
Abstract
We performed the Queckenstedt's (Q)-test (compression over bilateral internal jugular veins) and a sham test on 33 patients with migraine attacks (coded as 1.1 based on headache classification proposed by International Headache Society (IHS)), 15 with migrainous attacks (IHS code 1.7), and 15 with tension-type headache (IHS code 2.1) in both supine and sitting positions. ‘Migrainous headache‘ (code 1.7) was defined if the headache characteristics fulfilled all but one criteria for ‘migraine without aura’. Migraine sufferers reported a marked increase in headache intensity after a 30-second Q-test in both supine and sitting positions. Aggravation was greater in the supine position. The intensity increase was not demonstrated in the sham test, or in patients with migrainous attacks or tensiontype headaches after the Q-test. Patients with acute migraine thus appear more sensitive to increased cerebral venous pressure or intracranial pressure. The discrepancy of intensity changes between supine and sitting positions may reflect different amount of venous return through the internal jugular veins.
Introduction
Migraine pain is likely related to neurogenic inflammation, as the site of inflammation is at the postcapillary venules (1, 2). This trigeminovascular system can be activated by mechanical or electrical stimulation of the superior sagittal sinus in animal models (3–5). The popular and effective antimigraine drugs dihydroergotamine, ergotamine and sumatritpan are also vasoconstrictors (6, 7). These observations might suggest a possible link between the cephalic venous system and migraine pathophysiology.
Queckenstedt's test (Q-test) determines whether there is a blockage of the spinal canal by briefly compressing the bilateral internal jugular veins, which obstructs the venous return from the head and increases the intracranial and intracranial venous pressures (8). Dauggard et al. (9) observed no significant change in headache intensities when they tried to increase migraine pain during acute attacks in sitting patients by use of the Q-test, which they interpreted as evidence against the involvement of the cephalic venous system or neurogenic inflammation with migraines. However, the subsequent demonstration that the internal jugular veins are in fact collapsed in the sitting position led to the suggestion that performing the Q-test in the sitting position might not be able to induce ‘sufficient’ cephalic venous congestion. Use of the Q-test on acute migraine sufferers in both sitting and lying positions (10) documented a marked severity in pain intensity in the supine position. While these observations support a possible role for cephalic venous congestion in the generation of migraine pain, a definitive conclusion was impossible, as only patients with acute migraine attacks were recruited, and the investigators did not compare the Q-test with placebo maneuvers.
To further determine if the effect of the Q-test on migraine headaches can be extended to other types of headaches, we performed the Q-test on patients with acute headache attacks that included migraine, migrainous, and tension-type headache. A sham placebo maneuver was included in the protocol.
Subjects and methods
The study was designed to evaluate the difference of the change of headache intensity between the jugular vein compression (Q-test) and a sham (placebo) procedure in different headache types during acute attacks. Patients who were visiting the Neurology Outpatient Clinic at the I-Lan General Hospital, I-Lan, Taiwan and currently experiencing a headache attacks were recruited into the study. This pattern of the use of a local clinic for relief of acute pain is similar to the urgent care in the United States.
The study protocol was approved by the Institution Review Board of the Taipei Veterans General Hospital. All patients provided their written informed consent of participation.
The patients were examined at Neurology Outpatient Clinic during the acute headache attacks. Acute headache characteristics as well as previous headache history including pain location, pattern, intensity, and accompanying symptoms were recorded. Patients who had a new onset headache of unknown aetiology or who had treated their acute headache attacks in the preceding 12 h with medications such as ergotamine, sumatriptan, nonsteroidal anti-inflammatory agents or simple analgesics were excluded.
Diagnosis of acute headache attacks
Acute headache attacks were classified according to the diagnostic criteria of the International Headache Society (IHS) criteria (11). Migraine attacks (IHS code 1.1) were characterized by the presence of at least two of the following four criteria: unilateral location, pulsating quality, moderate or severe intensity, and aggravation by physical activity, and the occurrence of at least one of the following accompanied symptoms: nausea, vomiting, or photo- and phonophobia. ‘Migrainous headache’ (IHS code 1.7) was defined if the headache characteristics fulfilling the diagnostic criteria of ‘migrainous disorder not fulfilling above criteria.’ Tension-type headache (IHS code 2.1) was characterized by at least two of the following pain characteristics: pressing/tightening (nonpulsating) quality, mild or moderate intensity, bilateral location and no aggravation by walking stairs or similar routine physical activity, and by the absence of nausea or vomiting, and photo- and phonophobia.
