
Abstract

Developmental venous anomaly (DVA, venous angioma) is the most often occurring cerebral vascular malformation, with an estimated incidence of 2.5% in autopsy series (1–4). In one third of patients co-existing other intracranial vascular malformations, predominantly cavernous angiomas (cavernomas) are found (1, 2, 5). The bleeding potential of DVAs is very low, and when present, it is typically caused by associated cavernoma, or less often other vascular malformations, and not the DVA (1, 2, 5, 6). Only a few cases of haemorrhage in patients with DVA have been reported in absence of other vascular malformations, and the bleeding was uniformly intraparenchymal (7–9).
Subarachnoid haemorrhage (SAH) related to DVA, without intraparenchymal haemorrhage has not been previously reported.
Case report
A 39-year-old male presented with sudden intense headache with onset during exertion (lifting heavy aquarium) three hours before admission. Headache was localized occipitally and was accompanied by nausea and vomiting. Mild headache preceded the intense headache, but the patient was convinced that they were connected with tension and light exertion. Neurological examination revealed neck stiffness, with no other abnormalities. Routine blood tests were normal, and laboratory tests did not reveal any haematological abnormality. Brain computerized tomography performed at admission, demonstrated a subarachnoid haemorrhage (SAH) in the basilar cisterns and the fourth ventricle (Fig. 1a), and an infratentorial hyperdense vascular structure (Fig. 1b). Magnetic resonance (MR) imaging performed 16 h after the onset of headache, and 12 h after the CT study, showed an anomalous dilated infratentorial vein, presumably corresponding to precentral vein, with a rim of high signal intensity on T1 weighted images, suggesting partially recanalized thrombosis (Fig. 2). There was no evidence of other vascular malformations on MR imaging. Magnetic resonance venography (MRV) showed diminished flow through the distal portion of the anomalous vein, just proximal to the vein of Galen (Fig. 3). Small veins arising in the cerebellar parenchyma just behind the fourth ventricle were joined together to form the proximal aspect of the anomalous vessel. On subsequent intra-arterial digital subtraction angiography (DSA) this vein was again demonstrated, with irregular narrowing in its distal segment (Fig. 4a). A number of small veins arising adjacent to the fourth ventricle were draining into it, with a characteristic ’caput medusae’ appearance (Fig. 4b). Cerebral aneurysms, arterio-venous malformations and dural fistulas were excluded on DSA. Gradient-echo T2∗-weighted images were incorporated in study, and did not demonstrate any evidence of cavernous angioma or intraparenchymal haemorrhage. The headache resolved, and the patient was discharged.
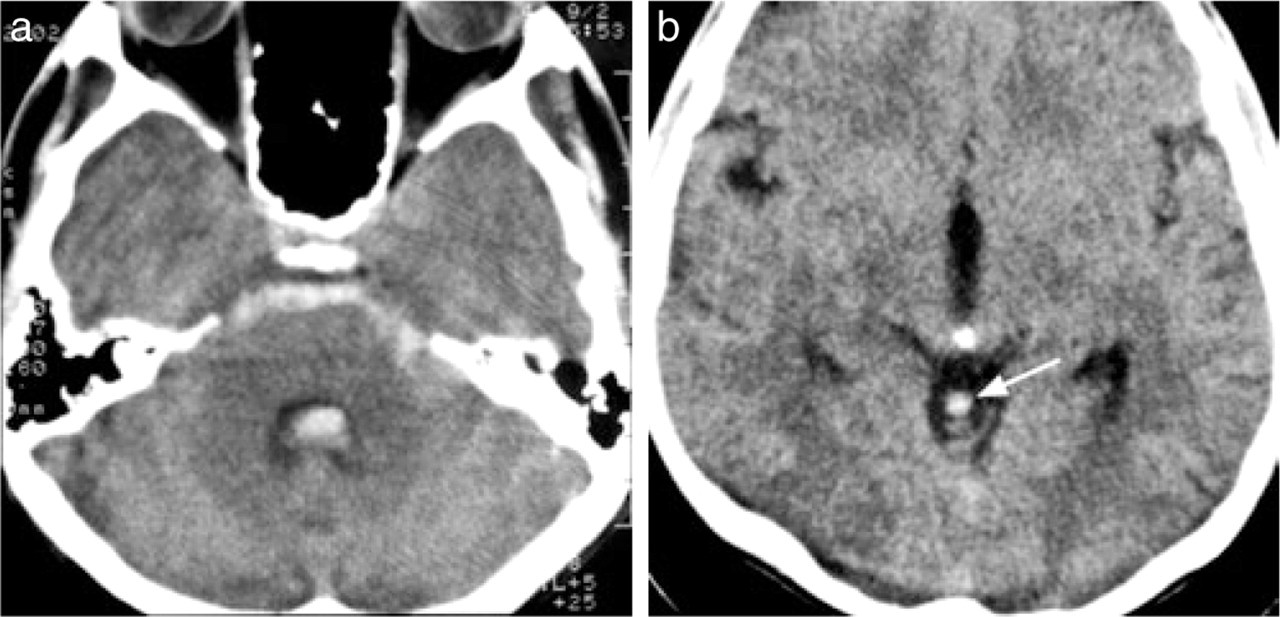
Brain CT upon admission. (a) Subarachnoid haemorrhage (SAH) is seen in the basilar cisterns and the fourth ventricle. (b) A hyperdense structure is seen near the midline in the supravermian cistern (arrow). This abnormal vessel, which was considered thrombosed, was extending from the cerebellum to the vein of Galen.

