
Abstract
The dilatated cyst of the cavum septi pellucidi (CSP) is rare and may be associated with headaches. We reviewed the computerized database of 54 000 patients' computed tomography or magnetic resonance images and found 22 cases (0.04%) involving a dilatated cyst of the CSP. Sixteen patients had a chief complaint of headache, which was classified as acute episodic headache (type I, n = 7, 43.7%), chronic daily headache (CDH) with acute onset (type II, n = 5, 31.3%), or CDH with insidious onset (type III, n = 4, 25%). Acute Valsalva-induced headaches were common with type I (85%) or II (100%); 70% of these responded to indomethacin. At follow-up, patients with type I headache had the highest remission rate (71%), and type III patients the lowest (0%). Dilatated cysts of the CSP should be considered a cause of acute Valsalva-induced headache or new daily persistent headache, and may respond to indomethacin. A protracted course (≥ 3 months) indicates a worse outcome.
Introduction
The cavum septi pellucidi (CSP), erroneously named the fifth ventricle, is an anatomical variant and located between the leaflets of the septum pellucidum. The prevalence of the CSP is low and estimated to be 0.73% in adults in a computed tomography (CT) study (1). The CSP has been widely regarded in clinical neurology or autopsy series as an incidental finding of little clinical importance. Nevertheless, the presence of the CSP is also considered a putative marker of disturbed brain development (2).
Compared with the CSP, a dilatated cavum or a cyst of the CSP is even rarer. According to Shaw and Alvord (3), a cavity in the septum pellucidum is called a cavum, generally implying an incidental anatomical variation of no clinical significance. When the cavity is larger than usual, it may be called a cyst, a congenital cerebral cyst of the cavum, or a dilatated or widened cavum. Sarwar (4) further defined a cyst of the CSP as a fluid-containing structure between the lateral ventricles whose walls exhibit lateral bowing instead of being parallel and are 10 mm apart or greater. Such cysts are reportedly related to a variety of neuropsychiatric disorders, including headache, acute hydrocephalus, loss of consciousness, autonomic dysfunctions, seizures, and psychiatric problems (5–9). The current hypothesis suggests that these pathological symptoms may result from an enlarged cyst that obstructs the interventricular foramen and thus hinders the passage of cerebrospinal fluid (CSF), as some patients have been found to have a manifestation of intermittent hydrocephalus (10).
In a large series of surveys of patients with the CSP, headache was the most common chief complaint (11). Previous case reports mentioning headache frequently stress the use of surgical techniques to remove the cyst, but do not focus on the headache profiles or the outcome of patients not undergoing surgical intervention (6, 8, 10). We retrospectively studied the clinical characteristics and prospectively assessed long-term outcomes of a cohort of patients with a dilatated cyst of the CSP who presented with headache.
Methods
Enrollment of patients
We searched for consecutive case series of all patients with a CT or magnetic resonance imaging (MRI) report of dilatated cysts of the CSP. Computer records of neuroimaging examinations done at Taipei Veterans General Hospital from 1998 to 2002 were reviewed. A dilatated cyst of the CSP was identified if the maximal diameter exceeded 1.0 cm with lateral bowing, as shown on brain MRI or CT scans (4). The size of the dilatated cyst and the presence or absence of bowing of its walls were based on the axial T2-weighted MRIs. If MRIs were not available, CT scans were used.
Headache profiles and follow-up
Patients included in the final sample were those with headache as the chief indication for neuroimaging studies. Their headache profiles were identified according to the results of the headache intake form of our headache clinic or hospital medical records. Headache characteristics, such as headache pattern, location, frequency, duration, precipitating factors, accompanying symptoms, and treatment efficacy, were recorded. One physician (K-C.W.) called all of the patients for a semistructured headache questionnaire to follow up their current headache profiles and clinical condition in June 2003.
Comparison with headache control patients
We found that patients with a dilatated cyst of the CSP frequently reported Valsalva-induced headache (see below). In order to determine if the link was a chance association, we compared the frequency of Valsalva-induced headache in a compatible control group without a dilatated cyst of the CSP. We reviewed consecutive patients in our headache clinic from November 2002 to October 2003, whose brain neuroimages (MRI and/or CT) did not reveal obvious intracranial lesions or a cyst of the CSP. These patients were chosen as a control group because during this period the presence or absence of Valsalva-induced headache was specifically queried; the relevant activities included straining at stool, lifting heavy objects, exercise, sex, coughing, and holding breath.
