
Abstract
The aim of this study was to determine the clinical implications of migraine in systemic lupus erythematosus (SLE) using the cumulative organ damage scores (SLICC-DI). Eighty SLE, 40 rheumatoid arthritis (RA) patients and 40 controls (non SLE, nor RA out-patients), all women, were included. Migraine was defined according to the International Headache Society (IHS) criteria for neuropsychiatric SLE. Disease activity was measured by MEX-SLEDAI and cumulative organ damage by SLICC-DI. Statistics were obtained by Chi-square and Fischer's exact tests. ANOVA was used for comparing means. Migraine was identified in 42.5% of SLE patients, compared to 12.5% of RA patients (P < 0.05) and 10.0% (P < 0.05) in the control group. In the SLE group, a significant association between migraine and Raynaud's phenomenon (P = 0.003, OR = 10.1; 95%CI 2.9-35) and antiphospholipid antibodies (P = 0.0012; OR = 7.5; 95%CI 2.5-22.9) was noted. SLE patients with active migraine had higher MEX-SLEDAI scores than SLE patients without migraine. SLE patients with past history of migraine had significantly higher SLICC scores than SLE patients without migraine. History of migraine was associated with greater organ damage. Active migraine was associated with higher disease activity, antiphospholipid antibodies and worsening of Raynaud's phenomenon. The increased cumulative organ damage in SLE patients with past history of migraine justifies the routine evaluation of migraine in clinical practice.
Introduction
Systemic lupus erythematosus (SLE) is a chronic, inflammatory, immune-mediated disease with diverse clinical manifestations. Central nervous system (CNS) involvement in SLE has been more frequently recognized and reported in recent years, occurring in up to 50% of the patients during the disease course (1). The incidence varies because of the heterogeneity of methods applied and the small number of patients in different studies (2). Several neurological manifestations have been considered to be important features of SLE and indicative of CNS involvement (2–4), but only a few studies (3, 5, 6) included headache as a CNS manifestation.
The exact prevalence of migraine in SLE patients is unknown (7), but several studies published prevalence that varied between 31 and 45% (1, 6–9). The limitations of research in this area are the small sample size, the large variability between study designs and the different classification criteria applied (6).
The clinical importance of migraine has been addressed by several studies (1–7, 10), but the association between migraine and disease activity, antiphospholipid antibodies and Raynaud's phenomenon remains unclear.
Headaches are considered to be associated with a significant source of patient disability (7); therefore the aim of this study was to determine the relation between migraine and cumulative organ damage in a SLE cohort followed prospectively during a one-year period.
Patients and methods
Patients and controls
The frequency of migraine in 80 patients with SLE (11), classified according to the revised criteria of the ACR (12) was compared to that found in 40 controls.
In order to study the relationship between migraine and the chronic conditions of rheumatic diseases, the frequency of migraine in SLE patients was also compared to that found in 40 RA patients (13). All patients and controls were women and were followed up in the outpatient Rheumatology Unit of the State University of Campinas, Brazil, a tertiary reference centre for rheumatic diseases. The control subjects were selected among out-patients women attending other clinics in our hospital and were not related to the RA patients or to other patients with autoimmune diseases.
The patients and controls were examined by the same investigator (SA) on a quarterly basis, during a one-year period. All of the patients and controls signed an informed consent document prior to beginning study procedures.
Exclusion criteria
Migraine has a high rate of familial occurrence, suggesting an underlying genetic factor. In order to determine if SLE influences the occurrence of migraine, patients and controls with a family history of migraine were excluded from this study. Patients with history of migraine prior to diagnosis of rheumatic disease, suggesting that migraine and SLE or RA were coexisting conditions, were also excluded. Patients with headache secondary to infection, hypertension, uraemia, metabolic disorders, lesions or traction of intra- and extra-cranial structures were excluded through history, clinical and laboratorial examinations, performed at every visit. Acute episodes of nonrecurrent headache of very low intensity or frequency were not included in the analysis. As hormonal changes influence the occurrence of migraine, we also excluded postmenopausal women.
