
Abstract
Available studies offer only limited guidance on neuroimaging of non-acute headache patients. The aim of this study was to estimate the frequency of significant intracranial lesions in patients with headache and to determine the clinical variables helpful in identifying patients with intracranial lesions. All patients aged ≥l 15 years attending the Neurology Clinic with non-acute headache were included in the study and followed prospectively. Every patient was investigated by neuroimaging studies, either computed tomography or magnetic resonance imaging. Neuroimaging results were classified as ‘significant abnormalities’, ‘nonsignificant abnormalities’ or ‘normal’. Significant abnormalities included neoplastic disease, hydrocephalus, vascular malformations, Chiari malformation, large arachnoid cysts, intracranial haemorrhage, and acute cerebral infarcts. Consecutive patients (n = 1876; 1243 women and 633 men) were included. Their mean age was 38 years (range 15-95 years). Neuroimaging studies detected significant lesions in 22 patients [1.2%, 95% confidence interval (CI) 0.7, 1.8]. The rate of significant intracranial abnormalities in patients with headache and normal neurological examination was 0.9% (95% CI 0.5, 1.4). The only clinical variable associated with a higher probability of intracranial abnormalities was neurological examination. The proportion of patients with headache and intracranial lesions is relatively small, but neither neurological examination nor the features in the clinical history permit us to rule out such abnormalities.
Introduction
Headache is a common disorder with many potential causes. The lifetime prevalence of all types of headaches varies from 31% to 96% (1, 2). Primary headache disorders, mainly migraine and tension-type headache, account for the majority of headaches. However, many patients and physicians are concerned that an intracranial lesion may be responsible for the headache. The main reason for obtaining a neuroimaging study, whether computed tomography (CT) or magnetic resonance imaging (MRI), is to detect a treatable lesion such as a tumour or a vascular malformation. Neuroimaging may also be helpful to reassure the patient. Medico-legal concerns and the patient's request are other reasons that may also influence the physician's decision to perform a neuroimaging study.
The US Headache Consortium published an evidence-based guideline focused on neuroimaging in patients with non-acute headache (3). The studies identified in the review of the medical literature received a low-quality grade (level IV evidence, in a ranking of I–IV). This guideline concluded that there was not sufficient information to estimate the probability of important intracranial pathology among patients with non-migrainous headache and normal neurological examination, and that comparative studies between MRI and CT were needed in the study of patients with non-acute headache.
The healthcare system in Spain offers neurological care in close vicinity to primary care and free to all the population. Family physicians are responsible for referral of patients to specialized care. A previous epidemiological study in our health area identified 10.6 new patient referrals to the neurologist per 1000 adult population and year (4). Headache was the most frequent reason for referral, occurring in one out of three patients.
The objectives of our study were: (i) to estimate the frequency of significant intracranial lesions in patients with headache evaluated in primary care and referred to the neurologist; (ii) to determine the clinical variables helpful in identifying patients with intracranial lesions.
Patients and methods
The study was performed in two neurology clinics, one located in Aranjuez, a town near Madrid with a population of 85 379, and the other located in Orihuela, with a population of 135 000.
From 2000 to 2002, all patients aged ≥ 15 years attending the Neurology Clinic with non-acute headache as their main symptom were included in the study. Non-acute headache was defined as any type of headache that had begun at least 4 weeks before. Patients with facial pain alone and pregnant women were excluded. Patients with headache were referred by the family physicians working in the health area.
Every patient was examined by one of the staff neurologists and followed up for at least 3 months. The following variables were considered prospectively:
Duration of headache, classified in two groups, < 1 year (new-onset headache), and > 1 year (chronic headache).
Intensity of pain, rated as mild or severe. Headache was considered mild if it was relieved by simple analgesics such as aspirin or acetaminophen, and did not impede the patient's activities, and severe if it was not relieved by simple analgesics, and impeded the patient's activities.
Worsening (increasing frequency or intensity over time) or not.
Sex and age
Type of headache, according to the operational criteria of the International Headache Society (5). When the headache did not clearly fit into a defined type of headache on the first clinical evaluation, it was considered as indeterminate.