Results
Twenty-two consecutive patients(10 men and 12 women) with a dilatated cyst of the CSP were identified from 54 000 patients who underwent cranial CT or MRI in 1998–2002, a prevalence of 0.04%. Among the 22 patients, six did not experience headaches, and their chief complaints were seizure (n = 2), injuries due to a traffic accident (n = 2), trigeminal neuralgia (n = 1), and an abnormal sensation over the tongue (n = 1). Headache was the chief complaint for neuroimaging studies in 16 patients (72.7%; nine male, seven female), who formed the final sample for this study.
The patients’ initial headache profiles were identified from the headache intake form (n = 13) or hospital medical records (n = 3). Twelve patients had MRIs and four had CT scans. Table 1 shows the demographic data, headache pattern, and radiological findings of the dilatated cyst of the CSP. In addition to the cyst, some patients also had a dilatated septi vergae (sixth ventricle) and slight blunting of the frontal horn (Fig. 1). The mean age at diagnosis was 32.5 ± 13.4 years (range 14–52 years). The mean diameter of cyst was 1.61 ± 0.35 cm (range 1.1–2.3 cm).

Magnetic resonance imaging of the brain in patient 11, who presented with an acute postcoital headache. (a) Axial three-dimensional spoiled gradient recalled-echo images (TR/TE/NEX/flip angle, 10/4.2/2/15°) show the dilatated cyst of the cavum septi pellucidi (CSP), which is about 1.7 cm in width (arrows). The cavum vergae are also shown (arrowheads). (b,c) Coronal contrast-enhanced T1-weighted images (TR/TE/NEX, 550/20/1) show the dilatated cyst of the CSP, which causes lateral bowing and blunting of the frontal horns of bilateral lateral ventricles (arrows). The dilatated cyst compresses the opening of the interventricular foramina, possibly hindering the flow communication of the cerebrospinal fluid (arrowheads).
Characteristics of patients with a dilatated cyst of the cavum septi pellucidi and headache

CM, Chronic migraine; CTTH, chronic tension-type headache; ETTH, episodic tension-type headache; NDPH, new daily persistent headache.
Classification of headache profiles
We identified three headache patterns among these patients (Table 2). Type I was acute episodic headache with duration < 3 months. Type II was acute headache followed by chronic daily headache (CDH) of > 3 months, similar to the characteristics of new daily persistent headache (NDPH) that Silberstein et al. proposed (11). Type III was CDH longer than 3 months but with an insidious onset. Among our patients, seven (43.7%) had headache classified as type I; five (31.3%), type II; and the remaining four (25.0%), type III. In total, 12 patients had an onset of severe acute headache and nine patients had CDH for longer than 3 months.
Classification of headache and radiological pattern in patients with a dilatated cyst of the cavum septi pellucidi

Case illustrations: examples
Patient with headache type I: acute headache (patient 15)
A 25-year-old man visited our emergency department (ED) at the age of 23 because he suddenly developed a severe headache when he was getting up from his chair after watching television for hours. The pain was explosive and involved his entire head. It reached maximal intensity immediately, and physical activity exacerbated the pain. He denied any aura, nausea, or vomiting, but he did have photophobia and phonophobia. In the ED, neurological examination did not show any abnormalities. Brain CT revealed a 1.4-cm, dilatated cyst of the CSP with lateral bowing. Ketorolac 30 mg was intravenously administered, but the severe headache persisted for several hours. The patient had a similar headache once when he was 20 years old. At the 2-year follow-up, no further headaches had occurred.
Patient with headache type I: acute swimming headache (patient 9)
A 52-year-old woman, a daily swimmer, noted sudden onset of severe headache while swimming one day at the age of 50. The headaches were pulsatile over her entire head and were not accompanied by nausea, vomiting, photophobia, or phonophobia. The pain lasted for hours but recurred within 5 min when the patient swam in the following 3 days. No other exertional factors or Valsalva manoeuvres, including cough, straining at stool, or lifting heavy objects, induced the pain. CT of the brain revealed a dilatated cyst of the CSP measuring 1.3 cm in width. The patient's swimming-induced headache was responsive to indomethacin (75 mg/day). By follow-up at 2 years, no more swimming-induced headaches had occurred.