The diagnoses of the studied headache attacks were based on the headache profile at the time of the clinic visit rather than on their previous headache histories.
Sequence of procedure
The study was single-blind in design; participants did not understand the difference between the Q-test and sham procedure. Participants were asked to rest in the supine position for 30 min in a quiet room. While remaining in the supine position they received either the Q-test or a sham procedure at random for 30 s followed by a relief for 30 s, a sham procedure or the Q-test for another 30 s, then a relief for 30 s. The same order was then carried out in the sitting position. During each manoeuver and relief period, patients rated the headache intensity on a scale from 0 to 10, with 0 corresponding to the absence of pain and 10 corresponding to the worst pain imaginable. This rating was obtained verbally 10, 20 and 30 s after commencement of either compression maneuver or relief period.
Manual compression
The Q-test involved the application of a constant and equal manual pressure on both internal jugular veins near the limb of thyroid cartilage. The sham procedure was done by applying equal manual pressure over the same level as the Q-test at the lateral aspect of the neck but avoiding the internal jugular veins. In this study, all the procedures were performed by CH Chou.
Statistical methods
The headache intensity was treated as a continuous variable. In addition, we arbitrarily categorized the increment of headache intensity (≥2 score in comparison with the baseline score) as ‘headache worsening’ in order to compare with previous studies. The data was analysed using paired t-test and chi-square test. In addition, we also put positions(lying or sitting), headache types (migraine, migrainous attacks, tension-type headache) and time sequence (Q-test for 30 s and relief for 30 s) as factors in a factorial analysis of variance (ANOVA) model to evaluate their contribution to the change of headache intensity. If significant interactions were found among these factors, posthoc ANOVA tests were performed subsequently. The estimated difference of the headache intensity change attributed to the position change and time sequence after the Q-test was also calculated. A P-value of <0.05 was considered statistically significant.
Results
During the study period, 74 patients with acute headache gave their informed consent to participate in the study. However, after 30 minutes’ supine rest, 11 patients reported that they became headache free, and so were excluded from the study analysis. The final study population was comprised of 63 patients (23 males, 40 females, with a mean age of 38.1 ± 18.2). Pertinent demographic data and current headache profiles are shown in Table 1.
Clinical characteristics of different acute headache types and the accompanying symptoms
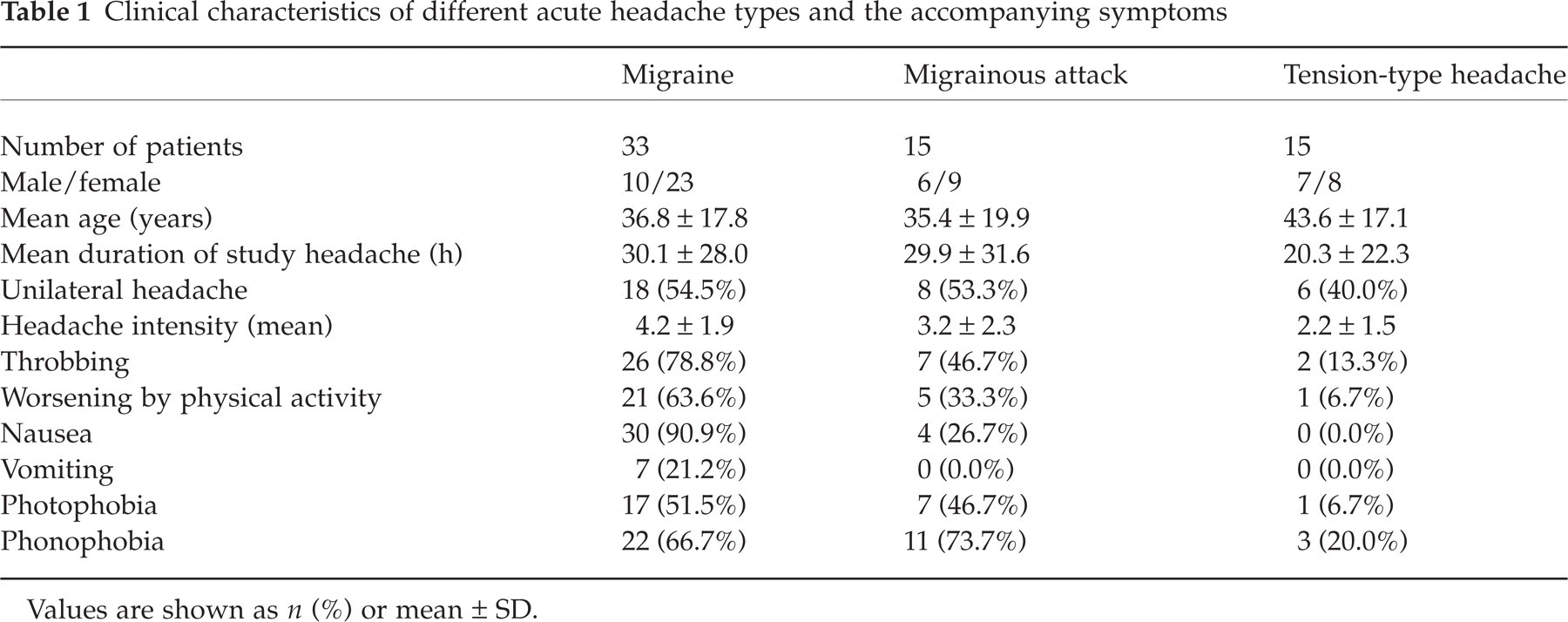
Values are shown as n (%) or mean ± SD.
