
Abstract
Both preclinical and clinical data link glutamate to the migraine pathophisiology. Altered plasma, platelets and cerebrospinal (CSF) glutamate levels have been reported in migraine patients. Chronic migraine is comorbid with several conditions. It has been recently shown chronic migraine comorbidity with fibromyalgia. The objective of this study was to study cerebrospinal fluid glutamate levels in chronic migraine patients with and without fibromyalgia. We studied 20 chronic migraine patients, with and without fibromyalgia, compared to age-sex matched controls. CSF glutamate levels were measured by HPLC. CSF glutamate demonstrated significantly higher levels in patients with fibromyalgia compared to those without fibromyalgia. Patients overall had higher CSF glutamate levels than controls. Mean pain score correlated with glutamate levels in chornic migraine patients. Tender points, the hallmark of fibromyalgia, can be considered as pressure allodynia, and is probably mediated by central sensitization, with increase in CSF glutamate levels. We postulate chronic migraine patients with fibromyalgia, in addition to have more disabling headaches, suffer from a more severe central sensitization process. This subtype of patients may respond to medications modulating glutamate receptors. Headache intensity correlate with glutamate levels in chronic migraine patients.
Introduction
Glutamate is a major excitatory neurotransmitter in the central nervous system, widely involved in migraine mechanisms. Glutamate is implicated in cortical spreading depression, trigeminovascular activation, and central sensitization. Both preclinical and clinical data link glutamate to the migraine pathophysiology (1).
Chronic migraine (CM) is a common disorder, affecting 2–3% of the general population (2), CM is one of the most debilitating (3) and difficult to treat headache disorders (4). CM is comorbid with several conditions, particularly depression, anxiety, insomnia (5). It was recently described fibromyalgia is present in 35% of CM patients (6), associated with more debilitating headaches (7).
Altered glutamate levels have been reported in migraine patients (1). It has been reported higher levels of CSF and plasma glutamate in episodic migraine patients compared to controls (8, 9). Gallai et al. (10) reported higher CSF glutamate levels in chronic daily headache patients.
Central sensitization has been implicated in chronic migraine pathophysiology (11). It is also involved in fibromyalgia (12), however, to date, glutamate levels have never been studied in chronic migraine patients with and without fibromyalgia.
Patients and methods
Patients
We studied 20 (6 male, 14 female) patients diagnosed with chronic migraine according to Silbertstein et al. criteria (13). Patients underwent a lumbar puncture in order to rule out idiopathic intracranial hypertension, present in 5–14% of chronic daily headache series (14–16). Twelve patients were diagnosed with fibromyalgia according to the American College of Rheumatology diagnostic criteria (1990) (17). Superimposed headache exacerbations, mean pain score (0–10 score), and acute medications overused (Table 1) were analysed. Acute medications were divided in groups (triptans, NSAIDs, analgesics, none).
Age, sex, pain scores, exacerbation frequency, acute medication overused, and fibromyalgia diagnosis in chronic migraine patients

FIBRO, fibromyalgia diagnosis; n, without fibromyalgia.
Control CSF specimens were also obtained from 20 age- and sex-matched subjects who underwent lumbar puncture for other diagnostic purposes. In all these subjects CSF and blood examinations and, if necessary, instrumental investigations, including neuroimaging, excluded CNS diseases (multiple sclerosis, vasculitis, and other autoimmune diseases affecting the CNS), or systemic diseases (diabetes, renal or hepatic dysfunctioning, inflammatory diseases). Neurodegenerative diseases were also excluded.
The study protocol was approved by the local Ethics Committee, all patients gave written consent to the study. All patients were in pain at the time of lumbar puncture.
CSF analysis
Sodium phosphate dibasic (Na2HPO4), methanol (HPLC grade), trichloroacetic acid and sodium bicarbonate were purchased from Merck. Sodium tetraborate, beta-mercaptoethanol (BME), phosphoric acid (85%, HPLC grade), o-phthaldialdehyde (OPA),
Chromatography
The chromatographic system, from Waters, consisted of a Model 600E multisolvent pump; a 717 plus autosampler and a 2475 multifluorescence detector (excitation 330 nm, emission 450 nm). The CSF samples were deproteinized with 10% trichloroacetic acid (1 : 0.2 v/v). The resulting mixture was kept at 0°C for 15 min and then centrifuged at 3000 g for 10 min at 4°C. Supernatant (100 µl) was added to 400 µl of 0.2
Statistical analysis
All values were expressed as mean ± SD. One-way within-subjects
Results
Chemical analysis of the CSF normal protein, glucose, and lactate levels. Cell count was also normal.
