
Abstract
The aim of this study was to determine the prevalence and clinical significance of antiphospholipid antibodies (aPL) in children with migraine. The values of anti-cardiolipin (aCL) and antiβ2 glycoprotein I (antiβ2GPI) antibodies were assayed by an ELISA method in 52 children with migraine and 22 children with tension-type headache. The control group consisted of 61 apparently healthy children at regular preventive visits. Two monoclonal β2GPI dependent aCL (HCAL and EY2C9) were used as calibrators. Lupus anticoagulant (LA) was determined by a modified dilute Russell viper venom time test. Persistently positive aPL were observed during the follow-up in 16.3% of children with migraine (9.3% for aCL, 7.0% for antiβ2GPI and 0% for LA) and in 16.7% of children with tension-type headache (11.1% for aCL, 5.6% for antiβ2GPI and 0% for LA). The prevalence of aPL did not differ significantly between patient groups and healthy children. The prevalence of aPL does not appear to be increased in an unselected group of children with migraine, however, the possible role of aPL in individual cases of paediatric migraine can not be excluded.
Introduction
Migraine is the most common cause of severe headache in children and adolescents, resulting in missing schooldays, limitation of daily activities, and deterioration of the quality of life (1–4). The pathophysiology of paediatric migraine is not well understood and has not been extensively studied. In the last decade the neurogenic inflammation hypothesis of migraine headache proposed that the vasodilator peptides released from the activated trigeminal sensory fibres cause abnormal distention of dural vessels and plasma protein extravasation (5, 6). Many mediators have been reported to be capable of activating or sensitizing trigeminal nerves, including capsaicin, bradykinin, tryptase, prostaglandins (PGE2 and PGI2), cytokines(e.g. IL-1β, IL-6, and TNF-α) and nitric oxide. These mediators are released upon activation from different cell types including endothelial cells and perivascular nerve fibres in meningeal tissues. However, despite considerable progress in understanding the molecular and cellular components involved in neurogenic inflammation, the exact mechanisms underlying migraine precipitation remain largely unknown.
In recent years, the possible role of immune mechanisms in the pathogenesis of migraine has been suggested and a growing number of reports have provided information on immune dysfunction in migraine patients (7). One of the most intriguing issues in the immune-pathogenesis of migraine is the association with antiphospholipid antibodies (aPL), which are considered as the most frequent cause of autoimmune thrombosis (8). The presence of anticardiolipin antibodies (aCL) has been investigated in a few cross-sectional studies in children with migraine, however, controversial data have been reported (9, 10).
Recently, the main antigenic target for the aPL has been identified to be β2 glycoprotein I (β2GPI), a phospholipid-binding protein. It has been demonstrated that endothelium-bound β2GPI offers suitable epitopes for circulating aPL, and antibody binding has been shown to induce activation of endothelial cells (11, 12). Moreover, there is experimental evidence that astrocytes, neurones and vascular endothelium can bind purified antiβ2GPI antibodies, which appears to be independent from aCL (13, 14). Altogether, these findings suggest a possible pathogenetic role for antiβ2GPI antibodies even in migraine, by either a direct interaction with neuronal cells or an interaction with brain microvascular endothelial cells.
Immune-mediated mechanisms of neurological complications may be particularly relevant for paediatric population, since the functionally immature central nervous system in children may be more vulnerable to direct effects of aPL. To address the problem of true prevalence of aPL in paediatric migraine, we prospectively followed the values for aCL, antiβ2GPI antibodies and lupus anticoagulant (LA) in a group of children with migraine, and tried to correlate antibody positivity with the disease activity and antinuclear antibody (ANA) status. To our knowledge, there have been no longitudinal studies on aPL in paediatric migraine and no study has addressed the presence of antiβ2GPI antibodies.
Materials and methods
Study design
The design was a prospective longitudinal study of consecutive unselected children with migraine referred to the outpatient clinic of the Department of Child, Adolescent and Developmental Neurology, University Children's Hospital Ljubljana. The presence of aCL, antiβ2GPI antibodies and LA was assessed at two time points: firstly, at study entry and secondly, 3–6 months after the first determination (mean 5.3 months). The study was approved by the Ethics’ Committee of the Slovenian Ministry of Health. Informed consent was obtained from guardians and patients as well when appropriate.
