
Abstract
Cluster headache is the most severe of the primary headaches. Positron emission tomography and functional MRI studies have shown that the ipsilateral posterior hypothalamus is activated during cluster headache attacks and is structurally asymmetric in these patients. These changes are highly specific for the condition and suggest that the cluster headache generator may be located in that brain area; they further suggest that electrical stimulation of that region might produce clinical improvement in chronic cluster headache sufferers refractory to medical therapy. In five patients with severe intractable chronic cluster headache, hypothalamic electrical stimulation produced complete and long-term pain relief with no relevant side-effects. We therefore consider it essential to propose criteria for selecting chronic cluster headache patients for hypothalamic deep brain stimulation before this procedure is undertaken at other academic medical centres.
Introduction
Cluster headache (CH) is excruciatingly painful (1, 2). The intractable chronic form of CH is rare, nonetheless it constitutes a major clinical problem. These patients are often subjected to destructive neurolytic procedures of the sensory trigeminal nerve (3); however, these procedures are characterized by high rates of recurrence and potentially severe side-effects including facial sensory loss, facial dysesthesias, anaesthesia dolorosa, corneal anaesthesia, corneal ulceration and loss of vision (4). Lack of understanding of the mechanisms giving rise to CH has hampered the development of new treatments. The typical seasonal recurrence of cluster periods and the occurrence of the attacks at fixed times of the day or night strongly suggested involvement of a hypothalamic pacemaker (5, 6). Neuroendocrinological studies on circadian rhythms of hypophyseal hormone systems, particularly melatonin (7, 8), have uncovered anomalies implicating hypothalamic dysfunction in CH (9). More recently, positron emission tomography (PET) and functional MRI studies have demonstrated that the ipsilateral posterior inferior hypothalamus is activated during CH attacks and is structurally asymmetric in CH patients (10, 11). These changes are highly specific for CH and are not seen on PET during acute migraine attacks, experimental first-division trigeminal pain, or in CH patients given nitroglycerine during a remission phase (12, 13). Activation in ipsilateral postero-inferior hypothalamus was however, reported in other types of clinical (14) and experimental pains (15, 16). There is nonetheless converging evidence from these clinical, neuroendocrinological and neuroimaging observations that the hypothalamus is pivotal in generating cluster headache (10), which would be the first time that a lesion site seems to have been identified for a primary headache.
Knowledge of the neuronal circuitry involved in movement disorders established the rationale for the use of deep brain stimulation (DBS) with stereotactically placed electrodes to treat these patients when drugs are no longer effective (17, 18). Consequently, identification of hypothalamic alterations in CH led to the suggestion that electrical stimulation of that region might produce clinical improvement in otherwise treatment refractory patients. Following the successful use of DBS to treat a patient with severe intractable chronic CH (CCH) who had previously undergone ablative trigeminal surgery (19), we published data on a further four patients, all with highly positive outcomes and negligible side-effects (19–21), and are following another three CCH patients more recently treated by this method (22). We therefore consider it essential to propose criteria for selecting chronic CH patients for hypothalamic DBS prior to this procedure becoming more widely utilized. Because the hypothalamus is important for internal metabolic homeostasis and circadian rhythms, and long-term hypothalamic stimulation has not previously been used in humans, we believe that extremely cautious patient selection, close postoperative monitoring of implanted patients, are mandatory for patient safety.
Commentary
Table 1 shows our proposed eligibility criteria for hypothalamic DBS in CCH diagnosed according to IHS criteria.
Criteria for electrode implants in intractable chronic cluster headache

The operation should be considered only in patients with CCH for at least two years, generally with daily or almost daily attacks
Our reasoning for this proposal is that from a clinical point of view, two years is sufficient to apply the full range of available CH prophylactic medications (23, 24), including recent open-label experience with therapies such as valproate, topiramate and gabapentin (25). Furthermore, first-line treatments such as verapamil (26) may need gradual titration to dosages as high as 960 mg/day (27), while others, such as gabapentin, may be effective when used as add-on therapy (25). It is also necessary to follow the patient for sufficient time to be certain that a remission period does not occur spontaneously.
Attacks must be strictly unilateral for at least 12 months
At present, we consider it advisable to consider DBS only in patients with strictly unilateral CH (no side shift), since contralateral attacks are well known to develop in CH patients after ablative trigeminal procedures. Bilateral DBS should not be considered until more experience on unilateral DBS has been accumulated.
Patients must be hospitalized to witness attacks and document their characteristics
We believe it important to closely monitor the patient over a period to verify the diagnosis and assess the crises at first hand.
Candidates must be psychologically stable with a normal psychological profile
We recommend that neuropsychological tests be administered before the operation and periodically afterwards.
No medical/neurological contraindications to DBS
Since the hypothalamus is involved in numerous important functions, we suggest, at the present state of knowledge, that the contraindications listed in item six of Table 1 should be adhered to.
Normal neuroimaging including cranial MRI with gadolinium, cranio-cervical transition and MRI arterial and venous angiography and CT of the skull base
It is important to exclude any intracranial abnormality that may contraindicate DBS or which could be a potential underlying cause of CH (28). Due to limited experience we do not recommend DBS in symptomatic CH, even if the pathology is distant to the site of stimulation.
Hypothalamic DBS and fertility
The effects of hypothalamic stimulation on pregnancy are completely unknown and for this reason we recommend pregnant patients should not receive DBS. Patient must be informed that continuous hypothalamic stimulation might have effects on fertility and sexual behaviour, although this aspect has not been studied.