CSF Glutamate levels were significantly higher in CM than controls (P < 0001) (Fig. 1). No differences were found when female and male patients were compared. Age did not correlate to glutamate levels. Mean pain score correlated with CSF glutamate levels (r = 0.551, P = 0.012). Superimposed headache exacerbation frequency did not correlate with glutamate levels.
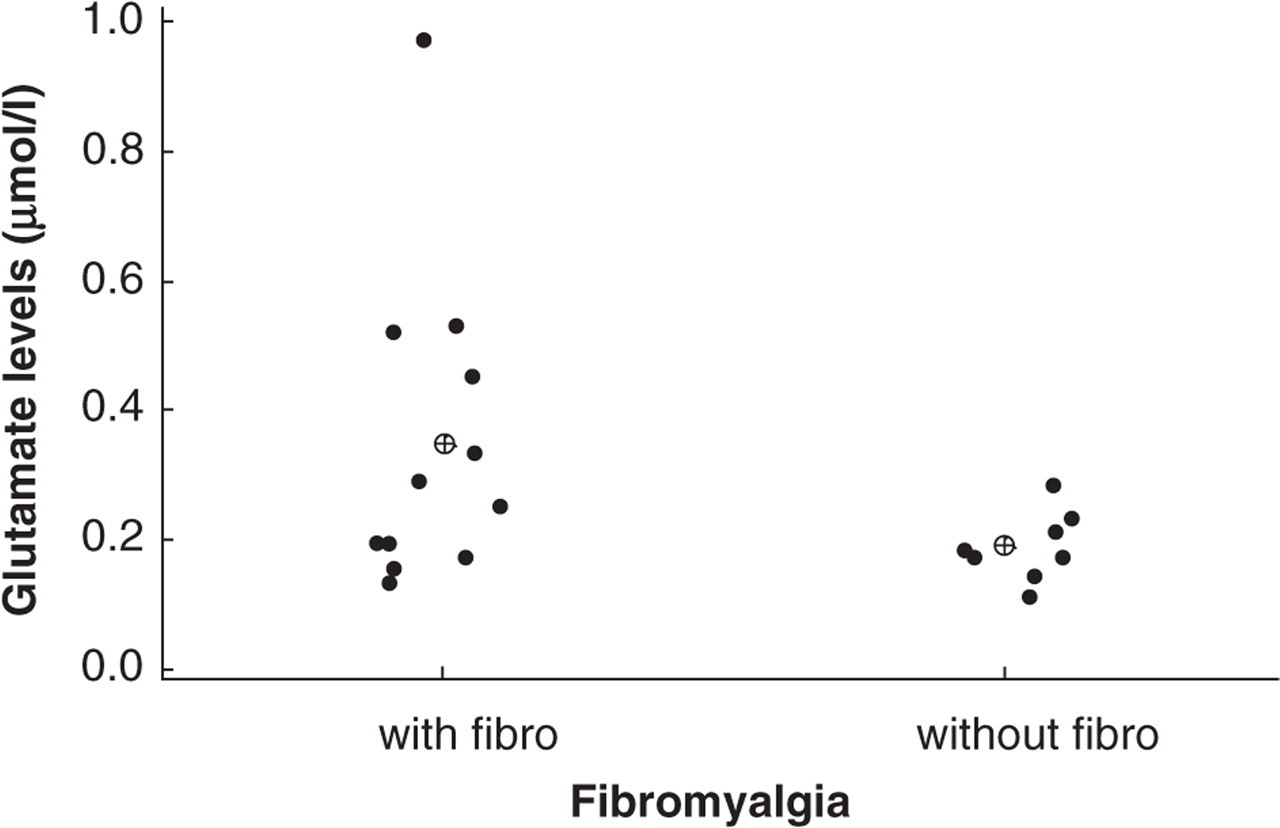
CM patients with fibromyalgia (fibro) had significantly higher CSF glutamate levels (µmols/l) than patients without fibromyalgia (wo fibro).
CM patients with fibromyalgia had significantly higher CSF glutamate levels than patients without fibromyalgia (0.34 ± 0.27 vs. 0.19 ± 0.06 µmol/l) (P < 0.04).
Both groups had higher levels than controls P < 0.001) (Graphic 1). No differences were found when acute medication groups (triptans, NSAIDs, analgesics, none) were compared.