In patients with migraine attacks, either in the supine or sitting position, the mean headache intensity increased significantly 10 s after commencing the Q-test (P < 0.05). No such increase was evident during the sham procedure. The difference was significant between the Q-test and the sham procedure in patients with migraine (Fig. 1). However, the difference was not found between the Q-test and the sham procedure in patients with migrainous attacks or tension-type headache.

Headache intensity changes in patients with acute migraine by the Q- and sham tests. LQ: lying position with Q-test; SQ: sitting position with Q-test; LS: lying position with sham test; SS: sitting position with sham test.
The verbally offered increment of headache intensity differed in the supine vs. the sitting position, with supine intensity being significantly higher at 10, 20 and 30 s after the Q-test but not during the relief period (paired t-test, all measurements P < 0.05) in patient with migraine (Fig. 2). In patients with migrainous headache or tension-type headache, the mean headache intensity did not increase after either the Q-test or the sham procedure, in both the supine and sitting positions.

Headache intensity changes in patients with acute migraine attacks (M), acute migrainous attacks (M′) and tension-type headaches (T) during (0–30 s) and after (30–60 s) the Q-test (Q). L, lying; S, sitting. †,‡P < 0.05 compared with initial headache intensity after the Q-test, ∗P < 0.05 comparisons between sitting and lying positions.
We calculated the contribution of headache types (migraine, migrainous attacks and tension-type headaches) and positions (lying or sitting) as well as different time point sequences during the Q-test and relief period to variance of the headache intensity change by factorial ANOVA. The analysis showed the significant variables included headache types, time sequence and the interactions between headache types and time sequence (Table 2) Patients with migraine attacks had significantly higher intensity change after the Q-test in comparison with those with migrainous attacks or tension-type headaches. On account of significant interactions, we performed separate posthoc analyses in different headache types and found only in patients with migraine but not the other headache types, did the Q-test induce a significantly higher intensity change in supine positions than in sitting positions, starting at 10 s through 30 s after the Q-test. The estimated difference of headache intensity change in relation to positions and time sequence was shown in Table 3.
The analysis results for factorial analysis of variance (ANOVA) of headache types, positions, and times sequence in relation to headache intensity change after the Q-test

Adjusted r 2 = 0.215; Headache types: migraine, migrainous attack, tension-type headache; Positions: lying vs. sitting positions; Time sequence: every 10 s after the Q-test for 30 s followed by relief for 30 s.
The posthoc analysis results of headache intensity change in relation to different positions and time sequence after the Q-test in patients with migraine

We arbitrarily defined an intensity increment greater than two or more (≥2/10) compared to baseline as ‘worsening’ after the manual procedure. As shown in Table 4, patients with migraine attacks had significantly higher frequencies of headache worsening in both supine and sitting positions in comparison with patients with other headache types.
The number and percentages of patients with headache intensity worsening more than two increments on the assessment scale after administration of the Q-test

In patients with acute migraine and/or migrainous attacks, those who showed headache ‘worsening’ after the 30-second Q-test in the supine position did not differ from those without headache worsening in age, sex, duration of the present acute headache, intensity, presence or absence of pulsatile headache, pain aggravation by physical activities, nausea, vomiting, phonophobia or photophobia (data not shown).
Discussion
The present single-blind study that incorporated a sham test as a placebo and objective reporting of the pain experience offers convincing evidence that the Q-test aggravates acute migraine attacks in both the sitting and supine positions, while the sham test does not. The increment of pain intensity is higher in the supine position. These phenomena are absent in patients with acute ‘migrainous’ attacks or tension-type headache.