Sagittal T1-weighted MR image performed the following day. There is a vascular midline structure extending from vermis to the vein of Galen (arrow), with a rim of higher signal intensity, corresponding to thrombus. Isointense areas in the basilar cisterns and the fourth ventricle correspond to SAH (arrowhead).

Oblique maximum intensity projection (MIP) of 2D time-of flight MR venography (MRV). The abnormal draining vein is again well visualized (arrow). There is diminished flow in its distal portion (arrowhead).

Intra-arterial digital substraction angiography performed 20 min after MR imaging (a) Lateral projection of a venous phase angiogram reveals irregular and narrowed lumen in the distal aspect of the anomalous vein (arrow). (b) Frontal projection of a venous phase angiogram shows ‘caput medusae’ (arrow), a characteristic DVA feature, in the cerebellum just posterior to the fourth ventricle. The other characteristic part of DVA, the anomalous draining vein is also well seen (arrowhead).
During the following six months he has not experienced headaches, or other neurological symptoms. Follow up MR imaging with MRV was performed five months later, and showed regular lumen and flow through the DVA (Fig. 5), with gradient-echo T2∗-weighted images, and did not demonstrate any evidence of cavernous angioma or intraparenchymal haemorrhage.

Oblique MIP of MRV at follow-up MR imaging study five months after admission The vein draining of the DVA is clearly seen (arrow), and the signal in its distal aspect, corresponding to flow, is much higher compared to Fig. 3.
Discussion
This is the first case of SAH caused by a thrombosed DVA, without parenchymal haemorrhage. We presume that a small intraparenchymal haemorrhage just adjacent to the clot in the fourth ventricle could have been present, but not distinguished by imaging studies. The vicinity of the DVA to the subarachnoid space probably explains the prominent subarachnoid haemorrhage. A thrombosed aneurysm may occasionally be missed on intra-arterial angiograms in the acute phase, however, this possibility is virtually excluded in our case, as no aneurysms were detected on either DSA, MRI, or MRA, both at the time of the haemorrhage and on the follow-up studies.
A patient with left parietal DVA and left parietal haemorrhage without demonstration of an associated cavernoma has been described (3). In that report it was not stated whether this was a parenchymal or subarachnoid haemorrhage. In all other patients with DVA and cerebral haemorrhage described in the literature, the symptoms could be attributed to an associated cavernous angioma located at or near the site of the haemorrhage (2), or to arteriovenous shunts (5). The previously reported high incidence of symptomatical haemorrhage in patients with DVA may result from the fact that in the pre-MRI and pre-CT era, the angiographically occult cavernous angiomas were extremely difficult to diagnose (10). Therefore, the cerebral haemorrhage was attributed to the angiographically diagnosed DVA, whenever ’caput medusae’ and a draining vein were identified. Also, some of these DVAs were later intra-operatively correctly diagnosed as arteriovenous malformations (11).
Follow-up studies consider DVA as a benign cerebral anomaly that is very unlikely to become symptomatic (12). DVAs are considered a variation of venous drainage of an otherwise normal brain tissue, as the region of the malformation is characterized by a compete absence of normal draining veins (13). At the same time dilated medullary veins and collecting dilated central veins are present, with the absence of feeding artery (5). According to Lasjaunias et al. (13), lesions represent an anatomical variant of venous drainage, without a venous occlusive condition in early fetal life.
In a series of 67 patients with DVA (1), whose files were retrieved from a large university hospital and a large radiological private practice, there was no association between the complaints that lead to the neuroradiological studies and the DVA diagnosed on MRI. Out of 67 patients, five presented with signs and symptoms of an intracerebral haemorrhage, and in all five an associated cavernous angioma was detected. In a study by Garner et al. (3), out of 100 patients with venous angiomas, haemorrhage occurred only in one patient, and it was parenchymal.
In a report by Uchino et al. (8), out of 82 patients harbouring DVAs, 13 (16%) presented with brain haemorrhage, and in 12 of them it was caused by venous angiomas or associated cavernomas. In one patient sequelae of a haemorrhagic venous infarct were found, possibly caused by thrombosis of the DVA (8). Intraparenchymal haemorrhage was reported in three other patients with DVA, in one of which it was caused by draining vein thrombosis (7, 9).
DVAs are relatively frequent findings, especially on contrast-enhanced T1-weighted MR images, and haemorrhagic events are typically associated with coexisting cavernous angiomas. Extremely rare cases of haemorrhage due to DVA were uniformly parenchymal, mostly associated with infratentorial and deeply draining supratentorial DVAs. Our case indicates that DVA thrombosis may lead to SAH in the absence of parenchymal haemorrhage, the infratentorial location in combination with the exertion probably increased the risk for its development, and it should therefore be included in the differential diagnosis of acute subarachnoid bleed, possibly accounting for some of the nonaneurysmal SAH cases.