Discussion
Our study shows increased glutamate levels in the CSF of chronic migraine patients compared to controls. More important is the new finding of even higher levels of glutamate in chronic migraine patients with fibromyalgia compared to those without fibromyalgia.
Previous studies showed abnormal glutamate levels in migraine patients in plasma (8, 9, 19–23), CSF (8–10) and platelets (20, 21). Ferrari et al. (19) demostrated that between attacks, migraineurs (notably with aura) had substantially higher plasma glutamate and aspartate levels than did controls and tension headache patients. During migraine attacks, glutamate (and to a lesser extent aspartate) levels were even further increased. This research group hypothesized a defective cellular (neuronal/glial) reuptake mechanism for glutamate and aspartate in migraineurs. Alam et al. (23) also found plasma glutamate was increased in migraine but not tension-type headache patients. Cananzi et al. (21) evaluated plasma and platelet glutamate levels finding higher levels in both migraine with and without aura.
Zukerman et al. (8) studied CSF glutamate levels in 10 episodic migraine patients, six diagnosed with migraine with aura, and four migraine without aura, showing an increase in glutamate levels. Martinez et al. also found similar results (9). Gallai et al. (10) reported a significant increase in CSF glutamate levels in chronic daily headache patients compared to controls. Rothrock et al. (24) found the levels of CSF taurine, glycine and glutamine significantly higher in migraine patients, without significant differences among three migraine subgroups coined as infrequent migraine, frequent migraine and transformed migraine.
Head pain in migraine arises within the trigeminal system. Central trigeminal neurons that receive convergent input from external stimuli may be sensitized. The mechanism of central sensitization has been implicated in migraine pathogenesis. Patients frequently offer evidence for central sensitization of the trigeminal system during migraine attacks, such as pain returning on head movement or scalp pressure after attacks have subsided, allodynia of the head, and even allodynia and pain of the upper trunk and limbs that suggests supraspinal origins of sensitization. Central sensitization may account for the severe pain of migraine headache, in this study we showed pain intensity correlated with CSF glutamate levels, providing evidence that glutamate levels, central sensitization and pain intensity are linked.
Patients’ drug treatments may have influenced the CSF glutamate levels, however, we could not find significant difference in the acute medication subgroups. One cannot exclude the possibility that acute medications might play a role in glutamate levels because the consumption profile and the small number of patients did not provide sufficient statistical power for the analysis.
It has been hypothesized that migraine is associated with a state of central neuronal hyperexcitability, involving overactivity of the excitatory amino acids, glutamate, and possibly aspartate (25). This theory may also be applied in the comorbidity between migraine and fibromyalgia. A low brain magnesium and consequent reduced gating of glutamatergic receptors (26) could be another possible link between migraine, fibromyalgia and the mechanisms of glutamate hyperactivity, neuronal hyperexcitability, and susceptibility to glutamate-dependent spreading depression.
Burstein (27) has proposed that: (a) sensitization of both peripheral and central trigeminovascular neurons accounts for the intracranial hypersensitivity observed in migraineurs, i.e. the worsening pain during coughing, bending over, rapid head movement, and the throbbing nature of migraine pain, and (b) sensitization of central but not peripheral trigeminal neurons is responsible for the extracranial hypersensitivity (extracranial tenderness and cutaneous allodynia).
Further evidence of central hyperexcitability has been observed in a study of cutaneous allodynia during migraine in humans (28). Seventy-nine percent of patients experienced this effect during spontaneous headaches, with or without aura. Of those with allodynia, 85% reported it outside the referred pain area, on the ipsilateral side. An allodynic response on the contralateral side of the head or either forearm cannot be explained by peripheral sensitization alone; at least third-order neurons must be involved. However, only 33% of allodynic patients experienced allodynia at all sites tested. Therefore, it has been postulated that the increased sensitivity is due not to a general neuronal hypersensitivity, but to hyperexcitability in the central trigeminal pathway after its activation during migraine.
The study did not mentioned the association of fibromyalgia and migraine, however, tender points, the hallmark of fibromyalgia, can be considered as pressure allodynia. Our study shows this is probably mediated by central sensitization, with increase in CSF glutamate levels. We postulate chronic migraine patients with fibromyalgia, in addition to have more disabling headaches (6), suffer from a more severe central sensitization process. This subtype of patients need more agressive therapy. They may respond to medications acting on glutamate, such as topiramate, lamotrigine, and glutamate antagonists, opening a new therapeutic opportunity for the treatment of migraine associated with fibromyalgia.