
Abstract
Despite occasional case reports, the influence of migraine on time perception has not been systematically investigated. We used an experimental technique to study the estimation of auditory duration in 40 migraineurs at different tone intervals in the ms and in the 1-s range and compared their performance with 40 matched normal subjects. With a time awareness questionnaire we also evaluated the subjective experience of elapsing time for long durations involving long-term memory processes. Migraine did not influence temporal judgements in either of the tests, suggesting that migraineurs do not generally over- or underestimate temporal events. The subgroup of migraineurs with a depressive disorder, however, showed a marked speeding up of their internal timekeeping mechanisms, pointing to depression as an important covariable in time perception.
Introduction
Human information processing and motor behaviour evolve over time. Therefore, precise encoding of temporal information has direct perceptual and behavioural relevance. Natural selection has produced suitable and convergent solutions to the problem of temporal coding in human and animal brains (1). These neuronal mechanisms enable conscious temporal tracking of brief events in the millisecond range, but also allow noting of the cyclicity of slower natural phenomena such as the light–dark cycle caused by the earth's rotation.
The representation of time in the central nervous system has not yet been completely clarified. Beside classical structures known to be responsible for periodical biological events (circadian and ultradian rhythms, periodicity of the EEG and many others), such as the brainstem reticular formation, parts of the hypothalamus, the pineal gland and some thalamic nuclei (2), recent studies indicate the importance of the cerebellum, the basal ganglia, other thalamic nuclei and cortical areas of the left hemisphere in timekeeping operations (3–5). Because of the number of structures involved, one might expect that a variety of neurological disorders would affect time perception. Studies of patients with Parkinson's disease (6), cerebellar (7) and cortical (8) lesions have already demonstrated specific temporal abnormalities. While subjects with cerebellar and cortical lesions exhibited inaccurate temporal judgements in both directions (e.g. over- and underestimation of intervals), patients with parkinsonism demonstrated a systematic impairment towards a temporal slowness in both sensory and motor tasks. Levodopa administration can partly counterbalance this phenomenon (6).
Despite the anatomical proximity of many of the above structures to circuits known to be involved in migraine, research on time perception in migraineurs is rare. There are only a few case reports, which anecdotally describe juvenile and adult migraineurs experiencing distortions of elapsing time (9–12). To our knowledge, this issue has never been addressed systematically. From a cognitive point of view, migraine can be regarded as an information-processing disorder, as indicated by psychophysiological experiments (13). One might anticipate that processing of time would be impaired in a manner similar to other senses. Time, however, is a highly complex concept and shows many differences compared with simple information processing as it occurs in visual or auditory channels. Moreover, for some investigators, time perception is not a sensation like vision or hearing, since ‘events are perceivable but time is not’ (14).
The present study was designed to assess perception of time by migraineurs using computerized psychophysical tasks, which require an estimation of the duration of auditory intervals. We focused on brief temporal tone intervals in the range of milliseconds, but also examined longer tone intervals and long timing processes, which involve long-term memory mechanisms. In addition, the effect of a coexisting depression and the influence of sustained attention processes were also examined.
Materials and methods
Subjects
Forty migraineurs (27 females, 13 males, mean age 35.1 years, range 18–57 years) with or without aura (six and 34 subjects, respectively) from the Headache Outpatient Clinic of the Athens Naval Hospital and 40 healthy control subjects (27 females, 13 males, mean age 35.4 years, range 17–60 years) participated in the study. The study was designed on a matched-pairs basis, so that for each migraineur a gender and age (±3 years)-matched healthy subject was chosen. Patients were diagnosed according to the criteria of the International Headache Society (15) by one of the authors (D.D.M. or E.A.). Mean ictal frequency was 3.2 attacks per month for all patients, or 5.8 attacks per month when considering the pretreatment period of those patients who received prophylactic medication. None of the participants had a history of neurological disorder or disease other than migraine. If patients were receiving medication for migraine prophylaxis, the drugs were interrupted at least 14 days before testing. All migraineurs were tested interictally and none of them had an attack in the last 24 h before the experiment. The study was approved by the research ethics board of the Athens Naval Hospital and followed the tenets of the Declaration of Helsinki. After the procedure had been explained all subjects were asked for their consent.