Patients
The study population consisted of 52 children with migraine, 25 boys and 27 girls, mean age 14.2 years (range 10.0–18.0 years). Migraine was classified according to the criteria of the International Headache Society (15). Forty children were classified as having migraine without aura and 12 children migraine with aura. Diagnosis was established on the basis of thorough medical history followed by a complete physical and neurologic examination. Both children and parents completed a detailed structured questionnaire describing features of child's headache (frequency of attacks, duration of attacks, period of observation, pain location, quality of pain, accompanying symptoms, presence of aura) and general health. The disease severity was determined according to the criteria described previously (3), which include headache frequency, intensity and duration. Headache frequency was reported as the average number of attacks that occurred per month during the past 6 months. Only patients suffering from migraine who presented at least two attacks during the last six months were included. The headache assessment questionnaire included also a scale where patients indicated the average intensity of their headaches using a 10-point grading system (10 = most severe pain). The duration of headache pain was referred as the duration of average headache. All patients were included in the study between October 2002 and August 2003. There was no referral bias in the study population, as patients had been referred to our tertiary care department by primary care physicians unaware of the study. Children with recent infection, ascertained autoimmune disease, vasculitis or abnormalities of the coagulation process were excluded. At the time of the study, no patient was receiving preventive therapy for migraine.
The control group comprised 61 apparently healthy children at their routine preventive visits in the community based health centres. The clinical parameters of the control group and the statistical test procedures used to determine the cut-off values have been reported elsewhere (16). In addition, 22 children with tension-type headache (6 boys and 16 girls; mean age 15.3 years, range 11.0–18.0) served as the primary headache control group. Tension-type headache was classified according to the criteria of the International Headache Society (15).
Detection of aCL antibodies
aCL antibodies were detected by a solid-phase enzyme-linked immunosorbent assay (ELISA) as described (16, 17). In brief, microtitre plates (Costar Medium Binding EIA/RIA plates, Costar, Cambridge, MA, USA) were coated with 40 µl/well of cardiolipin (Sigma, St. Louis, MO, USA) in ethanol and allowed to evaporate at 4°C overnight. After incubation with 120 µl/well of 10% fetal bovine serum (Sigma) in phosphate buffered saline, pH 7.4 (FBS-PBS) for 1 h at room temperature (22–26°C) the plates were washed once with 300 µl/well of PBS. Then 100 µl/well of standards and serum samples diluted 1 : 100 in 10% FBS-PBS were applied in duplicate and the plates were incubated for 2.5 h at room temperature. The plates were washed four times with PBS, and 100 µl/well of alkaline phosphatase-conjugated goat antihuman IgG, IgM or IgA (ACSC, Westbury, NY, USA) diluted in 10% FBS-PBS was added. After 1 h of incubation at room temperature, the plates were washed 4 times with PBS and 100 µl/well of p-nitro-phenyl phosphate (Sigma) dissolved at 1 mg/ml in 1 M diethanolamine buffer (pH 9.8) was added. Optical density at 405 nm (OD) was measured first after 10 min and then every 3 min by a Rainbow Spectra Thermo microtitre plate reader (Tecan, Grödig/Salzburg, Austria) vs a reagent blank until optimal fitting to predicted OD of standards was obtained.
Detection of antiβ2GPI antibodies
Anti-β2GPI antibodies were detected by a solid-phase assay, as described recently (16, 17) and evaluated through the European Forum for aPL (18). In brief, microtitre plates (Costar High Binding EIA/RIA plates) were coated with 50 µl/well of β2GPI dissolved at 10 µg/ml in PBS for 2 h at room temperature. After one washing with 200 µl of PBS containing 0.05% Tween 20 (PBS-Tween), 50 µl/well of standards and serum samples diluted 1 : 100 in PBS-Tween were applied in duplicate and incubated for 30 min at room temperature. After 4 washes, 50 µl/well of alkaline phosphatase-conjugated goat antihuman IgG, IgM or IgA (ACSC) diluted in PBS was added. After 30 min of incubation at room temperature and 4 washes, 100 µl/well of substrate was added. OD was measured as described for aCL ELISA.
Monoclonal antibodies
Two monoclonal β2GPI-dependent aCL were used as calibrators:
the chimeric IgG monoclonal antibody HCAL, consisting of human κ and γ1 constant regions and variable regions from the mouse monoclonal β2GPI-dependent aCL WBCAL-1 (19);
the IgM monoclonal antibody EY2C9, derived from a patient with antiphospholipid syndrome (20).