Neurological examination, considered as normal or abnormal depending on the presence or absence of neurological signs. Neurological examination was patient-tailored but it included at least the following items: funduscopy, eye fields, pupillary light reaction, eye movements to pursuit on vertical and horizontal gaze, facial sensation and movements, palate and tongue movements, muscle power of arms and legs, reflexes (biceps, triceps, supinator, knee, ankle and plantar), light touch in hand and feet, finger–nose and heel–shin tests, and gait. Mental status examination was performed if the history suggested a disturbance of higher function.
Every patient was investigated by neuroimaging studies, either CT or MRI. The choice between CT and MRI was made on an individual basis depending on factors such as cooperation of the patient, the presence of contraindications to MRI, and waiting lists for the procedures. MRI was performed with 1.5-T imagers. The imaging protocol included standard sagittal and axial T1-weighted and axial T2-weighted imaging with 6-mm section thickness. All CT studies were performed with high-resolution scanners. The slice thickness was 5 mm in the posterior fossa and 10 mm in the supratentorial cavity. The choice of contrast medium was made by the radiologist on an individual basis after reviewing the unenhanced images. The radiologists who performed the evaluation of CT and MRI studies did not access the clinical history of the patients, although they knew their age, sex and the presence of allergies to contrast. Neuroimaging results were classified as ‘significant abnormalities’, ‘non-significant abnormalities’ or ‘normal’. Significant abnormalities included neoplastic disease, hydrocephalus, vascular malformations (aneurysms, arteriovenous malformations, dural fistula, cavernous angiomas), Chiari malformation, large arachnoid cysts, intracranial haemorrhage, and acute cerebral infarcts. MRI was performed after a normal CT if the patient's headache did not respond to treatment. MRI was also performed in most patients with abnormalities on CT to improve their diagnosis.
The clinical variables were considered as screening tests that might predict abnormalities on imaging. The predictive value of the variables was evaluated by means of likelihood ratios (6). A continuous variable, such as age, was compared using Student's unpaired t-test. Confidence intervals were calculated by standard methods.
Results
During the time of the study, 1876 consecutive patients (1243 women and 633 men) were included. Their mean age was 38 years (range 15–95 years). The types of headaches were the following: migraine (49%), tension-type (35.4%), cluster (1.1%), post-traumatic (3.7%) and indeterminate (10.8%). One-third of the patients (629) had new-onset headache while the other two-thirds (1247) had suffered from headache for more than 1 year. Neurological examination was considered normal in most patients (99.2%).
CT scan was done in 1432 patients and MRI in 580; 136 patients underwent both studies. Neuroimaging studies detected significant lesions in 22 patients [1.2%, 95% confidence interval (CI) 0.7, 1.8] (Table 1); neurological examination was normal in 17. The diagnoses in these 17 patients were: pituitary adenoma (n = 3), large arachnoid cyst (n = 2), meningioma (n = 2), hydrocephalus (n = 2), Chiari type I malformation, ischaemic stroke, cavernous angioma, arteriovenous malformation, low-grade astrocytoma, brain stem glioma, colloid cyst, posterior fossa papilloma. Of these 17 patients, eight were treated surgically: hydrocephalus (n = 2), pituitary adenoma, large arachnoid cyst, meningioma, arteriovenous malformation, colloid cyst and papilloma (one of each). The rate of significant intracranial abnormalities in patients with headache and normal neurological examination was 0.9% (95% CI 0.5, 1.4). Neuroimaging studies discovered incidental findings in 14 patients (0.75%, 95% CI 0.4, 1.1):; three pineal cysts, three intracranial lipomas and eight arachnoid cysts.
Patients with non-acute headache and significant abnormalities on computed tomography/magnetic resonance imaging

The yield of neuroimaging studies was higher in the group with indeterminate headache (3.7%) than in the migraine (0.4%) or tension-type headache (0.8%) groups (Table 2). MRI disclosed significant lesions in four of the 444 patients who underwent only MRI (0.9%, 95% CI 0.2, 2.3). CT showed significant lesions in 19 of 1432 patients (1.3%, 95% CI 0.8, 2.1), but one lesion was not confirmed on MRI. MRI was performed in 119 patients with normal CT and it revealed significant lesions in two cases: a small meningioma, and an acoustic neurinoma. Neurological examination in the patient with acoustic neurinoma suggested a posterior fossa lesion.