Tasks
Subjects took part in five procedures always applied in the same order.
(1) Main test
The main test was a computerized duration discrimination procedure (16) for brief time intervals in the range of milliseconds. Participants had to decide which of two acoustic stimulus intervals, each marked by two consecutive 5-ms tones, was longer. The presentation of the intervals and the recording of the subjects’ responses were controlled by an IBM-compatible PC. The tones were 1000-Hz sinusoids presented through headphones and the subjects were allowed to adjust the sound intensity to a readily audible and pleasant level, which was well above their hearing threshold. To investigate a possible influence of sound intensity on subjective duration estimation, we conducted pilot experiments with seven subjects by using increasing sound pressure levels, which were well above the minimal audible level and far below uncomfortable loudness. For this limited range of intensities, similar to the one used in the main study, we found no correlation between sound pressure levels and duration judgements for 1-kHz pure tones. However, for very loud (>100 dB SPL) or very quiet (<20 dB SPL) tones a temporal distortion cannot be excluded. During each session subjects were confronted with 300 two-alternative forced choice time judgements. An experimental session consisted of three blocks of 100 trials each with a brief pause between blocks. The first stimulus interval had a constant base duration of 70 ms (base interval, T b). The duration of the second, variable stimulus interval (test interval, T t) was T t = T b + Δi. The difference interval Δi is defined as Δi = (i − 4) × 10, where i = 1, 2, 3, 5, 6, 7, resulting in three variable intervals shorter and three intervals longer than the base duration T b. All possible durations of T t were applied in a pseudorandom order. Subjects sat in a comfortable chair, facing the computer monitor in an empty and quiet room. An experimental block was started by pressing any key on the keyboard. The two intervals, T b and T t, were then presented with an interstimulus interval of 900 ms. By pressing the ‘L’ key or the ‘S’ key, subjects