Demographic, clinical, serological and treatment features
In SLE patients, constitutional, cutaneous, musculoskeletal, respiratory, cardiac, haematological and renal manifestations of the disease were scrutinized. The diagnosis of Raynaud's phenomenon was based on at least two-phase colour reactions of bilateral distribution described by the patient or observed by a physician. Worsening of Raynaud's phenomenon was defined as worsening of the pain referred by the patient or appearance or worsening of pre-existing digital ulcers. Data on sex, race, age at disease onset and disease duration were collected for each patient. All clinical manifestations and laboratory test findings were recorded. Nephritis was diagnosed on the basis of proteinuria exceeding 1.0 g/l with abnormal urinary sediment and/or histological findings. Nephrotic syndrome was defined as proteinuria in excess of 3.5 g/day. Haematological alterations were ascribed to lupus only in the absence of bone marrow suppression (leucopenia < 4 × 106 cells/l; thrombocytopenia < 100 × 106 cells/l; haemolytic anaemia with positive Coombs test). Antinuclear antibodies (ANA) were determined by indirect immunofluorescence using mouse liver as the substrate and regarded as positive if higher than 1 : 40. Anti-double-stranded DNA (AdsDNA) antibodies were determined by indirect immunofluorescence using Chrithidia as substrate and considered positive if higher than 1 : 10. Precipitating antibodies to extractable nuclear antigens (ENA), including Ro (SSA), La (SSB) and Sm were detected by immunodiffusion and/or microhemagglutination. Anticardiolipin antibodies (aCL) of the IgG and IgM isotypes were measured by the ELISA method as described (14). Lupus anticoagulant (LA) activity was detected by coagulation assays in platelet free plasma obtained by double centrifugation, following the recommendation of the subcommittee on LA of the Scientific and Standardization Committee of the International Society of Thrombosis and Homeostasis (15).
Current treatment options were analysed and changes were made when considered necessary.
RA patients and controls had also a complete clinical examination performed during the visits. Antinuclear antibodies, antiphospholipid antibodies and lupus coagulant were searched in these groups.
Disease activity and cumulative organ damage
At every visit, SLE patients had their systemic disease activity measured by MEX-SLEDAI, a simplified modification of the SLEDAI with a good convergent validity in relation to other disease indexes (16). Patients were considered to have SLE flairs when the MEX-SLEDAI scores were three or more points higher than the previous scores (17). The patients were treated accordingly to their clinical manifestations.
Cumulative SLE-related damage was determined by SLICC-DI (18) in all SLE patients at the beginning and at the end of the study.
Neurological evaluation
A complete neurological examination was performed in all patients and controls during all visits by the same investigator (SA).
Headache
Primary headache syndromes were assessed at every visit according to the criteria of the International Headache Society (19), previously validated in Brazil (20, 21) and also adopted by the ACR (12). As a data-collecting instrument, a form based on one described by Bensenor et al. (22) was used. It followed the IHS diagnostic criteria (19) and was validated for the headache diagnosis.
Patients and controls were encouraged to report current changes in migraine characteristics, such as alterations in frequency, type, intensity and responsiveness to medication.
In order to analyse if migraine was associated with disease flares and SLE related organ damage, we divided patients with migraine in two groups: patients with active migraine and patients with past history of migraine. Patients and controls with migraine according to the IHS (19), but symptom free for a minimum of 12 weeks before the beginning of the study were considered to have past history of migraine. Patients and controls that did not meet these criteria were considered to have active migraine.
Statistics
χ2 analyses and Fischer's exact test were used to compare clinical manifestations and migraine. ANOVA was used to compare means. The Bonferroni inequality was used to adjust the P-values for multiple comparisons.
Results
Demographic characteristics
Eighty SLE patients, 40 RA patients and 40 controls fulfilled the inclusion and exclusion criteria. The strict inclusion and exclusion criteria led to the exclusion of five SLE patients, two RA patients and six controls, prior the study entry.
The SLE and RA patients as well as the controls had similar demographic data (Table 1). The mean age was 32.3 years (range 15–45, standard deviation (SD) 10.9) for SLE, 35.2 years (range 18–47, SD 11.04) for RA and 32.8 years (range 20–48, SD 8.27) for controls. A predominance of Caucasians was observed in all groups. The mean duration of disease was 7.2 years in SLE (range 1–20, SD 5.0) and 8.1 years (range 2–25, SD 6.8) in RA.
Demographic data of the study subjects

SD, standard deviation.