Calibrations according to original KAPS standards (21) and calibrations according to monoclonal antibodies were performed simultaneously in the same plates as the tested sera, to allow more accurate comparisons. The cut-off points for IgG and IgM aCL in children were 13.5 ng/ml HCAL and 36.9 ng/ml EY2C9, and the cut-off points for IgG and IgM antiβ2GPI antibodies were 3.2 ng/ml HCAL and 13.1 ng/ml EY2C9, respectively (16). Monoclonal antibodies for IgA aCL and antiβ2GPI antibodies were not available; therefore the cut-off points for IgA isotype were determined based on the absorbance values of control healthy children (16).
Detection of lupus anticoagulant
The LA was detected by coagulation assays, following the guidelines of the International Society on Thrombosis and Haemostasis (22). Prolonged phospholipid-dependent coagulation was first demonstrated with activated partial thromboplastin time test (aPTT) and a modified dilute Russell viper venom time test (dRVVT), as previously described (17). LA activity was confirmed by a confirmatory test in which the dRVVT-confirm reagent (LA-Confirm, Gradipore, Sydney, Australia) contained excess phospholipids to neutralize the LA effect. Tests were also performed in mixtures with pooled normal plasma to exclude factor II, V and X deficiencies.
Antinuclear antibodies (ANA)
ANA were determined using a standard indirect immunofluorescence technique on Hep-2 cells (Immuno concepts, Sacramento, CA, USA). ANA serum titres at > 1 : 40 were considered positive. Antibodies against extractable nuclear antigens (anti-ENA) were detected by counterimmunoelectrophoresis in agarose, as previously described (23).
Statistical analysis
Statistical tests were performed using subroutines from the statistical analysis package by MS Excel 6.0 for Windows. χ2 test, t-test assuming equal or unequal variances and linear regression analysis were used when appropriate. Differences were considered statistically significant when P < 0.05.
Results
Headache parameters
A total of 52 children with migraine were enrolled in this prospective study. Patient and headache characteristics at the time of the first serum collection are shown in Table 1.
Patient and headache characteristics at the time of the first serum collection

†values shown as mean ± 2 SD.
Initial aPL determinations
The overall aPL positivity (aCL, antiβ2GPI and LA) at the time of the first serum collection in all patients studied is shown in Table 2. The difference in aPL frequency between the two migraine subtypes was not statistically significant (P > 0.44). A total of 13/52 (25.0%) patients with migraine (groups without and with aura combined) had positive values for aPL. Anticardiolipin antibodies were found in 7 (13.5%), antiβ2GPI in 4 (7.7%), and LA in 3 (5.8%) patients with migraine. Of the 7 patients with migraine who were positive for aCL, 4 had low positive values of IgG aCL (one was positive for both IgG and IgM isotypes) and three patients had a moderate-titre of IgG aCL below 47 ng/ml HCAL (58 GPL). One patient had IgG antiβ2GPI, two IgA antiβ2GPI, and one patient had both IgG and IgA isotypes of antiβ2GPI antibodies. The quantitative expression of IgG antiβ2GPI was low, being generally below 55 ng/ml HCAL. Of note, only one patient with migraine was simultaneously positive for both aCL and antiβ2GPI.
