
Abstract
Headache is a common symptom described by patients with systemic lupus erythematosus (SLE). It is uncertain whether both the prevalence and phenotype of headache disorders seen in patients with SLE are similar to those in the general population. The current American College of Rheumatology (ACR) classification of headache disorders includes only five categories, included ‘Intractable headache, non-specific’, which is not further defined. The International Headache Society (IHS) has produced a classification which aims to include all recognized headache disorders. We compared the performance of the IHS and ACR criteria in 61 subjects with SLE. Whereas reference to the IHS criteria enabled classification of all headache disorders seen in the cohort, use of the ACR criteria resulted in failure to classify 22% of headache disorders. We suggest that the ACR criteria require revision. Until this is done, IHS criteria should be used in all future studies of headache in SLE.
Keywords
Introduction
Headache disorders are a common and potentially disabling problem in patients with systemic lupus erythematosus (SLE) (1, 2). Traditionally, headaches have been regarded as a manifestation of SLE and were included in the American College of Rheumatology (ACR) case definitions for the neuropsychiatric (NP) manifestations of SLE in 1999 (3). Although secondary headaches can occur in SLE, for example, as a consequence of cerebral venous sinus thrombosis, the characteristics of the majority of headache disorders described by these patients are indistinguishable from the common primary headache disorders seen in the general population, including migraine and episodic tension-type headache (TTH).
A number of attempts have been made to classify the NP manifestations of SLE, but many have not been adequately validated. The ACR criteria were devised in 1999 by a committee of 35 international experts in the field of SLE and related specialities, including neurology and psychiatry. A summary of the ACR classification for headache disorders is shown in Table 1. The criteria are very limited in scope and detail compared with other classifications such as that of the International Headache Society (HIS) (on which they were loosely based) and may fail to classify certain headache types that occur in patients with SLE. Conversely, cluster headache is included in the ACR criteria despite only a single case report of its occurrence in association with SLE existing in the literature (4). In addition, the ACR term ‘intractable headache’ is not defined, so severely limiting its usefulness.
The American College of Rheumatology classification of headache disorders (1999)

The IHS classification criteria for headache disorders were originally compiled in 1988 (5) and were revised in 2004 (6). They are detailed and exhaustive, and are currently regarded as the gold standard for the purposes of clinical research studies. Included in the classification is ‘Headache attributed to other non-infectious inflammatory disease’ (7.3.3.), where SLE is one of the examples stated. Although no typical characteristics are given, the headache must develop in close temporal relation to the inflammatory disorder and resolve within 3 months after successful treatment. However, defining what constitutes ‘successful treatment’ of SLE is difficult, since many manifestations (including headache) follow a chronic smouldering or episodic course seemingly irrespective of immunosuppressive treatment. Studies that have utilized the IHS classification when determining the prevalence of headache disorders in SLE have found a wide range, from as low as 33% (2) to as high as 78% (7). A recent meta-analysis by Mitsikostas et al. (8) has found that the published data concerning headache disorders in SLE were of poor quality. Most studies were uncontrolled and all were retrospective. Only a minority of studies applied either the ACR or IHS classification. Pooled data showed that 57% of SLE patients reported any type of headache disorder, a similar prevalence to that amongst healthy control subjects. This analysis reported that the prevalence of migraine was 32% and that of TTH was 24%, meaning that headache disorders other than these two are infrequently described in studies of patients with SLE. No evidence for a distinctive form of headache disorder attributable to SLE and no association between headache and SLE disease activity were found. However, the available evidence in this area remains inconclusive. In part, this may reflect uncertainties regarding the performance of available headache classifications such as that of the ACR.
The ability of the IHS and ACR criteria to classify headache disorders occurring in a group of patients with SLE has not been directly compared in the past. The purpose of this study was to make such a comparison between these classifications in order to ascertain the adequacy of the ACR criteria.
Methods
Subjects with SLE were recruited prospectively from a tertiary referral rheumatology centre in Leeds, UK. Subjects were selected randomly from an electronic database that included all patients with SLE who attended the centre for their routine clinical care (approximately 200 patients). The presence of SLE was defined according to standard ACR criteria (9) by an experienced rheumatologist. All subjects were assessed clinically by an experienced neurologist using a set of standardized headache-related questions. The prevalence of each headache disorder was determined with specific reference to the ACR and IHS classifications. The study was granted ethical approval from a local research ethics committee and written consent was obtained from all subjects prior to their participation.