Migraine
Diagnostic criteria for migraine were met in 42.5% of SLE patients compared to 12.5% (P < 0.001) of RA patients and to 10.0% (P < 0.001) of the controls, during the study. Aura was referred by 13 of 34 (38.2%) SLE patients, by 1 of 5 (20.0%) RA patients and by 2 of 4 (50.0%) controls with migraine.
Headache prevention drugs were used by 13 of 34 (38.2%) SLE patients, by 2 of 5 (40.0%) RA patients, and by 2 of 4 (50.0%) controls. At study onset and at visit 1, 23 SLE patients, 3 RA patients and 3 controls were classified as having past history of migraine. At visit two, active migraine was identified in 12 SLE patients, 4 RA patients and 2 controls. At the end of the study, active migraine was identified in 9 SLE patients, 2 RA patients and 1 control.
Clinical, serological and treatment features
In order to search for the association between disease activity and migraine, SLE patients were asked to record recent changes in their symptoms. The most frequent changes observed were greater intensity of pain (37.5%), new episodes of migraine after being on effective therapy for 12 weeks (39.1%) and change in aura characteristics (46.1%).
No difference was noted when we compared the mean MEX-SLEDAI scores of SLE patients during all 3 visits. However, when we compared the mean MEX-SLEDAI scores of patients with active migraine (13.7 ± 2.19) to patients without them (4.6 ± 1.5), at the end of the study, a statistically significant difference was observed (P < 0.001) (Fig. 1).

SLE: MEX-SLEDAI scores in patients with (▪) and without (□) active migraine at the end of the study.
Raynaud's phenomenon was more frequent in SLE patients with active migraine (P < 0.0001, OR = 14.0; 95% CI = 4.2–41.0) (Table 2). Worsening of Raynaud's phenomenon shortly before severe migraine episodes was referred by 44.1% of SLE patients. Eleven of 13 (84.6%) patients with migraine referred worsening of Raynaud's phenomenon during aura.
SLE: Clinical manifestations in patients with and without migraine

∗P < 0.003.
Antiphospholipid antibodies were more frequent in SLE with migraine when compared to SLE without migraine (P < 0.0001; OR = 11.7; 95% CI = 3.7–37.1). No difference between the frequencies of other auto antibodies in these two groups was observed (Table 3).
SLE: Immunological features in patients with and without migraine
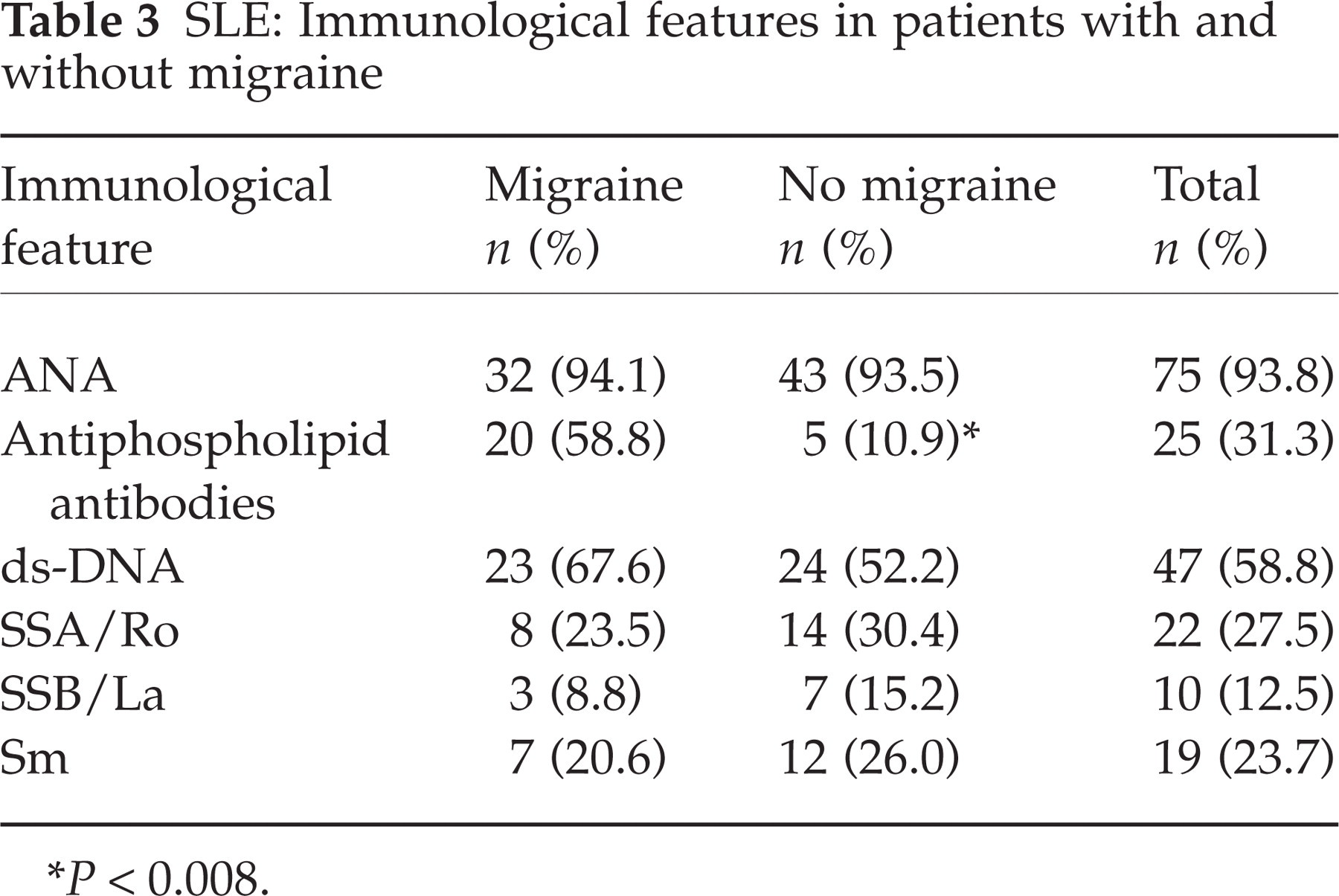