The overall antiphospholipid antibodies positivity at the time of the first serum collection in all patients studied
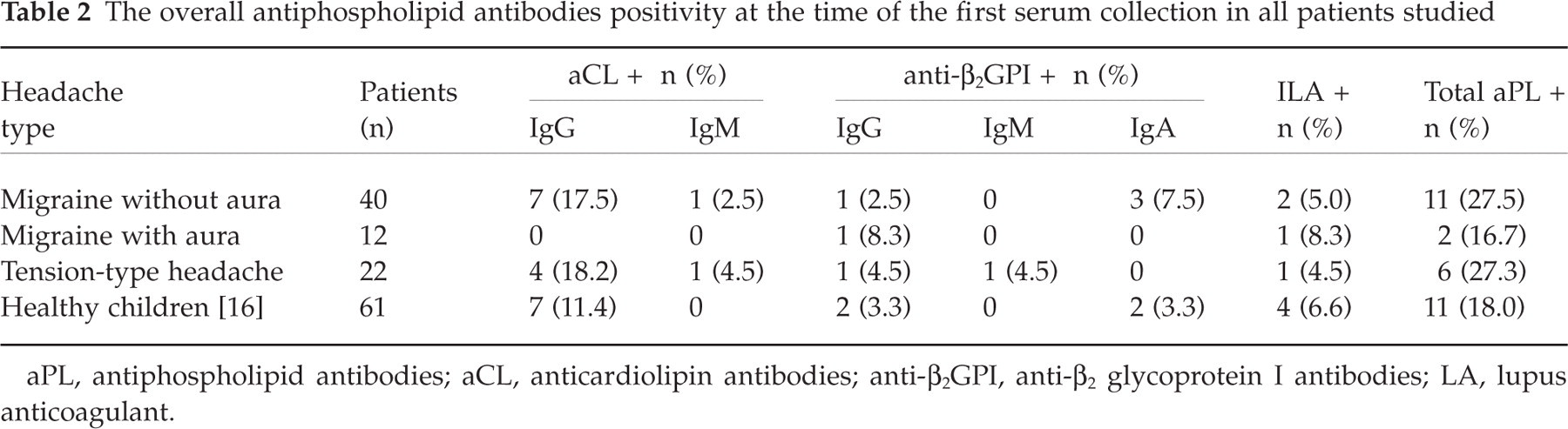
aPL, antiphospholipid antibodies; aCL, anticardiolipin antibodies; anti-β2GPI, anti-β2 glycoprotein I antibodies; LA, lupus anticoagulant.
The frequency of positive aPL was slightly higher in patients with migraine than in apparently healthy children, however, the difference did not reach statistical significance for either aPL subtype. In addition, there were no statistically significant differences in aPL frequency rates between patients with tension-type headache and patients with migraine or apparently healthy children (P > 0.8 and P > 0.5, respectively). Among 5 aCL positive patients with tension-type headache, 4 had low positive values for either IgG or IgM aCL, and only one had moderately elevated IgG aCL (37 ng/ml HCAL or 39 GPL). Anti-β2GPI antibodies were positive in two patients with tension-type headache. One boy had positive IgG antiβ2GPI (18 ng/ml HCAL) and one girl had positive IgM antiβ2GPI (143 ng/ml EY2C9). Both of the antiβ2GPI positive patients with tension-type headache were simultaneously positive also for aCL.
Follow-up aPL determinations
Follow-up sera were available from 43 patients with migraine (32 without aura and 11 with aura) and 18 patients with tension-type headache. Persistently positive aPL were observed during the follow-up in 7/43 patients with migraine (16.3%) (Fig. 1). Four of them (9.3%) were positive for IgG aCL and 3 patients (7.0%) were positive for either IgG or IgA antiβ2GPI antibodies. None of the patients with migraine were persistently positive for LA or displayed persistent positivity for more than one subtype of aPL. Two patients with persistently positive IgG aCL had moderately elevated levels below 47 ng/ml HCAL (58 GPL), while other two patients exhibited low levels of IgG aCL. Two girls with particularly severe form of migraine with high frequency of attacks (once a week) and severe pain(10 points on the grading scale) displayed persistent IgG antiβ2GPI positivity in the range between 42 ng/ml HCAL (48 GPL) and 66 ng/ml HCAL (102 GPL). None of these patients had evidence of aPL-related clinical manifestations.

Prevalence of antiphospholipid antibodies (aPL) in children with migraine and in children with tension-type headache who had persistently positive anticardiolipin (aCL □), antiβ2 glycoprotein I (antiβ2GPI ░) antibodies or lupus anticoagulant (LA ▪). ∗Frequency of aPL in apparently healthy children was determined in a cross-sectional study published elsewhere (16).
Transient positivity of aPL was detected in 9/43 patients with migraine (20.9%). Six of these patients were initially positive and later negative for aPL (4 for IgG aCL and 2 for LA), and three were initially negative and later positive for aPL (two for IgG aCL and one for LA).
Among the patients with tension-type headache, persistently positive aPL were observed during the follow-up in 3/18 (16.7%). Two of them (11.1%) were low positive for IgG aCL and one patient (5.6%) was low positive for IgG antiβ2GPI. Three of 18 patients with tension-type headache were classified as transiently positive for aPL (16.7%). Two of them were initially positive and later negative for aPL (one for IgM aCL and one for LA), and one was initially negative and later positive for IgG antiβ2GPI.