indicated whether T t was longer or shorter than T b. After subjects had responded, visual feedback (‘correct’ or ‘false’) was displayed on the screen. The next trial was applied after 3000 ms. All responses were saved on disc and were used off-line to count the number of false responses. Prior to data collection, subjects had to practice for 3 min, in order to accustom thenselves to the stimulus–response configuration and to ensure that they understood the directions. Practice trials were repeated as necessary until it was clear that each subject was familiar with the task. A schematic presentation of the stimulus paradigm is shown in Fig. 1.
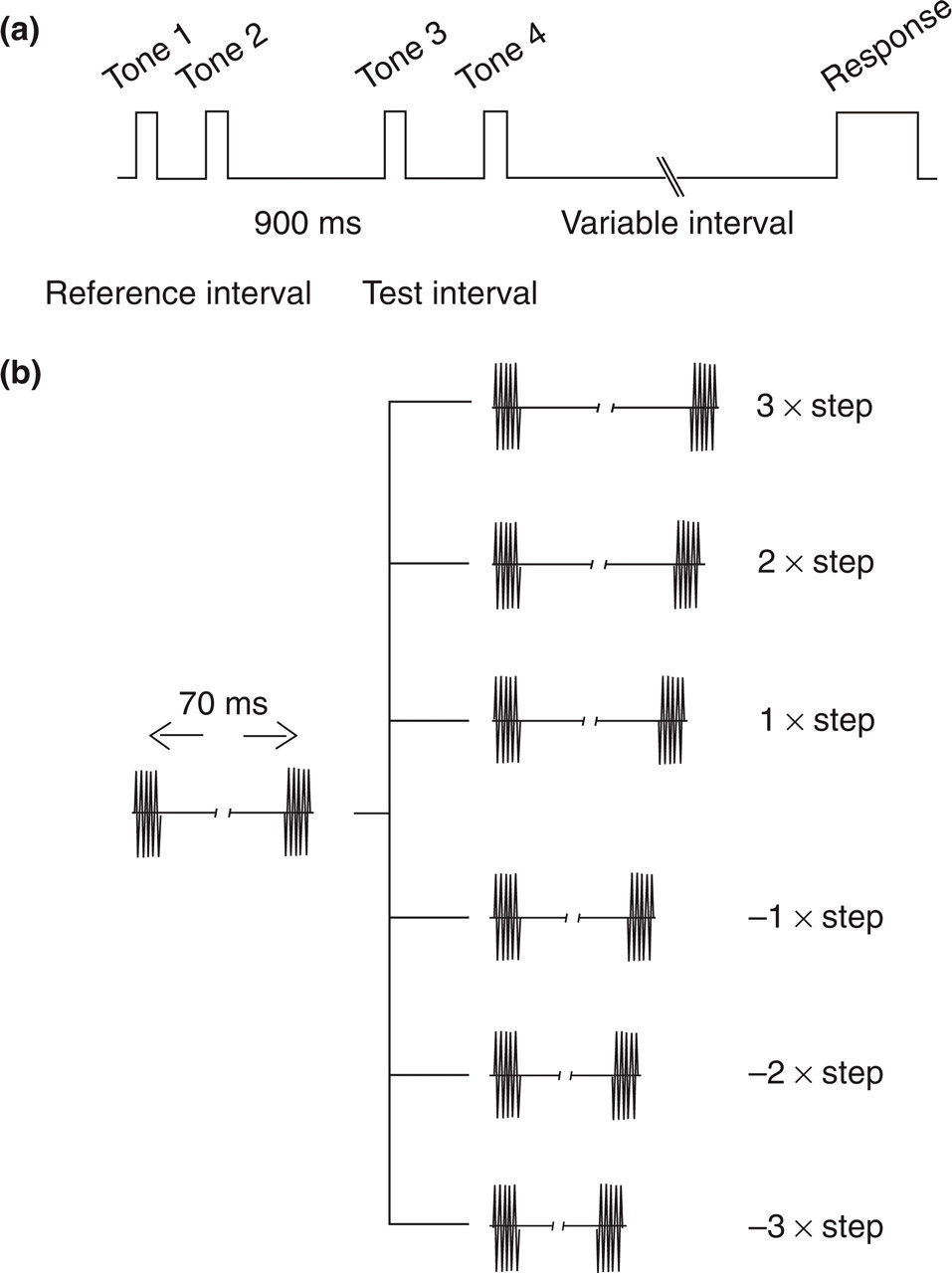
(a) Temporal sequence of events in the main experiment. Two pairs of tones defining the two intervals [reference (T b) and test interval (T t)], followed by the subject's response. (b) The intervals are marked by brief (5 ms) pure sine tones of 1000 Hz. After a reference interval of constant duration there follows a test interval of six alternative durations: three longer and three shorter than the reference interval.
(2) Complementary test
This procedure was included to assess the possible effect of migraine on longer durations in the range of 1 s, since it is assumed that there might be different neuronal mechanisms involved in these longer intervals (4). We used a much simpler method than the one applied in the main experiment, because it was considered important to reduce the total time of the test to prevent the participants suffering fatigue. Subjects were asked to compare various durations (0.25 s, 0.5 s, 1 s, 1.5 s and 2 s) with their own idea of a 1-s duration in a two-alternative (‘this was one second’ vs. ‘this was not one second’) forced-choice procedure according to the technique of Lhamon and Goldstone (17). In pilot experiments, we found that the 0.25-s interval was always identified correctly by the subjects without exception. We therefore excluded this interval from subsequent experiments and used only the four remaining intervals: 0.5 s, 1 s, 1.5 s and 2 s. The sum of all false responses was computed off-line to asses the subjects’ performance.