∗P < 0.008.
No difference was noted when mean SLICC scores from SLE patients at the beginning and at the end of the study were compared. However, the mean value of SLICC scores was 4.0 (±2.19) for SLE patients with past history of migraine compared to 0.8 (±0.83) (P < 0.001) for SLE patients without past history of migraine (Fig. 2) at the end of the study. Renal, musculoskeletal and peripheral vascular systems were significantly more frequently affected (P < 0.05) in SLE patients with past history of migraine (Fig. 3).

SLE: SLICC scores in patients with (▪) and without (□) past history of migraine at the end of the study.

SLE: SLICC-DI scores in different organ involvement at the end of the study. Without (▪) and with (□) migraine.
No relation between past or current drug use (corticosteroids, nonsteroid anti-inflammatory drugs or other immunosuppressive drugs) and the incidence of new episodes of migraine was found. Patients, who were treated with corticosteroids or other immunosuppressive drugs for other systemic manifestations of SLE than headache, had a 41.2% improvement in migraine symptoms. No RA patients or control had positive antiphospholipid antibodies or Raynaud's phenomenon.
Neurological evaluation
Neurological examination was normal in all SLE patients and controls during all visits. Twenty (50%) of RA patients presented some degree of muscle atrophy and 5 (12.5%) had gait disturbance, secondary to hip involvement at the beginning and at the end of the study. These abnormalities could be explained by articular sequelae secondary to RA.
Discussion
Although a number of studies analysed the importance of disease activity in migraine (2, 8, 10), no study, to our knowledge, analysed the impact of migraine in SLE using the cumulative organ damage scores. Our study shows that SLE patients with past history of migraine have higher SLICC-DI scores than patients without this manifestation. Although most previous controlled studies (1–7) did not find an association between SLE and migraine, we demonstrate that, patients with active migraine had higher disease activity scores than patients without migraine and were therefore more often treated with corticosteroids to control SLE activity than patients without migraine. Both the chronic use of corticosteroids and the presence of SLE flairs are features associated with greater organ damage in SLE patients.
