
Abstract
Cervicogenic headache is still a controversial disease entity, and good and reliable treatment is lacking. In the present randomized, sham-controlled, patient- and evaluator-blinded study, 12 patients with a disabling, long-standing and treatment-resistant strictly unilateral cervicogenic headache were included. The diagnosis was based on purely clinical criteria. Six were randomized to receive radiofrequency neurotomy of facet joints C2-C6 ipsilateral to the pain, and six were randomized to sham treatment. Patients were followed for 2 years with diary registration of pain for 14-days periods after 1, 3, 6, 12, 18 and 24 months, and also followed with algometry and neck mobility measurements at 3, 12 and 24 months. Side-effects were minor and short-lasting, and those patients who were treated with neurotomy were somewhat improved at 3 months, but later there were no marked differences between the groups. In conclusion, the procedure is probably not beneficial in cervicogenic headache.
Introduction
Although the notion that headache may stem from the neck is an old one, the term cervicogenic headache (CeH) was first introduced in 1984 (1) and clinically useful criteria for the diagnosis published in 1990 (2) and revised in 1998 (3). The interobserver reliability for these criteria has been found to be as good as those for migraine and tension-type headache (4). The clinical picture can be explained anatomically by a convergence of fibres from the upper cervical segments and trigeminal fibres in the spinal tract of the trigeminal nucleus which extends as far down as the C3 segment (5, 6). It has, however, also been shown that pathology as far down as the C7 may give rise to CeH (7).
The concept of CeH is not universally accepted, and the precise pathology in the neck that should give rise to the pain has not been found. Among the candidate structures are the upper cervical nerves (greater and lesser occipital nerves; GON and LON), nerve roots, cervical muscles, cervical discs and facet (‘zygoapophyseal’), atlantoaxial and atlantooccipital joints. Neck trauma in the history is said to be typical (2), and the CeH related to trauma may differ somewhat from the type occurring spontaneously (8).
Various treatment modalities directed towards these structures have been attempted. Of the more promising approaches is radiofrequency (RF) neurotomy of the cervical facet joints (9, 10). The main aim of the present study was to investigate the effects of RF denervation of facet joints C2-6 on the side with pain in a group of patients with CeH.
Materials and methods
Patients
Patients were included from March 1997 until December 1999 from the outpatient clinic of the Department of Neurology. CeH was defined according to a somewhat simplified version of the criteria from 1990 (2), which all had to be fulfilled in a single patient:
Strictly unilateral headache without side-shift.
At least 2 of the following, indicating neck involvement:
Reduced range of motion in the neck (on clinical examination);
Precipitation of typical headache by palpation or pressure exerted against muscle insertions in the occiput or the neck;
Precipitation of typical headache by neck movements or positions;
Irradiation of pain to ipsilateral shoulder or arm.
These criteria are purely clinical in the sense that they do not mention blockade effects. Blockades were nevertheless performed in all patients, but since we intended to investigate to what degree blockade effects would predict treatment outcome, they were not among the inclusion criteria.
In addition, the patients should be between 25 and 65 years and have relatively severe complaints lasting for more than one year inhibiting participation in work or social life, and insufficient effect of appropriate prophylactic headache medication. Cerebral CT or MRI and cervical MRI, taken within 3 years before inclusion, should be without significant pathology.
Exclusion criteria were the following:
Cervical spinal stenosis or disc herniation;
previous neck surgery;
malignant disease;
rheumatic or other disease necessitating intake of analgesics;
other clinically significant disease, clinically significant concomitant headache disorder;
ongoing or pending litigation for compensation after trauma.
Study design
The study was conducted as a randomized, patient- and evaluator-blinded, sham-controlled study. Before inclusion, all patients were subjected to a neurological and general medical examination. After inclusion, before treatment, patients were instructed to fill in a patient diary at home. For each day during a 14-day period, they were asked to indicate the maximal intensity of head pain, neck pain and arm or shoulder pain (0, no pain; 1, mild pain; 2, moderate pain; 3, severe pain), total duration of pain in hours, and analgesic medication (number of tablets). The same diary was used 1, 3, 6, 12, 18, and 24 months after treatment.
Range of motion (ROM) in the neck and algometry were performed by the study nurse as described in detail previously (11, 12). Measurements of ROM (active movements) with a baseline inclinometer were carried out in three dimensions (maximal flexion/extension, lateral flexion, and rotation). For all movements, the average of three measurements was calculated. Algometry was done by measuring pain pressure threshold with an algometer. In contrast to the study by Sand et al. (12), we only investigated 3 points on each side of the head (temple, mastoid process, occipital region), and also included 2 points on each side of the neck (transverse processes of C2-C3 and transverse process of C5-C6). The difference in pain threshold between the nonsymptomatic and the symptomatic side was calculated, and the average of three single trials performed with a few minutes interval was used in the statistics. Neck ROM and algometry were also performed during visits to the department at 3, 12 and 24 months after treatment. At these visits, the patients also had a consultation with the neurologist, who made a thorough examination and asked about possible side-effects and the global effect of the treatment.