Results
Sixty-one subjects (58 female, three male) with SLE were included. Their mean age was 46.3 years (range 19–72) and mean disease duration was 10.2 years (range 0–32). At the time of study they had moderate disease activity (the median ‘SLE disease activity index’ score was 2) and SLE-related cumulative organ damage (the median ‘Systemic lupus International Collaborating Clinics/ACR damage index’ score was 2). In total, 60 (98%) of subjects described at least one of the ACR-defined NP syndromes, the most prevalent being headache disorders, cognitive dysfunction and mood disorders. Fifty-eight (95%) subjects described a history of a headache disorder, although in three (5%) cases this was inactive (defined as where no episodes of headache had occurred in the preceding year). Twenty-four (39%) subjects with SLE suffered from more than one type of headache disorder. Table 2 shows the prevalence of headache disorders according to the classification criteria used comparing the ACR and IHS classifications. When referring to IHS criteria, classification of all headache types was possible. Using ACR criteria only 78% (63/81) of headache types were classifiable.
Headache disorder prevalence comparing American College of Rheumatology (ACR) and International Headache Society (IHS) classifications
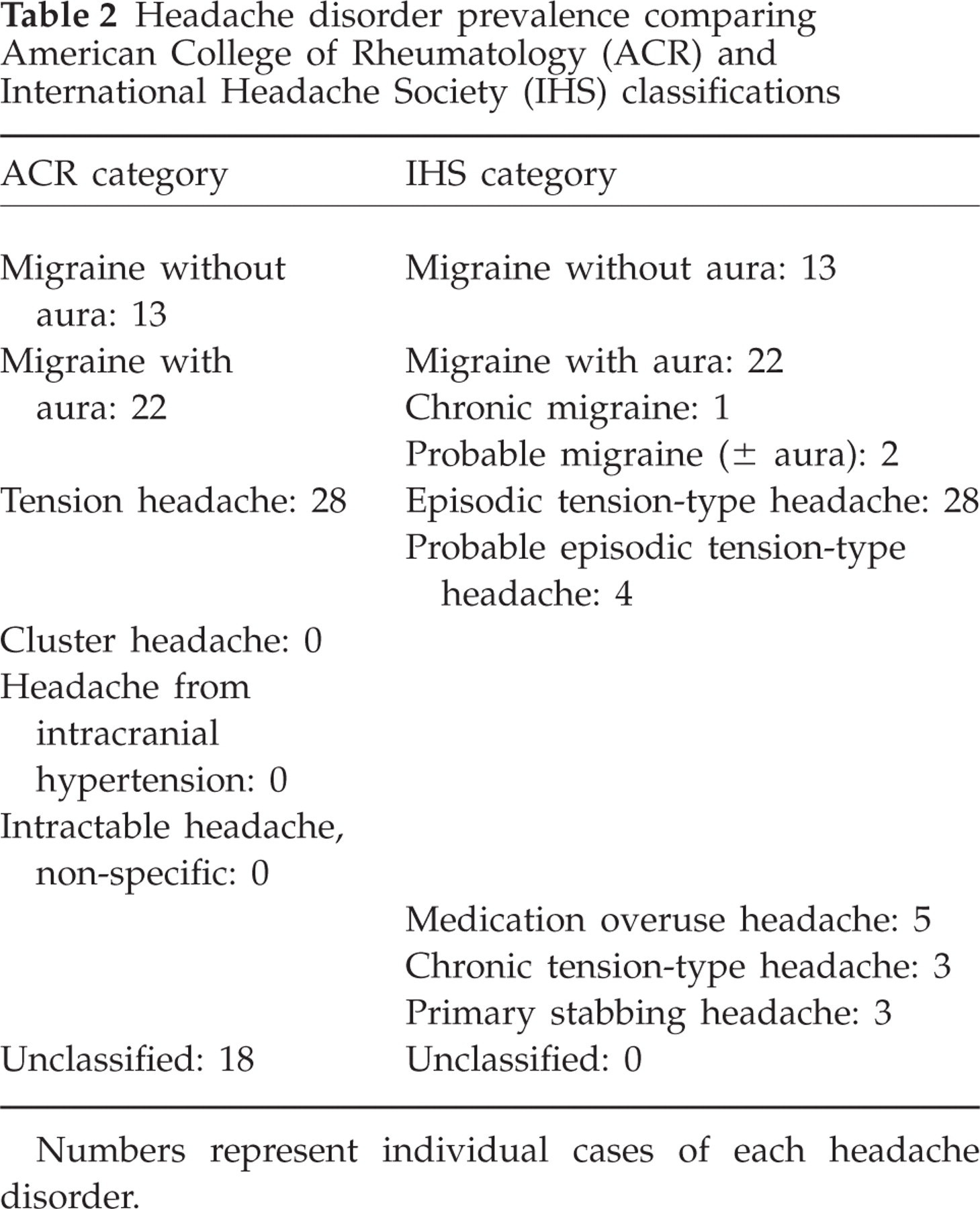
Numbers represent individual cases of each headache disorder.