The prevalence of persistently positive aPL was compared between patients with migraine, patients with tension-type headache and the frequency of aPL in apparently healthy children and no significant differences were observed. None of the patients with migraine were persistently positive for ANA or anti-ENA antibodies and only one patient with tension-type headache exhibited persistent ANA positivity with titre at 1 : 80. No significant correlations were found between aPL positivity and the presence of ANA, anti-ENA antibodies or disease activity.
Discussion
Antiphospholipid antibodies have been associated with a variety of neurological manifestations. Some, such as stroke and chorea, are clearly associated with raised aPL whilst others are less well established, e.g. migraine and seizures. Epidemiological studies have shown that teenage migraine is a risk factor for ischaemic stroke in young people (24, 25), however, it is still not clear if this relationship is associated in part with the presence of aPL.
In the present study, the values of aCL, antiβ2GPI antibodies and LA were prospectively followed in 43 children with migraine and 18 children with tension-type headache. According to our results, the estimated prevalence of aPL in children with migraine is 16.3% (9.3% for aCL, 7.0% for antiβ2GPI, 0% for LA) and in children with tension-type headache 16.7% (11.1% for aCL, 5.6% for antiβ2GPI, 0% for LA). Our results show that the prevalence of aPL in children with migraine or tension-type headache is similar to the frequency of aPL observed in healthy children (16). These findings do not indicate a role of aPL in the pathogenesis of teenage migraine, nor do they support the role of aPL in the disease activity.
Published clinical studies on aPL in children with migraine have yielded conflicting results for aCL and have not addressed the question of the presence of antiβ2GPI antibodies. In a cross-sectional study performed by Verrotti et al. (10) aCL were observed in 10% (2/22) of children suffering from migraine with and without aura and in 11% (2/18) of children with complicated migraine. Compared with healthy controls, no increase in frequency of aCL positivity in children with migraine was found. In contrast, Angelini et al. (9) reported positive aCL in 6 (35.3%) out of 17 children suffering from migraine with aura (9). The patients enrolled in this study were highly selected, since only cryptogenic neurological conditions (e.g. migraine with aura) were investigated. In a large study in the adult population, Tietjen et al. (26) found that aCL were not associated with migraine with aura or without aura.
To our knowledge, the present study was the first in which the values for IgG/IgM aCL and antiβ2GPI antibodies in children with migraine were expressed in concentrations of monoclonal antibodies, which allow straightforward comparisons between different laboratories using the same detection method.
It is worth noting that during the follow-up two of our patients with migraine persistently exhibited a moderate titre of IgG aCL, fulfilling the laboratory criteria for antiphospholipid syndrome (APS). Moreover, two girls with particularly severe form of migraine displayed persistent IgG antiβ2GPI positivity. According to these findings, it can be hypothesized that aPL may have an important role in isolated cases of teenage migraine, representing only a small proportion of all children with migraine. Since migraine is the most common cause of headache affecting more than 10% of children and adolescents, it is likely that the small subset of patients with aPL-related migraine would not be recognized in a smaller study; a longer follow-up of a larger series of patients seems necessary to confirm this hypothesis.
To provide an additional illustration of the possible role of aPL in individual cases of paediatric migraine, we report a clinical case of a teenage boy with severe migraine who was found to have persistently moderately elevated levels of IgG aCL. No prophylactic treatment was administered and at the age of 14 years he suddenly developed thrombosis in the left posterior tibial artery therefore fulfilling clinical and laboratory criteria for APS. After commencing antithrombotic therapy, the number of his migraine attacks dramatically decreased, similarly as has already been documented in few adult APS patients (27).
In summary, according to our results the prevalence of aPL does not appear to be increased in an unselected group of children with migraine. However, we found two children with severe migraine and persistently positive aPL, which seems to suggest a relationship between aPL and individual cases of paediatric migraine. Although at present there is no justification to evaluate all children with migraine for aPL, we do believe that determination of aPL may provide clinically relevant information in difficult cases of paediatric migraine(e.g. children with frequent and very intense headaches).
Footnotes
Acknowledgements
We wish to thank Professor Takao Koike (Hokkaido University School of Medicine, Sapporo, Japan) for kindly providing the monoclonal antibodies HCAL and EY2C9, and Dr Andrej Mlakar (General Hospital Celje, Slovenia) for his help in collecting patient's data.