Rates of significant abnormalities in patients with different types of headache and normal neurological examination

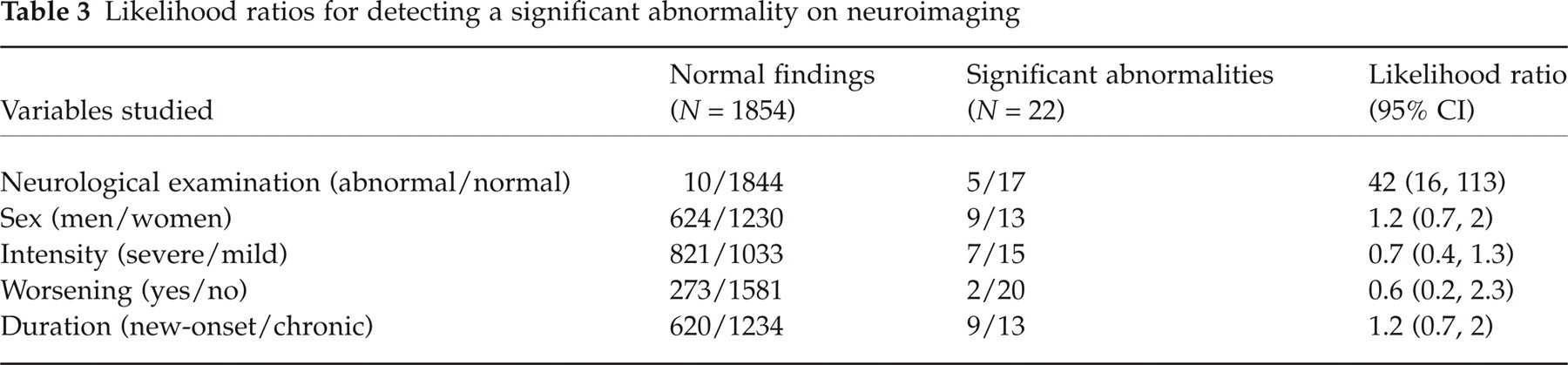
The effectiveness of the clinical evaluation in detecting intracranial abnormalities was evaluated by means of likelihood ratios (Table 3). Neurological examination was the only clinical variable which significantly increased the likelihood of finding a relevant lesion. Mean age was slightly higher among patients with abnormalities on neuroimaging but without statistical significance (age 40.7 vs. 38; P = 0.43). Neurological examination was also helpful in detecting a serious illness even when the neuroimaging studies (CT and MRI) were normal. Three patients with headache were diagnosed with idiopathic intracranial hypertension which was suspected from the presence of bilateral papilloedema in the neurological examination.
Likelihood ratios for detecting a significant abnormality on neuroimaging
Discussion
The appropriate evaluation of the diagnostic utility of neuroimaging studies in headache requires (7): (i) a large number of consecutive patients, representative of the population with this medical problem; (ii) detailed clinical data; (iii) neuroimaging in all patients; and (iv) interpretation of neuroimaging study without knowledge of the clinical data.
All the studies that have analysed the usefulness of neuroimaging in headache had several methodological flaws. The main one is that they included only the patients with headache who were referred for CT or MRI, so there is no information about the patients who were not scanned and the reason for not doing so. Another limitation is a referral bias, since most studies were conducted at tertiary centres, which can overestimate or underestimate the rate of intracranial abnormalities.
The rate of significant intracranial abnormalities in series of patients with chronic headache (not further defined) ranged between 0 and 3%(8–12). However, there is no clear consensus about which abnormalities should be considered ‘significant’. The US Headache Consortium considers as significant those lesions that require further action, such as an acute stroke, neoplastic disease, hydrocephalus or vascular malformations (7). Pineal cysts are considered incidental findings unless they cause aqueductal obstruction with hydrocephalus. Abnormalities of the paranasal sinuses are frequently detected on MRI but they are considered incidental findings unless there is clinical evidence of rhinosinusitis.