As the primary efficacy variable, it was decided to use the variable ‘days with intense pain’, defined as the number of days per 2 weeks with pain intensity 2 (moderate) or 3 (severe) which would reflect the number of days where headache interfered with the function of the patient. A meaningful clinical response was defined as a reduction of at least 30% of days with significant headache.
After inclusion, patients were randomized in blocks of 4 and stratified in two groups, based on whether the patients perceived their complaints to be caused by a trauma or not, to receive either RF denervation or sham treatment. The randomization was carried out by colleagues at the Hospitals’ Stroke Unit who communicated the result of the randomization only to the operator. In our setting, it was for practical reasons impossible to blind the operator as to the results of the randomization. The patients, and the evaluators (LJS and GH), working in another department in another building than the operator, had no access to the results of the randomization.
All patients received written and oral information about the study design, treatments and possible hazards, and all signed a written consent before inclusion. The study was approved by the Regional Committee for Ethics in Medical Research, and by the Norwegian Data Inspectorate.
Blockades and treatment
Blockades of the greater occipital nerve (GON) on the symptomatic side was performed before inclusion as previously described (13). Before neurotomy, all patients were also given diagnostic cervical medial branch blockades of the facet joints C2-6 on the symptomatic side. On each level, the blockades were performed in accordance with the technique described in International Spinal Injection Society Guidelines with regard to the needle positioning and amount of local anaesthetic given (14), but the results of the blockades were not among the inclusion criteria. In a first trial, patients received 0.5 ml lidocaine, and in a second trial a few days later 0.5 ml bupivacaine. Patients evaluated the effect of all blockades by indicating on a VAS scale the level of pain at the start and then every 10 min after the procedure for at least 4 h. The effect was calculated as the maximal pain reduction within the first 3 h in percent of the level just before the procedure.
The cervical RF medial branch neurotomies were performed on facet joints C2-6 on the symptomatic side under aseptic conditions, with the patient supine on an operating table with a narrow radiolucent head/neck extension. The facet joints C2/3–5/6 on the pain side were identified using a movable C-arm fluoroscope, and a RF generator (RFG-3C Graphic, Radionics, Burlington, MA, USA), RF electrodes with temperature monitoring capacity (50 mm, 22 gauge cannulae/Thermocouple electrode, SMS-Kit), and diathermy ground plate were prepared. Under fluoroscopic control, the electrode was placed parallel to the medial branches of the facet joints with a percutaneously posterolateral approach. The blunt electrode was inserted through the neck muscles striking the articular pillar just dorsal to the root canal, parallel to the facet joints. The electrode was then carefully redirected so as to just slip past the lateral margin of the pillar. The position of the electrode was viewed under lateral and AP fluoroscopy. Stimulation was now carried out (50 Hz), and if required followed by repositioning of the electrode. After the injection of 1 ml of local anaesthetic the patient then received three to four lesions (85°C) for 60 s. The position of the electrode was checked between the lesions which were given 1 mm apart, moving the electrode from caudal to cranial direction. The lesions given to the C2-3 facet joint were made by directing the electrode at an oblique and sagittal direction towards the third occipital nerve, and then two to three lesions were given to denervate the facet joint.
Patients randomized to the sham procedure went through exactly the same operation, except that after local anaesthesia, no lesions were given although the needles were positioned as described above. Both the RF and the sham procedure lasted about 90 min.
Sample size and statistics
Since the variance of the primary efficacy variable was not known, it was impossible to calculate sample size beforehand, but we assumed that at least 24 patients would be needed (9), and that inclusion would take 1.5–2.0 years. Sample size estimations were done post hoc on the basis of the primary efficacy variable in the pretreatment period of all included patients (n = 12, mean 11.4 days/2 weeks, SD 3.1) according to the method described by Altman (15). To detect a moderate effect (on average 30% reduction in headache days) with 80% probability at a 5% significance level would require 24 patients (12 in each group), and to detect a marked effect (50% reduction) would require 12 patients (6 in each group). It turned out to be much more difficult to recruit patients than we had calculated, and after 2.9 years we had only included 12 patients. It was problematic to find patients with a pure CeH without concomitant migraine or tension-type headache, and many patients were also ineligible because they had contacted private clinics in and outside Norway to get RF-treatment of facet joints. It was therefore decided to terminate the study after 12 included patients.