(3) Test for sustained attention
This test made it possible to investigate the effects of attention on duration estimation, since it is well established that attention constitutes a major factor in interindividual variability in this kind of experiments (18). We used a modified version of the computerized ‘seven-triangle’ test from the Wiener Test Battery. This procedure enables us to assess sustained attention performance, since the subjects try to pick up and count triangles with a particular orientation among seven triangles of equal size presented on a monitor. The seven-triangle set changes automatically every 2 s 150 times. Subjects are asked to respond every time they see three triangles pointing downwards (peak down and base up). The number of correctly identified sets is then computed off-line for each subject.
(4) Time awareness questionnaire
This is a self-rating questionnaire, which gives a less rigid evaluation of time perception than the controlled psychophysical experiments described above. It concerns, however, a different aspect of duration estimation, which focuses on longer intervals and clearly involves other brain functions such as long-term memory. The questionnaire originates from Solomon (1950) and was used by Kitamura and Kumar on depressive subjects (19). It consists of nine situation-dependent questions (‘when I read …’, ‘when I am eating …’, ‘when I am alone …’, ‘when I am with people …’, ‘when I participate in recreational activities …’, ‘when I am busy …’, ‘when I am idle …’, ‘when I walk …’ and ‘when I am judging time in an experiment …’, and one general question ‘I find time passes …’), for each of which only one answer is allowed out of ‘very slowly’ (1 point), ‘slowly’ (2 points), ‘neither slowly nor quickly’ (3 points), ‘quickly’ (4 points) and ‘very quickly’ (5 points). The total score was calculated by dividing the sum of the score for each item by the number of answered questions, so that the possible range of total scores is 1.0–5.0.
(5) Hamilton's Rating Scale for Depression
Due to the high comorbidity of migraine and depression (20), we asked the patients to complete the Hamilton's Rating Scale for Depression (HRSD) (21 items) (21). It is known (22, 23) that depressive disorders can influence time perception, and this could bias the present study towards responses which reflect an overestimation of durations. Therefore, we used the HRSD to define possible subgroups of depressive and non-depressive migraineurs, in order to check for effects attributable to this comorbidity.
Results
Main experiment
The difference in mean performance between migraineurs and controls was not significant (t-test for independent samples, t =−0.127, P > 0.05), since both patients and controls gave approximately 114 false responses out of 300 (Fig. 2).

Cumulative results from the 80 participants (40 migraineurs, 40 controls) of the main experiment. The number of false responses is displayed on the ordinate, the subjects are separated in migraineurs and controls on the abscissa: 1.00 = migraineurs, 2.00 = controls. Means are indicated by horizontal marks.
Cluster analysis in both the migraine and control groups separated two subject populations. The first population (28 subjects, 13 migraineurs and 15 controls) showed a higher performance with a cluster centre at 89.4 false responses, while the second population (52 subjects, 27 migraineurs and 25 controls) had a cluster centre at 127.2 responses. The difference between the high- and the low-performance cluster could not be attributed to factors such as gender, depression (HRSD score) or attention, as revealed by statistical comparisons. Furthermore, migraineurs with and without aura where equally distributed in the two clusters, revealing no relationship between the presence of auras and overall performance. Nevertheless, we observed a tendency for more false responses with increasing age of the subject. This finding, however, did not reach statistical significance.
Separate analysis of each of the six T
t also showed no significant differences between patients and controls (

Results of the main experiment displayed for each of the six test intervals separately. Ordinate: number of false responses; abscissa, subjects separated into migraineurs (1.00) and controls (2.00); and six test intervals, three shorter (−3.00, − 2.00 and −1.00) and three longer (1.00, 2.00 and 3.00), than the test interval. Error bars indicate 1 SD.
