistically significant differences were found between LES patients and controls. Fernández-Nebro et al. (7), reported a headache prevalence of 46.5% in SLE patients and 43.7% in healthy unrelated subjects matched for age and sex. Sfikakis et al. (8) found that the one year prevalence of headache was similar between SLE patients (32%) and otherwise healthy persons (30%) although the overall disease-duration prevalence of headache in SLE was 40% (i.e. patients reporting headache any time since the onset of SLE). Both previous studies concluded that headache in patients with SLE is not significantly related to disease expression or severity. Methodological differences preclude a comparison of our study with these negative studies. Although our headache questionnaire uses 49 questions and allows classifying headache in the seven subtypes accepted by the IHS, a limitation of our headache test is that questions do not distinguish clearly the accompanying symptoms for each separate headache type, in the case that the patient reported more than one headache type (mixed headaches).
An interesting finding of the present study is that the prevalence of headache in patients with SLE (40.7%) was much higher than patients suffering from another chronic and inflammatory disorder (17% in RA patients). Due to the fact that headache, and more specifically migraine, is associated with psychosocial factors, such as depression, or the use of several drugs, such as NSAIDs, and is more common in the female population, we decided to include patients with rheumatoid arthritis as a comparison group. Rheumatoid arthritis is also a chronic inflammatory disorder, it has a gender distribution similar to the one in SLE, and it is also associated with the chronic use of drugs, including NSAIDs. The observation of a high frequency of headache in SLE patients when compared to RA patients allow us to consider that headache in SLE is not related to factors associated to systemic or chronic disease, precipitating headache in susceptible individuals. However, the mean age difference between SLE and RA patients (31.2 ± 9.7 years vs. 45.7 ± 12.6 years; P = 0.02) could explained the higher headache frequency because SLE patients are in the most susceptible range of age for migraine in our general population (between 35 and 45 years).
Among the studied clinical features, we found that Raynaud's phenomenon was associated with headache and migraine, as previously reported (20). This could mean that headache in SLE could have a vascular physiopathological mechanism among other different associated mechanisms. Nevertheless, other studies had not found association between headache and Raynaud's phenomenon in patients with SLE (3, 8, 21, 22). This discrepancy could be related to population or study design differences or to searching intensity considering that prevalence of Raynaud's phenomenon varies with the observer's specific questioning of the patient. We recruited more patients with Raynaud's phenomenon in the current study than the expected prevalence in Mexican patients with SLE (32% vs. 25%) (23), probably because patients were specifically asked about it. On the other hand, psychosocial factors seem to play a role in the prevalence of headache and migraine in SLE. Depression was significantly associated with migraine, which has been previously reported in several studies with healthy subjects (24, 25). In their study Omdal et al. (5) found an association between depression and headache, but they did not find similar results in relation to migraine. On the other hand, Amit et al. (26), found that headache was associated to musculoskeletal and constitutional disease manifestations and was not specific for the diagnosis of serious neurological involvement.
Although the clinical impact of headache was reflected in lower patient's global assessment scores, we did not find association between headache and SLE activity, measured through the MEX-SLEDAI index, in concordance to other studies (5, 26). There was also a lack of association between headache and antiphospholipid antibodies positivity as previously reported (27). However, we found an important association between anti-β2GP-I and headache in SLE, which as far as we know has not been previously reported. This antibody has been associated with typical signs and symptoms of the anti-phospholipid syndrome (arterial or venous thrombosis, thrombocytopenia), and even though it is usually present in patients who fulfil criteria for the anti-phospholipid syndrome, it has also been reported in patients with negative anti-cardiolipin antibodies (28–30). This could be explained by a hypercoagulable state that could be specifically detected through this antibody, and could play a role in the physiopathology of headache in SLE.
Finally, one of the reported adverse effects of chloroquine is transient and mild headache. We found an association between the use of this drug and headache in SLE, while hydroxichloroquine, which is considered to be a less toxic derivative, was associated with a low frequency of headache (OR 0.12; 95% CI 0.014–0.98; P = 0.024). This finding deserves further investigation considering additional information as duration of drug use, doses etc.
Our study suggests that headaches are more frequent in systemic lupus erythematosus than in rheumatoid arthritis patients and independently associated with Raynaud's phenomenon and the presence of anti-β2GP-Ι.
Footnotes
Acknowledgements
The authors thank the Latin American Headache Study Group for allowing us to use the Spanish language standardized questionnaire of headache.