For all efficacy variables, the percent change from baseline (before treatment) was calculated. Due to small sample size and non-normal distributions of results, all comparisons between groups were performed with nonparametric methods (Mann–Whitney U-test) for continuous variables. Fisher's Exact Test was used for comparing proportions. P-values ≤ 0.05 were considered statistically significant. Statistical Package for the Social Sciences (SPSS, Chicago, IL, USA), release 11.0.1, was used in the analyses.
Results
All 12 patients fulfilled the 1990 criteria for CeH (2). Eleven patients received blockades of the facet joints twice, and 1 only once. Data with relevance to the diagnosis in each of the 12 patients receiving treatment is given in Table 1, and MR findings and comorbidity is given in Table 2.
Data with relevance to diagnosis of CeH (Patient 1–6: RF group, 7–12: sham group)

M, male; F, female; R, right; L, left; ROM, range of motion; ↓, reduced; (↓), slightly reduced; n.d. not done; Facet1/Facet2, Facet joint blockade C2-C6; number 1 and number 2.
MRI findings and previous and concomitant illnesses

M, male; F, female.
Patient no. 3 died between month 6 and 12 in the study from a traumatic cause, totally unrelated to the study according to her primary physician. Patient no. 4 could not attend at one year, and patient no. 8 did not fill in the diary at 24 months. In addition, some diaries were incompletely or incorrectly filled in for some variables. The number of valid observations for each variable at the various time points is given in Table 4.
Treatment effect in individual patients (global impression/days with intense headache from pain diary), relation to trauma and litigation, and side-effects reported after the procedure and at 3 months

M, male; F, female; Y, yes; N, no; ↓, worse; →, No change; ↑, Improved; ↑↑ Markedly improved; – patient unavailable.
∗Patient could not attend consultation but filled in pain diary at month 3
∗∗Patient attended to consultation but did not fill in pain diary at 24 months.
Ongoing or pending litigation after trauma was an exclusion criterion. In one patient (no. 3), a case for trauma-related disablity pension had been completed > 1 years before inclusion. Three other patients (nos. 1, 2 and 8) started a process for getting such compensation before the end of the study.
Compared to the sham group, patients in the RF-group were on average 8 years younger and had had the complaints for a shorter period, but they had longer lasting pain each day and somewhat more intense pain in head, neck and shoulder, and less neck mobility. With algometry, however, the sham group had a more distinct unilaterality of the tenderness (Table 3). The RF-group had better effects of blockades of facets joints. With regard to MRIs, no marked pathology was found in either group (Table 2).