Patient with headache type II: CDH with an acute onset (patient 3)
A 36-year-old man had daily headaches after a traumatic accident involving a lumbar spinal fracture at the age of 34. The patient reported no exact history of head injury, and no neurological deficit was observed. The pain involved a sensation of fullness over both temples and the posterior aspect of the neck, usually accompanied by phonophobia and photophobia. Each headache lasted at least 4 h but < 1 day. The headaches were exacerbated by exertion. The patient tried several remedies, including cervical traction, to relieve his headache but these were unsuccessful. He visited our headache clinic, where brain MRI showed a 1.2-cm dilatated cyst of the CSP. Indomethacin was given for acute headaches; fluoxetine was added for chronic headache prophylaxis. At follow-up about 22 months after disease onset, his headaches had improved but were still episodic.
Patient with headache type III: CDH with an insidious onset (patient 8)
A 39-year-old woman had migraines with and without aura since age 18 years. Her father also had a history of migraine. The patient's migraines were exacerbated after she gave birth at the age of 30 years. The pain was pulsatile, located unilaterally in one temple, then spreading bilaterally. They were usually accompanied by nausea, vomiting, phonophobia, and photophobia. Her headaches later became daily and were invariably exacerbated by menstruation. She overused painkillers and had undergone several hospitalizations for detoxification. In addition, she had a poor response to many headache prophylactic agents, including nadolol, flunarizine, fluoxetine, and valproic acid. Sumatriptan and indomethacin were effective for temporary pain relief. Brain MRI showed a 2.1-cm dilatated cyst of the CSP with lateral bowing (Fig. 2a). She underwent endoscopic fenestration of the cyst. After the operation, her headache subsided until 8 months later, when it recurred but with only episodic migraine attacks, an outcome much better than before surgery. She had been using topiramate and nadolol as migraine prophylaxis. Follow-up MRIs performed 6 and 10 months after surgery revealed no recurrence of the cyst (Fig. 2b).
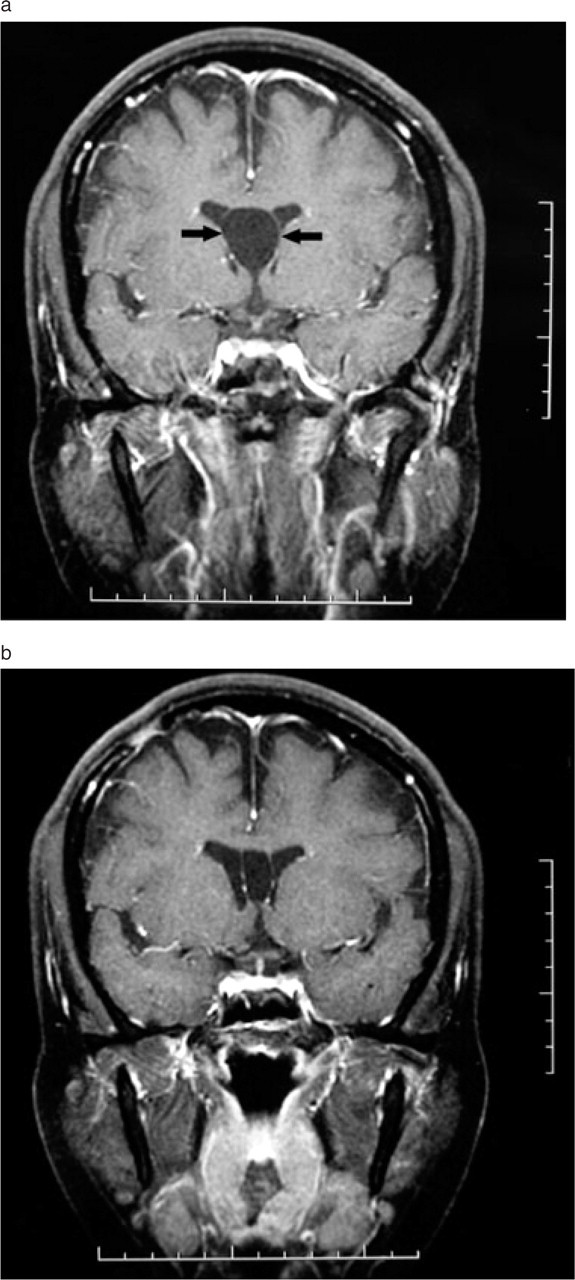
Magnetic resonance imaging (MRI) of the brain in patient 8, who presented with chronic migraine and underwent endoscopic fenestration of the cyst. Follow-up MRI performed 6 and 10 months after surgery revealed no recurrence of the cyst. (a) T1WI (TR/TE/NEX 550/20/1) MR images show a cyst of cavum septi pellucidi with bowing of the walls (arrows) into the frontal horns before endoscopic fenestration. (b) T1WI (TR/TE/NEX 550/20/1) MR images 10 months after surgery do not show recurrence of the cyst (disappearance of the wall bowing).