We should also take into account that unexpected abnormalities are occasionally discovered during MRI in apparently asymptomatic people. In a series of 1000 paid asymptomatic volunteers with a mean age of 30.6 years, MRI disclosed six relevant lesions (0.6%; 95% CI 0.2, 1.3): aneurysm, cavernous angioma (n = 2) and primary brain neoplasm (n = 3) (13). However, this population cannot be considered representative of the healthy population and may even include patients who simulate healthiness for a free evaluation or for financial gain. Another study determined the prevalence of serious findings unrelated to stroke on MRI in a population of elderly people (14) MRI revealed 41 relevant intracranial lesions among 3672 participants aged 65 and older (1.1%; 95% CI 0.8, 1.5) which included 19 meningiomas, six pituitary adenomas, five cavernous malformations, four aneurysms and seven other findings.
We considered as significant those lesions that would eventually require surgery or another kind of therapy. The finding of a meningioma may not need surgery at the time but it deserves follow-up and may require surgery later on. The yield of neuroimaging studies in patients with non-acute headache in our study was 1.2%. However, since headache is a common medical problem, it is not unusual for physicians to treat patients with headache that harbour potentially relevant intracranial lesions. The question is: are we able to determine clinically the patient who should be scanned and the one who should not?
The first step in the clinical evaluation of a patient with headache is the diagnosis of the clinical type of headache. Migraine and tension-type headaches are the two most common forms in the clinical setting. In our study, 84% of the patients were clinically classified in one of the two groups. In a meta-analysis (3), the estimated prevalence of significant intracranial abnormalities on neuroimaging in patients with migraine and normal neurological examination was 0.2%, with an upper 95% confidence limit of 0.6%. We found four relevant lesions (0.4%), pituitary adenoma, hydrocephalus, arteriovenous malformation, and colloid cyst, among 920 patients with migraine and normal neurological examination.
So far, only two studies, each including fewer than 50 patients, have analysed the prevalence of intracranial lesions in patients with tension-type headache (15, 16). Both studies reported no patient with significant intracranial lesions. In our study, the prevalence of significant intracranial abnormalities on neuroimaging in the group of 665 patients with tension-type headache and normal neurological examination was 0.8%, with an upper 95% confidence limit of 1.7%. There have been several case reports linking cluster headache with intracranial neoplasms (17, 18), but there are no reliable estimates of the prevalence of intracranial abnormalities in patients with cluster headache. We found only one patient with a pituitary adenoma among 20 patients with cluster headache. The type of headache was not clearly determined in 10% of patients at the first visit. The rate of intracranial abnormalities was relatively high in this group (3.7%).
The prevalence of asymptomatic aneurysms with magnetic resonance angiography was 7.0% in a prospective study (19). We did not find any aneurysm among 580 patients who underwent MRI. The detection rate of intracranial saccular aneurysms with MRI was also low in other studies, about 0.1% (13, 14). We foud only one patient with ≥ 5 mm caudal descent of the cerebellar tonsils but the headache was not attributed to Chiari malformation (20). In a retrospective series of 3498 patients with headache, only patient was diagnosed with Chiari type I malformation (21).
Are there any features in the history or physical examination that indicate a higher probability of finding significant abnormalities on scanning? It is generally accepted that some situations raise concerns about a serious organic cause for headaches: new-onset headaches, especially in middle-aged or elderly patients, progressive headaches, headaches that interfere with sleep, and headaches precipitated by exertion, change of position, cough, sneeze, or strain (22, 23). However, the evidence supporting these ‘red flags’ is tenuous. The US Headache Consortium stated that ‘evidence is insufficient to make specific recommendations regarding neuroimaging in the presence or absence of neurological symptoms’ (3). The only variable we found associated with a higher probability of intracranial abnormalities was neurological examination. The likelihood ratio of an abnormal neurological examination was 42. On the other hand, neither severe nor progressive or new-onset headaches were associated with higher rates of significant intracranial lesions.
There are limited data regarding the relative effectiveness of CT and MRI for detecting significant lesions. In our study, among 118 patients with normal neurological examination and normal CT scan, MRI disclosed only one significant lesion, a small meningioma that was not treated surgically.
Overall, the proportion of patients with headache and intracranial lesions is small, but neither the neurological examination nor the features in the clinical history permit us to rule out such abnormalities. Moreover, there are other reasons for neuroimaging, such as reassurance and patient's quality of life. Nowadays, most people with headache demand CT/MRI as an essential part of their medical attention. Investigative tests may produce positive psychological benefits and improve the symptoms of the patients independently of other aspects of management (24, 25). Future studies in the field of neuroimaging in headache should address the impact of these studies on patient satisfaction and quality of life.