Baseline variables (median and range for continuous variables)
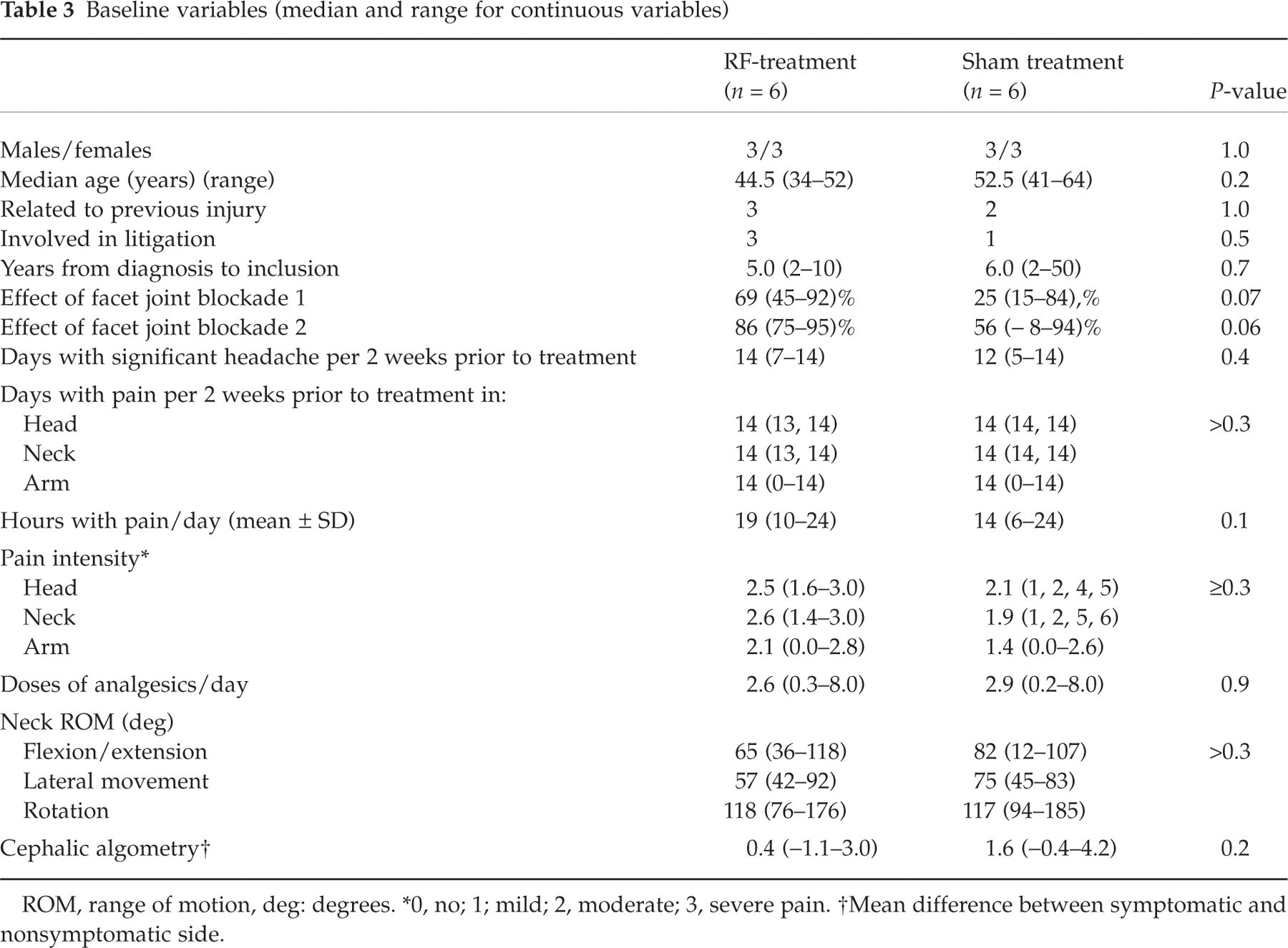
ROM, range of motion, deg: degrees.
∗0, no; 1; mild; 2, moderate; 3, severe pain.
†Mean difference between symptomatic and nonsymptomatic side.
As to side-effects, more patients in the RF-group reported increased neck pain (4/6) than in the sham group (1/6) at discharge from the hospital 1–2 days after the procedure (Table 4). After three months only one patient in the treatment group and none in the sham group reported worsening of neck pain for some time after discharge from the hospital. Patient no. 9 got an acute form of rheumatoid arthritis between month 6 and 12, and her consumption of analgesics increased dramatically in this period, which markedly increased the average analgesics consumption in month 12 in the sham group (Table 5). This patient reported that the head and neck pain was unchanged at this time, and the arthritis went in remission in the following year.
Variables from pain diary

‡n = 5
†n = 4.
The effect in each patient at 3, 12 and 24 months is given in Table 4 where both the global impression and the primary efficacy variable are shown. At 3 months, 4 patients in the treatment group and 2 in the sham group had a meaningful clinical response (≥ 30% improvement), but at 24 months only 1 (of 5) patients in the treatment group and 3 (of 5) in the sham group had a similar effect. One in the treatment group and none in the sham group had become more than 30% worse at 24 months.
Looking at the group statistics (Tables 5 and 6), only one significant difference was found (arm pain intensity month 3). In month one both groups tend to be better, but in month 3 there seems to be a tendency that the RF-group is doing better than the sham group with regard to all variables except analgesics intake. In month 6 and later the two groups seem to be similar, but in month 24, the sham group is better on most variables (Table 5). A similar pattern is found with regard to the algometry, but with regard to neck mobility, no group seems to be markedly improved (Table 6).
Recordings from visits in department

‡n = 5
†n = 4.
Discussion
Although we could not include as many patients as intended (≥24), power calculations indicate that we should be able to detect a marked treatment effect (>50% improvement) with only 12 patients. Hence, we felt an obligation to report the study since it is the first controlled study on RF-treatment in CeH, and the 2-year follow-up enables detection of possible long-term beneficial and/or harmful effects.