We further checked for a general under- or overestimation effect by comparing the summed false judgements of the three longer T
t (i.e. T
t > T
b) with the summed false judgements of the three shorter T
t (i.e. T
t < T
b). Again, the differences between patients and controls failed to reach significance at the 5% level (
The effect of a coexisting depressive disorder was examined by focusing on the depressive migraineurs (14 subjects with a HRSD score > 14) and comparing their performance with that of the non-depressive migraineurs and that of the healthy subjects (none of the controls had a HRSD score > 14). There were no differences between the three groups, either in the mean performance across all intervals (one-way
Complementary experiment
No difference in performance could be found between patients and controls in the summed responses (t-test for independent samples, t = 0.216, P > 0.05) or in the data after categorization according to the four stimulus intervals (

Results of the ‘1-s’ experiment, where subjects were asked to compare various durations, presented through headphones, with their own idea of a 1-s duration. Depressive migraineurs differed from non-depressive migraineurs and controls, in that they overestimated systematically the 0.5-s duration (
Time awareness questionnaire
Both patients and controls produced similar time awareness questionnaire (TAW) scores with values approximating 3.0, indicating that time in general passes neither slowly nor quickly for them (t-test for independent samples, t =−0.500, P > 0.05). As expected, however, TAW scores correlated negatively with the HRSD score (R 2 = 0.269, F = 28.700, P < 0.001), demonstrating the strong relationship between depression and time perception (Fig. 5).

Scores of the time awareness questionnaire (TAW) as a function of the Hamilton's Rating Scale for Depression (HRSD) score for each subject. TAW score > 3.0 means that the time passes quickly, TAW score = 3.0 means that time passes neither slowly nor quickly, and TAW score < 3.0 means that time passes slowly for a particular subject. TAW scores are linearly correlated with HRSD scores [for migraineurs and controls together (thick line): R 2 = 0.269, P < 0.001, f(x) =−0.032x + 3.030]. Thin and dotted lines depict regression lines separately for migraineurs and controls, respectively.
The subgroup of depressive migraineurs, again, favoured answers towards lower TAW scores compared with non-depressive patients and controls (one-way
Sustained attention
A linear correlation was observed between sustained attention performance and temporal performance in the main experiment (R 2 = 0.101, F = 8.790, P < 0.01). No such relationship could be detected in the complementary experiment (R 2 = 0.024, F = 1.930, P > 0.05), emphasizing that the neural mechanisms for short time intervals are not identical to those for longer intervals (Fig. 6).

Correlation of performance in the main experiment and the 1-s experiment with scores in the sustained attention test. Performance in the main experiment (thick line) is linearly correlated with attentional performance (R 2 = 0.101, P < 0.01, f(x) =−3.03x + 147.58). In contrast, performance in the 1-s experiment (thin line) is not correlated with attentional performance.
There were no differences in sustained attention performance between patients and controls, either before (t-test for independent samples, t =−0.152, P > 0.05) or after separate analysis of the depressive migraineurs (one-way
It should be mentioned that consideration of migraineurs with aura (six subjects) in a separate dataset did not reveal any more differences between patients and controls than those mentioned above. The same held true for three subjects who suffered from a migraine attack in the last 48 h (but still more than 24 h previously) before testing: exclusion of these subjects from statistical comparisons provided no further significant findings.
Discussion
It has long been known that migraine involves a dysfunction of information processing that is evident also in the interictal period. This is supported by many electrophysiological observations, which demonstrate prominent interictal abnormalities with a variety of neurophysiological techniques (24, 25). In the present study we investigated whether these changes in information processing described in migraine sufferers also extend to the processing of time. We stimulated our subjects with brief tone intervals, since hearing is the most accurate of the senses in discriminating temporal sequences (26). Both the test for brief durations in the ms range and the test for longer durations in the 1-s range failed to demonstrate any abnormality in temporal acuity attributable to migraine. It was thought necessary to conduct both tests since it is believed that brief intervals are processed by different neuronal structures than longer intervals (4, 27). Elementary functions such as the perception of simultaneity and event succession take place in the subsecond range (18). When durations become longer (range of seconds), other processes become important, which relate to the feeling of nowness, the so called ‘subjective present’ (26). This distinction is supported in the present data by the fact that the sustained attention performance is strongly correlated with temporal performance in the former but not in the latter test. This finding was demonstrated for all participants and was not associated with the presence of migraine. Furthermore, we documented the subjective temporal experience of the subjects by means of the time awareness questionnaire. The results were, again, similar for both migraineurs and controls, indicating that there is no systematical speeding up or slowing down of time estimation related to migraine. Collectively, migraine sufferers did not exhibit any specific abnormal pattern in their perception of the passage of time in any of the three tests applied in this study.