Headache is a common complaint of the general population, especially among young women and influenced by hormonal and psychosocial factors (23). The epidemiological similarities between SLE and migraine require a control group paired by age and sex, but not related to the patients themselves. In order to analyse all these factors, we included only premenopause women. In addition, the frequency of migraine in SLE was also compared to the frequency of migraine in RA, another chronic rheumatic disease, in order to exclude the assumption that nonspecific factors related to systemic diseases, may act to precipitate migraine in susceptible individuals (24, 25). The increased prevalence of migraine in SLE when compared to RA suggests that the presence of migraine could not be explained solely by the presence of an underlying chronic disease.
There is clinical experimental evidence that extracranial arterial vasodilation, extracranial neurogenic inflammation, and decreased inhibition of central pain transmission are involved in the pathogenesis of the migraine headache (24). Raynaud's phenomenon is frequently observed in patients with migraine in general population surveys (26–28), suggesting that these conditions may share a common pathogenic mechanism, such as similar vascular reactions (26, 27) and vascular endothelial cell dysfunction (29, 30). Proposed mechanisms include antibody-mediated interference with coagulation homeostasis, activation of platelets and endothelial cells and a T-cell immune response to serum phospholipid-binding proteins. Several studies have examined the specific interaction between antiphospholipid antibodies, in especially, antibodies to β2-glycoprotein I and in-vitro endothelial cell function (31–36). The direct binding of β2-glycoprotein I to the endothelial cell surface is facilitated by the constitutive negative charge on the surface of endothelial cells, enhanced surface expression of negatively charged phosphatidylserine during apoptosis (31) and the fact that annexin II acts as a receptor for the binding of β2-glycoprotein I to cultured endothelial cells (32). Thus, antiphospholipid antibody binding to the endothelial cell surface in a β2-glycoprotein-I–dependent manner leads to endothelial cell activation, which is manifested by up regulation of cell surface adhesion molecules and increased secretion of interleukin-6 and prostaglandins (33–36). So they may induce endothelial damage by complement and or antibody dependent cytotoxicity. Endothelial cells are involved in the regulation of many substances that are involved in the pathogenesis of migraine: inactivation of vasoactive substances such as serotonin and bradicynin and production, for example, of endothelin 1 and prosatcycline. Endothelial cell dysfunction is a relevant pathogenic mechanism explaining the interaction between migraine, antiphospholipid antibodies and Raynaud's phenomenon.
Some studies have analysed the associations between migraine and Raynaud's phenomenon in SLE (24, 25, 37, 38). We found not only a higher prevalence of Raynaud's phenomenon in SLE patients with migraine, but also a worsening of Raynaud's phenomenon prior to migraine episodes in 44.1% of our SLE patients. The majority of our patients with aura referred worsening of Raynaud's phenomenon during the aura occurrence, supporting the idea that both conditions may have a common pathogenic mechanism. Several neurological disorders have been associated with the presence of antiphospholipid antibodies (39–42), but there are still controversies in relation to migraine (7, 24, 25, 37, 38). However, the majority of study groups are small, making statistic analysis more difficult. In our study, the presence of antiphospholipid antibodies was more frequent in SLE patients with migraine.
The Rheumatology Unit of the Sate University of Campinas is a reference centre for rheumatic diseases and this fact explains the high frequency of some clinical SLE manifestations, such as nephropathy.
Our study has some limitations. First, this is not an unselected sample of SLE patients. Only women were included in this study because both migraine and SLE have hormonal influence. Second, the number of patients with active migraine is small and no headache diary was used, making difficult to extract conclusion in a prospective manner. Also, the strict inclusion and exclusion criteria used could introduce bias, especially in relation to the number of persons affected by migraine in all three groups. But as the primary objective of our study was to determine the relation of disease activity and cumulative organ damage and migraine in SLE, and not to determine the overall prevalence of migraine in this population, we consider that these limitations were not relevant to determine this issue. Third, no neurological consultation was performed in this study.
In summary, history of migraine was associated with greater organ damage using SLICC-DI. Active migraine was associated with higher disease activity, measured by MEX-SLEDAI, antiphospholipid antibodies and worsening of Raynaud's phenomenon. The increased cumulative organ damage in SLE patients with past history of migraine justifies the routine evaluation of migraine in clinical practice.
Footnotes
Acknowledgements
This work was supported by Fundos Remanescentes da Sociedade Brazileira de Reumatologia and FAPESP (03/01527-0).