Much effort was expended in order to get a group of patients with typical CeH according to the 1990 criteria (2). Positive effects of blockades of the GON and/or the C2 root on the symptomatic side is an important but not obligatory criterion in the 1990 criteria (2). In the 1998 criteria it has been made an obligatory criterion in scientific works (3). In the IHS classification of 1988, the criteria for headache attributed to the neck (2, 11) are quite unspecific and do not include reference to diagnostic blockades at all (16). In the present study, which used the 1990-criteria, positive effect of blockades was not obligatory, but all patients had received GON blockades prior to inclusion, and after inclusion they also received facet joint blockades (Table 1). One reason for not including blockade effect as a diagnostic criterion was that we wished to test whether treatment outcome could be predicted by blockade effect, but this aim could not be achieved since only 6 patients were given RF treatment. All our patients had at least a 50% effect on at least one of the blockades, but the consistency of the responses in the same patient, particularly among the controls, was not very high (Table 1). Only 4 patients (nos. 2, 6, 9 and 10) had more than 90% effect on at least one of the blockades. Whereas patients nos. 11 and 12, belonging to the sham group, fulfilled the set of criteria proposed in 1990, these patients would not have fulfilled the somewhat more restrictive criteria of 1998. Patient no. 12 actually got worse from the GON blockade, but was more than 50% relieved by one of the facet joint blockades.
When results are evaluated, one must take into consideration that the randomization resulted in two groups of patients that were different in some important respects (age, duration and intensity of complaints, and blockade effects). The fact that the RF-group had complaints of shorter duration could predict a more favourable prognosis in this group, but the fact that the RF-group tended to have more intense pain might have an opposite effect.
The results could also be influenced by the fact that 4 patients (3 in the RF group and 1 in the sham group) were litigants. Patients were excluded if they were involved in litigation at the time of inclusion, but patient no. 3 had had her case settled > 1 years before inclusion, and patients nos. 1, 2 and 8 started after they had received treatment in the study. One would expect litigation to affect the prognosis negatively, but in the present study no clear cut trend could be seen to this effect since patients no. 1 and no. 3 were among those who seemed to improve after RF treatment (Table 4).
Looking at the results in individual patients (Table 4), it seems that the correspondence between global impression of effect and days with intense headache is rather poor. There is no clear-cut relation between treatment effects and a perceived traumatic start of pain (Table 4). Acute side-effects were mild to moderate and relatively short-lasting (Table 4).
When the group data are evaluated (Tables 5 and 6), some tentative conclusions can be made, despite the relatively low power of the study. There seems to be an effect of the treatment at month 3. The fact that it was not possible to discern an effect at month 1 may partly be due to a higher incidence of pain experienced after the RF-procedure than after the sham procedure (Table 4, side-effects). From month 6 no consistent improvement can be seen in the RF-group, neither in comparison with the sham group, nor in comparison with the pretreatment period.
Previously, only one study (open, with no control group) has been made with RF-treatment for CeH (on facet joints from C3-C6) (10). At follow-up 17 months after treatment, patients experienced a mean reduction in headache days of 34% compared to baseline, which is comparable to the long-term results in the sham group of the present study (median 50% reduction). In the RF-group of our study, however, there was virtually no change in this same parameter. The main difference in the operative technique between the two studies is that we treated all facet joints from C2-6, whereas van Suijlekom et al. (10) only treated the C3-6 joints. One may therefore speculate that spontaneous improvement may have been impeded by making a RF-lesion to the C2-facet joint in our RF-group. It has been shown that stimulation of the C2–3 facet joint, but not at lower levels, cause pain in the head (17), and that RF-denervation of the C2-3 facet joint is technically more difficult than denervation at lower levels (18).
In a sham-controlled, double-blind study on 24 patients with neck pain stemming from facet joints (C3-4 level to the C6-7 level) (9) the median time to return of 50% pain was 263 days. This seems better than in the present study where only one patient in the treatment group had a definite improvement at 12 months (Table 4), and where no change was seen in the median of the primary efficacy parameter after 3 months (Table 5). It may be that the results were better in this study because patients had a somewhat different diagnosis, the effect of blockades (double blind, and placebo controlled) were among the inclusion criteria, and only the putatively symptomatic joint, and never the C2-3 joint, was treated (9).
It can reasonably be argued that the lack of effect in our study weakens the validity of the purely clinical criteria. Alternatively, one can argue that the definition is valid but the pain does not stem from the facet joints but from other peripheral structures, e.g. muscles or ligaments. Another possibility is that the pain experienced by most of these patients does not have its origin in any peripheral structure but is a variant of a primary headache.
In conclusion, we do not find much evidence that RF-treatment of facet joints C2-C6 is a promising procedure for most patients fulfilling purely clinical criteria for CeH. It is of some concern to us that many such patients are treated with facet joint neurotomy, despite lack of robust evidence for a beneficial effect. Since results are so dubious, we would recommend that RF-treatment for CeH is not performed on a routine basis, but is restricted to research protocols. A consistent and marked (close to 100%) effect of facet joint blockades should probably be among the inclusion criteria in such studies.