Smoking and drinking alcohol
Both these activities, when stopped, may help transform a chronic form of cluster headache into an episodic one.
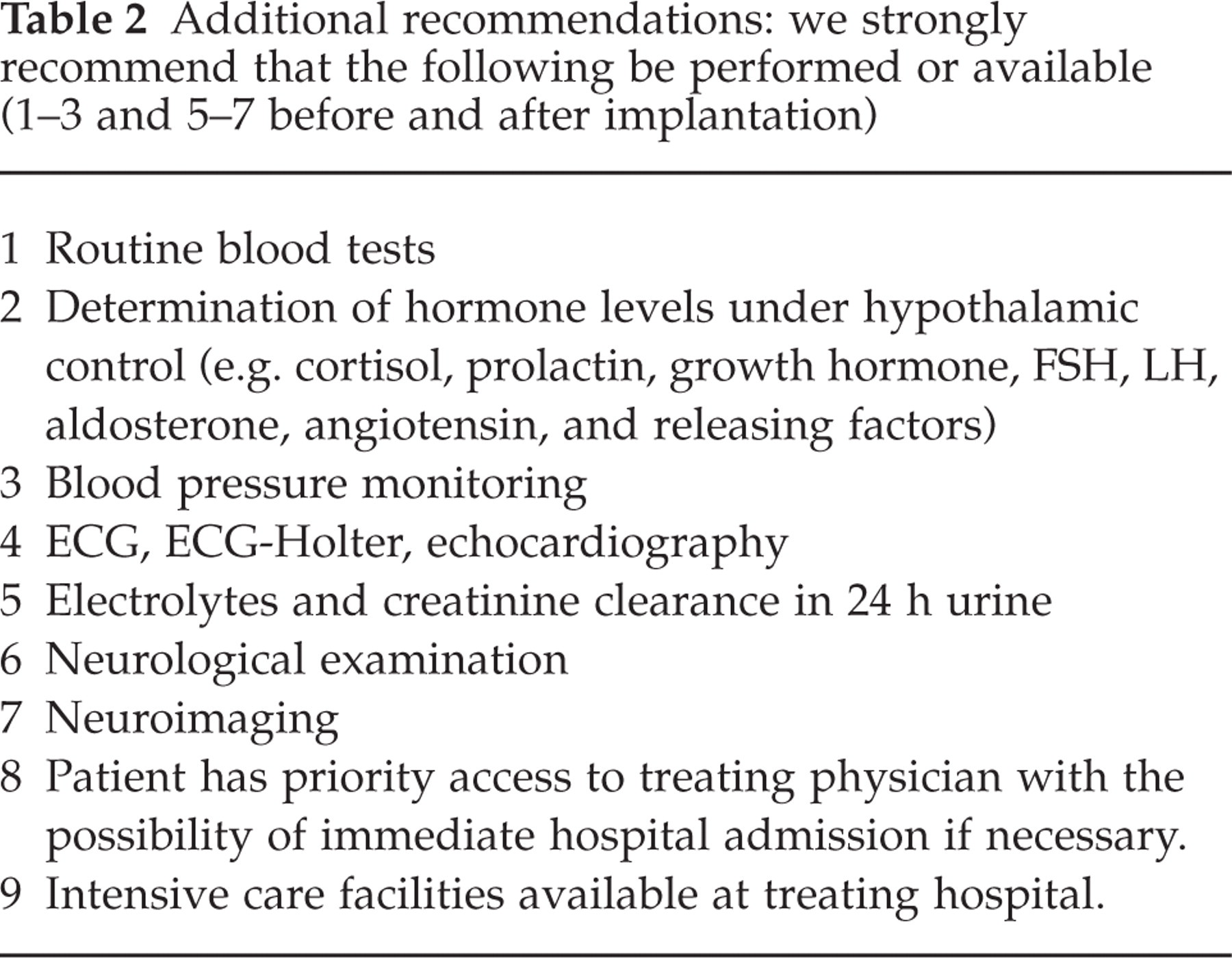
Further recommendations are listed in Table 2.
Additional recommendations: we strongly recommend that the following be performed or available (1–3 and 5–7 before and after implantation)
Other
(a) After electrode implantation, the stimulator should not be switched on before another typical spontaneous CH attack has occurred.
(b) We recommend that the stimulator be switched off after each attack-free period of three months. This should only be done with the patient's consent, however, the patient should be blinded to this procedure. The stimulator should be switched on again only after a spontaneous attack occurs.
Electrode targeting
The use of DBS for the treatment of intractable movement disorders is well established and possible targets clearly identified. For tremor, correct electrode positioning is ensured by intraoperative stimulation which eliminates or minimizes the symptom. For DBS in CCH, there is at present no objective means of determining intraoperatively whether the electrode has reached the exact hypothalamic site indicated by May et al. (13) – which in any event is only an average estimation over several patients. Targeting with high resolution PET may be possible in the near future. To ensure the most accurate electrode localization, we adapt the coordinates given by May et al. (13) to each patient, using a series of anatomical and functional reference points obtained from previous stereotactic operations; these points are used to compile an anatomical-functional atlas which provides each patient with personalized stereotactic coordinates that offer the greatest probability of safely reaching the target (19–22). Obviously the position of the electrode has to be checked by postoperative MRI. Further studies are required to identify intraoperative techniques which ensure that the electrode placed in its hypothalamic target.