Summary of headache profiles
Table 3 shows the headache profiles of the three groups of patients. Most patients had explosive headache of moderate to severe intensity. The headaches were usually bilateral (87%). The diameter of the cyst did not differ among the three types of headache. The patients’ headaches were usually acute and severe; 10 of 16 patients (62.5%) had visited an ED for help.
Headache profiles in patients with a dilatated cyst of the cavum septi pellucidi (CSP)

∗At least one of the four associated features: nausea, vomiting, photophobia, or phonophobia.
The other symptoms, such as nausea, vomiting, photophobia and phonophobia, were frequently encountered in type II (60%) or III (100%) headaches, but not in type I (29%) headaches. Unlike the type III group (25%), most or all of those of type I (85%) or type II (100%) reported Valsalva-induced headache.
Treatment
Medical treatment
Indomethacin (50–75 mg/day) was given to those with acute exertional headache (n = 10), with a fair response reported by seven patients (70%). A diuretic (furosemide 40 mg/day) was given to four patients (two with type II and two with type III headaches). Two patients reported a decrease in headache intensity. Headache prophylactic agents were given to four patients in the type II group and four patients in the type III group. Three patients (75%) with type II headaches and one (25%) with type III headaches reported a decrease in headache frequency after treatment.
Surgical intervention
Two patients received endoscopic fenestration to remove the cyst of the CSP: patient 16 with acute headache lasting for 3 months (type II) and patient 8 with chronic migraine (type III). For the former patient, the acute headache was resolved without recurrence. For the latter patient, the daily headaches resolved for 8 months but recurred, with episodic migraine attacks.
Outcome follow-up
At a mean follow-up of 20.9 ± 16.7 months (range 6–60 months) (Table 4), all patients were successfully contacted by telephone. In the type I group, two patients (29%) experienced only episodic headaches, and most patients (five of seven, 71%) were headache free. In the type II group, only two patients (40%) were headache free. In the type III group, none of the patients was headache free at follow-up. Two patients (50%) improved, with intermittent headaches; these included one patient who underwent endoscopic fenestration. The remaining two patients still had CDH after headache prophylaxis.
Headache features at follow-up

Comparison with headache control patients
A total of 201 patients (56 men, 145 women) with a mean age of 45.8 ± 15.6 years (range 14–86 years) without a cyst of the CSP and obvious organic lesions were included in this analysis during the study period. MRI was done in 157 (78.1%), CT in 38 (18.9%) and both in six (3%). Of them, 44 (21.9%) reported having experienced Valsalva-induced headache. The frequency was significantly lower than in patients with a cyst of the CSP in neuroimaging [21.9% vs. 75% (12/16), P < 0.0001, Fisher's exact test, two-tailed].
Discussion
We found that dilatated cyst of the CSP was rare, with a 0.04% prevalence in brain CT or MRI studies. Headache was the most common symptom (72.7%) in our series. Diagnosis was made only after brain imaging studies were done. Three types could be delineated: acute episodic headache (type I), CDH with acute onset (e.g. NDPH; type II), and CDH with insidious onset (type III). Valsalva-induced headache was one characteristic of the patients with a component of acute-onset headache (types I and II). The prognosis was generally unsatisfactory in those with a protracted course, especially those in the type III group with CDH.