In healthy adults, cerebral venous drainage is predominately via the internal jugular veins under the supine position, and in the erect position the major outflow pathway is via the vertebral venous system (12). This supports our finding and those of others (10) that aggravation of pain after the Q-test is more severe in the supine position, and is consistent with the contribution of venous congestion. However, our results differ from Doepp et al. (10) in that we demonstrate headache exacerbation in the sitting position.
In previous studies that employed the sitting position, pain aggravation has been absent (9) or very minimal with trend of significance (6.4 ± 1.4–6.7 ± 1.5, P = 0.05 10). The exact reason for this discrepancy is unknown. The increment of cerebrospinal fluid pressure caused by the Q-test has been measured at about 150 mmH2O (13). However, the cerebrospinal fluid pressure increment is proportional to the magnitude of pressure conducted on the jugular veins (14). The different manual pressures applied in the Q-test by different investigators might contribute to the discrepancy of the results.
The similar pain reporting scales adopted presently and in a prior study (10) have demonstrated a significant or marginally significant increase of pain aggravation. This measurement is more sensitive than ‘worsening’ or ‘better’ to evaluate the change of headache intensity (9). Moreover, the present comparison with a sham test has shown a reliable increment of pain in the sitting position after the Q-test, although the effect size was not as obvious as that displayed in the supine position.
It is of note that our migraine patients had a longer duration of acute headache in comparison with the study of Daugaard et al. (30.1 vs. 4.8 h) (9) We postulate that the chance of ‘central sensitization’ was higher in our study patients, as a consequence of a longer and more intractable headache (15). Therefore, our patients may have been even more sensitive to the change of intravenous or intracranial pressure, even that pressure change inspired by performance of the Q-test in the sitting position.
Among the three different headache types, we found a spectrum of change; the most marked pain exacerbation was found in migraine attacks, followed by migrainous attacks, followed by tension-type headache. The response to the Q-test of migrainous attacks was more similar to tension-type headache than migraine attacks. A recent study that showed a spectrum of headache attacks, ranging from migraine to migrainous headache to tension-type headache in migraineurs were all responsive to sumatriptan (16) supports the continuum model of headache (17), which places tension-type headache, migrainous, and migraine along a spectrum of severity, based upon the existence of a common biological mechanism. However, since many patients with migrainous attacks in the present study were actually migraine sufferers, the migrainous attacks or tension-type headaches (also known as interval headaches or aborted migraine) were possibly different from ‘full blown’ migraine attacks in the underlying pathomechanisms, based on the different response to the Q-test.
Why cephalic venous congestion can exacerbate migraine headaches is still unknown. Some authors suggest that it might be through the influence of venule dilation caused by neurogenic inflammation (2). However, based on the present observations, we propose that increased intracranial pressure may play a role. Aggravation of headache intensity started as early as 10 s after both the Q-test, and improvement was noted within 10 s of commencing the relief period (14). The Q-test can elevate intracranial pressure within seconds, via the increase of intracranial venous pressure, by obstructing the venous return from the head (8). Therefore, it is likely that increased intracranial pressure after the Q-test aggravates migraine pain. Patients with migraine attacks might be more sensitive to increased intracranial pressure than those with migrainous attacks or tension-type headache, although whether the intracranial pressure is higher or not in migraine attack remains unknown. However, the proposed association between migraine attacks and intracranial pressure is supported by our observations that no headache intensity changes on nonmigraine attacks occurred in both sitting and supine positions. Thus, we suggest that intracranial pressure is a more important worsening factor for migraine pain than migrainous attacks or tension-type headache. The sensitivity to the change of intracranial pressure in migraine attacks might be related to the mechanism of ‘central sensitization’. In addition, the difference of pain increase during the Q-test on migraine patients may be related to the collateral cephalic venous flow (18). An individual with prominent vertebral venous system or extrajugular pathways may cause less or no intracranial venous distention on the Q-test, and so may have a less pronounced increase in headache severity.
Conclusions
Cerebral venous congestion plays a role in the aggravation of migraine pain, which is related to body position. This effect is not evident in patients with migrainous attacks or tension-type headaches. A discrepancy of the sensitivity to increased intracranial pressure may exist among different headache types.
Footnotes
Acknowledgements
We thank all the patients who participated in our study, and our assistant Eunice Chung for her help in following up patients and data recording.