In general, the headache disorders described by the study subjects were simple to classify using IHS criteria. Three subjects described persistent analgesic-unresponsive headaches which we classified as chronic TTH in two cases and chronic migraine in the other case. No cases of headache fulfilled the IHS classification ‘Headache attributed to other non-infectious inflammatory disease’, primarily due to the lack of an unequivocal relationship between immunosuppressive therapy and headache resolution.
Discussion
All types of headache disorder occurring amongst this cohort of subjects with SLE were classifiable using the IHS criteria. The present study has demonstrated a prevalence of headache disorders in excess of that found by even the highest report in any previous study (7), although many studies did not use the IHS classification. It is possible that selection bias due to recruitment taking place from a tertiary referral centre may have contributed to this high prevalence, although the present study's case mix, including age, gender ratio, SLE disease duration and ethnic mix, was broadly similar to that of other studies. The present study has also documented a greater diversity of headache disorders than in most previous studies. For example, some studies have reported only migraine and TTH (1, 2), whereas another classified three out of 28 headache disorders as ‘non-specific’ (10). Failure to recognize and/or classify rarer headache disorders such as ‘primary stabbing headache’ or to include ‘probable’ cases of migraine and TTH in previous studies may have resulted in lower prevalence rates. In our view, the fact that the assessment and classification in the present study were performed by a physician experienced in the assessment of headache disorders probably contributed to the high prevalence and diversity documented. Despite the high prevalence of migraine with aura in SLE, in general, the aura features described by subjects were not atypical in terms of their distribution (predominantly visual), character or duration. Overall, headaches occurring in the context of SLE seem to have similar features to those seen in the general population (for whom the IHS criteria were devised), but we acknowledge that our study was not designed with the aim of identifying the causality of headache disorders in patients with SLE.
The ACR classification does not contain specific detail regarding whether headache disorders occurring in the context of SLE can be directly attributed to SLE by aetiology, although the aim of the classification was to stimulate research that may aid this distinction. The approach taken in the present study was phenomenological; we did not attempt to describe headache aetiology. Hanly et al. (10) have attempted to infer aetiology of headache disorders to SLE by only attributing the symptoms to SLE if they ‘occurred following the diagnosis of SLE and if no other aetiology could be identified’. Using this methodology, only 10 of 28 headache disorders were attributed to SLE. Similarly, we observed that the onset of the headache disorder often predated SLE diagnosis, in many occasions by a number of years. However, this approach may not necessarily mean that headache disorders that precede the diagnosis of SLE are always an incidental comorbidity, since it is uncertain how long underlying immunological abnormalities that eventually result in a ‘diagnostic’ clinical phenotype of SLE are present before the diagnosis is typically made.
In common with most previous studies, no conclusive evidence for the existence of a distinct phenotype seen only in patients with SLE, such as the ill-defined entity of ‘lupus headache’ (11), was found. Consistent with existing literature, no subjects reported cluster headache. We suggest that the inclusion of cluster headache in the ACR classification is unnecessary. Although no cases of ‘headache from intracranial hypertension’ were found in our cohort, there is rather more evidence supporting the existence of this disorder in the literature than is the case for cluster headache (12). Nevertheless, further research will be required in order to define what proportion of cases of this disorder actually result from cerebral venous sinus thrombosis or some other SLE-related mechanism rather than being idiopathic and (usually) relatively benign.
The majority of headache types that were not classifiable with reference to the ACR criteria were chronic headaches (defined by the IHS as where headache attacks occur on ≥15 days per month for a continuous period of >3 months and with a daily duration of at least 4 h). Since the ACR classification does not explicitly include a category for chronic headache disorders, there is a risk that the category ‘intractable headache’ will be used as a catch-all term to describe a range of chronic headaches which, in fact, fulfil specific IHS criteria such as chronic TTH and medication overuse headache. It is unclear whether the ACR term ‘intractable’ means continuous, or if it could also be applied to chronic intermittent headaches, or whether it requires unresponsiveness to analgesic or prophylactic headache medication. We feel that this term is unhelpful and fails to offer the physician any practical guidance in terms of appropriate investigation and treatment modalities.
The present study has shown that the use of the IHS classification enables more exhaustive classification of headache disorders occurring in patients with SLE to be made than with the ACR classification. The IHS classification is already well-established in the non-SLE headache literature, and, increasingly, is used as the basis for clinical trials of headache treatments. At present, classification of SLE-related headache according to IHS criteria is preferable to that using the ACR classification. Further research is warranted to clarify whether there is an aetiological association between certain headache types (such as migraine with aura) and SLE. Revision of the ACR classification, in particular to define the term ‘intractable headache’ in detail and to remove ‘cluster headache’, is recommended. Given the stated intent of the authors of the ACR classification to do this following any modification of the IHS classification, revision is now overdue.