In the acute-headache groups (types I and II), several patients were triggered by a Valsalva maneuver. These patients often went to an ED for help. The exertional component might have resulted from transient hydrocephalus caused by occlusion of the foramen of Monro by the dilatated cyst (10). Indomethacin seemed effective for this type of headache. It reduced the intracranial pressure by decreasing CSF production or cerebral blood flow (12). Chance association between Valsalva-induced headache and the dilatated cyst of the CSP cannot be completely ruled out. However, the frequency of Valsalva-induced headache in these patients was much higher than that in a headache control group without a dilatated cyst in the brain (75% vs. 21.9%). We consider the selection of this control group as compatible because most of the patients with the cyst of the CSP (13/16 = 81%) in this study also came from our headache clinic. It is noted that the prevalence of Valsalva-induced headache in our headache control group was higher than that reported from a community-based population (12.3%) (13). This is possibly because we surveyed this symptom in headache sufferers rather than the general population. We believe the control data would strengthen the association between the Valsalva-induced headache and cyst of the CSP.
It is of interest that patients with type II headaches, i.e. acute headache followed by CDH, had both acute and chronic components found in types I and III. We do not know if type II is transitional between type I and III. Patients with type III headaches might have had a protracted course and forgot their initial acute headaches. Patients with CDH were more resistant to treatment compared with those having only acute headaches.
The relationship between the dilatated cyst of the CSP and type III headaches with CDH is not clear, and may be incidental. Our patients with type III headaches had features similar to those of patients with chronic migraine or chronic tension-type headache. These features described by Silberstein et al. (14) have been adopted by the International Classification of Headache Disorders, 2nd edition, 2004 (15). The exertional components are not common. Unexpectedly, the improvement of headache symptoms after endoscopic fenestration in patient 8 provided a possible link, though preliminary. We hypothesize that the dilatated cyst in this patient might have resulted in mechanical obstruction that transformed the episodic migraine attacks to CDH. Therefore, the patient's headache returned to intermittent attacks after fenestration of the cyst. Nevertheless, the association between a dilatated cyst and persistent headache is still in doubt and needs further confirmation.
Lancon et al. reviewed 18 patients (14 male, four female; mean age 28.7 years) with dilatated cysts of the CSP who were reported in the literature from 1931 to 1996 (10). Headache (61%) was the most frequent symptom, as in our series. However, their patients also had other neurological or behavioural disturbances, including mental status change (58.8%), syncope (35.2%), sensorimotor and reflex changes (56%), and neuro-ophthalmological findings (papilloedema in 33.3% and abducens palsy in 16.6%). Of the 18 patients, 14 received surgery, and four patients spontaneously developed rupture of the cyst at the time of pneumoencephalography. All had good outcomes. This finding is in contrast to that in our patients, most of whom did not have neurological deficits and half of whom had protracted headaches (≥thinsp;3 months). Moreover, most patients in the type I group had a good outcome, even without surgical intervention. Selection or publication bias might have contributed to any discrepancy in clinical features between our patients and the case report by Lancon et al. (10). Therefore, surgical intervention for patients with a dilatated cyst of the CSP should be more conservative. Nevertheless, two of our patients did have positive results after endoscopic fenestration of the cyst; one had type II and the other type III headache. The first patient improved after relief of acute hydrocephalus; however, we could not provide a reasonable explanation for a dilatated cyst of the CSP in relation to CDH, as in the second patient.
In conclusion, dilatated cyst of the CSP should be considered a cause for Valsalva-induced headache, as well as NDPH, and it might respond to indomethacin. However, because of its very low incidence we do not suggest that one should suspect the presence of a dilatated cyst of the CSP in patients reporting Valsalva-induced headache. In our patients, the prognosis was usually good for those with acute onset of headache. However, the relationship between a dilatated cyst of the CSP and CDH with insidious onset is still unclear. The outcome in the latter group of patients was generally not satisfactory.
Footnotes
Acknowledgements
This study was supported in part by a grant from Veterans General Hospital-Taipei (VGH 331).