It appears that our data contradict other psychophysical and electrophysiological studies showing altered interictal information processing in many sensory modalities, which are also reflected in late cortical potentials such as the contingent negative variation and the P300 response (13, 24, 25). It should be noted, however, that duration estimation is not analogous to sensations like vision and hearing. Moreover, for some authors time estimation is not an information processing module itself, but rather a prerequisite for information processing (14, 18). This is also supported by the fact that fundamental psychophysical laws that govern all sensory modalities (28), such as the constancy of the Weber-fraction (‘Weber's law’), are not valid in time perception (29, 30). Hence, our results indicate that the substrate of the information-processing deficits prevalent in migraine sufferers is not based on a distorted chronometric mechanism. Indeed, numerous studies suggest that the cause of these interictal sensory impairments might be a lack of habituation to external stimuli, as is indicated by a potentiation of the evoked response amplitudes during stimulation in migraineurs, which is the most reproducible electrophysiological finding so far (24, 25).
Perception of time is intimately related to the affective state (22, 23). Hence, the application of the HRSD was necessary in order to isolate subjects with depression. All control subjects had low HRSD scores, in contrast to a subgroup of migraineurs who showed a depressive disorder. Interestingly, these subjects displayed striking deficits in the ‘1-s’ experiment: short temporal intervals were systematically overestimated, as reflected in the high amount of misjudgements of the ‘0.5-s’ intervals. This is compatible with a pathological speed-up of internal time monitoring processes. That causes subjective slowing at perceiving the passage of time. The same was true for the TAW questionnaire, where depressive subjects produced lower scores, suggesting a link between abnormal mood and slowed time experience. These results corroborate previous work on depressive subjects (19, 22, 23). Contrary to the above data from the ‘1-s’ experiment and the TAW questionnaire, results from the main experiment (ms range) demonstrated equal performance for the depressive migraineurs, non-depressive migraineurs and controls. This, also, highlights the different mechanisms underlying time estimation across different ranges of interval (4, 27).
The main finding of the present study is that the neural abnormalities involved in migraine pathogenesis (31) do not interfere with the mechanisms that mediate time perception. Abnormal time experience in migraineurs might be explained by a coexisting mood disorder. Rare cases of bizarre temporal distortions (9–12) might also reflect the unusual expression of an aura.
It remains to be determined whether temporal judgements are disturbed transiently during a migraine attack. However, this might be difficult to assess with objective computerized procedures, since the severity of the headache will drastically constrain the duration of the experiment, and thus undermine the statistical quality of the results. Furthermore, the high attentional and cognitive engagement required from the participants might also not be feasible in the ictal phase. Hence, an ictal study should probably be limited to a questionnaire evaluation, which is unfortunately flawed by the methodological bias of introspection (32). Nevertheless, a shorter version of the psychophysical tests described here might be applicable during mild attacks, as well as in the prodromal period or just after an attack. This will allow a comparison of ictal or peri-ictal temporal processing with our results. Recent advantages in human electrophysiological techniques might be useful in this direction. Earlier (33) but also very recent (34) studies used tone gaps to assess duration estimation, while recording event-related responses to these stimuli. The latter study demonstrated a robust method for eliciting mismatch negativity potentials evoked by rare tone gaps of varying durations, placed among a series of standard duration tones. These experiments might provide an objective characterization of time processing in migraineurs and might reduce the cognitive effort required from the subjects, since the mismatch negativity is considered to be an automatic response that can be elicited in the absence of conscious attention (35). In this light, new experimental series will be needed to elucidate temporal processing during attacks in migraine as well as in other transient neurological conditions such as cluster headache.