
Abstract
We investigated the prevalence and clinical characteristics of tension-type headache (TTH), psychosocial factors contributing to the onset and aggravation of headache and coping mechanisms of individuals in a young population in Turkey. The sample consisted of 2226 university students, aged 7 to 21 years old. A self-administered questionnaire inquiring about epidemiological and clinical features of headache was filled out by participants. TTH diagnosis was determined in accordance with the International Headache Society Criteria of 1988. The prevalence of TTH was 20.35% (25.54% for women and 14.25% for men). 43.7% of headache sufferers had one or more stressful life events before the onset of headache and stress was the most frequent aggravating factor of headache (52%). Resting (58.1%) was the most common coping style. In conclusion, TTH is not a rare condition in Turkish young people and psychosocial factors are always taken into consideration for diagnosis and treatment of TTH.
Introduction
Tension-type headache (TTH) is a primary headache syndrome and affects many headache sufferers. In addition to the significant impact on the quality of life of the sufferers, it causes a socio-economic burden due to missed work or reduced efficiency (1). Although TTH is a common condition, the pathophysiology and mechanism remain unclear. It has been suggested that the derivative pain of tension-type headaches has a muscular origin and this muscular pain tends to be dull and achy, poorly localized and radiating (2). On the other hand, it is widely accepted that psychological factors have a significant influence on headaches. It has been proposed that psychological factors are provoking agents, consequences of returning intense pain and personality traits, and that they predispose some people to headaches (3).
There are many studies on the prevalence of TTH conducted in different countries with a variety of methodologies. According to these studies, the prevalence of TTH has been found over a range from 1.3% to 65% in men and 2.7% to 86% in women (4–9). However, it is useful to find its prevalence rate in certain age groups. Epidemiological studies show that the prevalence of TTH in a young population also varies from one study to another in a range from 5.9% to 34.5% in men and 11.1% to 40.8% in women (7, 10, 11).
In 1997, on the basis of the International Headache Society (IHS) criteria (12), an epidemiological headache study was conducted throughout Turkey. The sample consisted of 2007 participants from different regions of Turkey, aged between 15 and 55 years old. According to the results of this study the prevalence of TTH was 31.7% (31.3% for women; 32.1% for men) (13). However, there is no epidemiological study on the prevalence of TTH in young Turkish people. Therefore, the main aim of this study was to investigate the epidemiological and clinical characteristics of TTH in a young population, aged 17–21 years. Possible psychological factors which affect the onset and course of headache and coping mechanisms of individuals were also evaluated.
Method
The subjects were 2226 students, aged 17–21 years enrolling in different faculties of Istanbul University, Turkey. Turkish state universities are free and entrance is controlled by University Entrance Examination which requires hard-work and preparation in previous years. During the 3-day enrolment period, there were 3000 students to enrol in their faculties who had just passed this examination. Of 3000 students we reached 2591 (86%). The content and the aim of the study was explained to the students and they were asked if they would like to participate in it. After an exclusion process which is presented in the ‘results’ section, 2226 students remained. A self-administered questionnaire was filled in by all participating students. This questionnaire consisted of 20 questions inquiring about the frequency, intensity, duration, location, associated symptoms and aggravating factors of headache, familial features, previous diagnoses and medications, restricted activities and coping mechanisms. The questionnaire also included questions relating to migraine which helped to exclude any migraine (with and without aura) and mixed headache cases (aura symptoms such as blind spots, flashing lights or zig zag patterns, and unilateral numbness and/or tingling prior to severe pain, and unilateral location). The diagnosis of TTH was made in accordance with the International Headache Society (IHS) criteria (12). Verbal informed-consent was obtained for the all participants. Data analysis was done by using χ2 test.
Case definition
Diagnosis of TTH was made only in those meeting the IHS criteria for episodic and chronic TTH.
1. Episodic TTH (ETTH) was diagnosed according to this algorithm constructed using the IHS criteria, with headaches having at least two of:
Bilateral pain, pressing or tightening quality, mild or moderate intensity, no increased pain with physical exertion;
More than 10 episodes of headache (fewer than 15 days in a month, lasting between 30 min and 7 days).
Neither nausea nor vomiting;
Phonophobia or photophobia were absent, or only one was present but without the other.
2. No positive response to questions related to migraine.
Chronic TTH (CTTH) criteria were identical to those for ETTH except that the attack frequency was 15 or more attacks per month for at least 6 months and 1 associated symptom of nausea, phonophobia, or photophobia was permitted.
Results
There were 3000 students to enrol in their faculties. Of 3000 students we reached 2591 (86%). Of these students 2425 (93%) agreed to participate and filled in a self-administered questionnaire. To protect the homogenity of the sample and to focus on a specific age group 127 of 2425 students aged > 21 years (range 22–43 years) were excluded from the study. Seventy-two students returned questionnaires only giving their socio-demographic information and no other answers. They were also excluded. The final number of students in our sample was 2226 (1024 men, 46%; 1202 women, 54%; age range 17–21 years).
Prevalence of TTH
Four hundred and fifty-three students were diagnosed as having TTH according to the IHS criteria (146 men, 32.2%; 307 women, 67.8%). The prevalence of TTH was 20.35% (14.25% for men; 22.71% for women). The mean (± SD) age was 18.3 ± 0.73 years (range 17–21 years). Table 1 shows the prevalence of episodic and chronic TTH in both sexes.
Prevalence of TTH in Turkish college students

Clinical characteristics of TTH
Table 2 shows clinical characteristics of TTH. Two hundred and twelve (49.4%) of 429 students with TTH reported the same type of headache in other family members.
Clinical characteristics of TTH

More than one feature may be listed per individual.
Values of ‘N’ less than 453 indicate that not all students answered this question.
Previous diagnoses for headache in students with TTH were migraine (n = 7, 1.8%), psychogenic (n = 18, 4.6%), sinusitis (n = 22, 5.6%), tension-type headache (n = 5, 1.3%) and others (n = 9, 2.3%). Three hundred and thirty (84.4%) of 391 students had no previous diagnosis.
One hundred and ninety-six (47.6%) of 412 headache sufferers reported that they had not used any analgesic medication for their headache. Of the 216 (52.4%) students using analgesic medication, 95 students (23.1%) reported complete relief and 106 students (25.7%) some relief in pain. In 15 students (3.6%) there was no relief in pain despite the analgesic use.
Disabilities due to headache were reported by 10.2% of headache sufferers for physical activity, 11.9% for social activity, 11.3% for self-care and 12.4% for academic performance. Table 3. shows predisposing and aggravating factors of headache and coping styles of headache sufferers.
Predisposing and aggravating factors of headache with coping styles of students with TTH
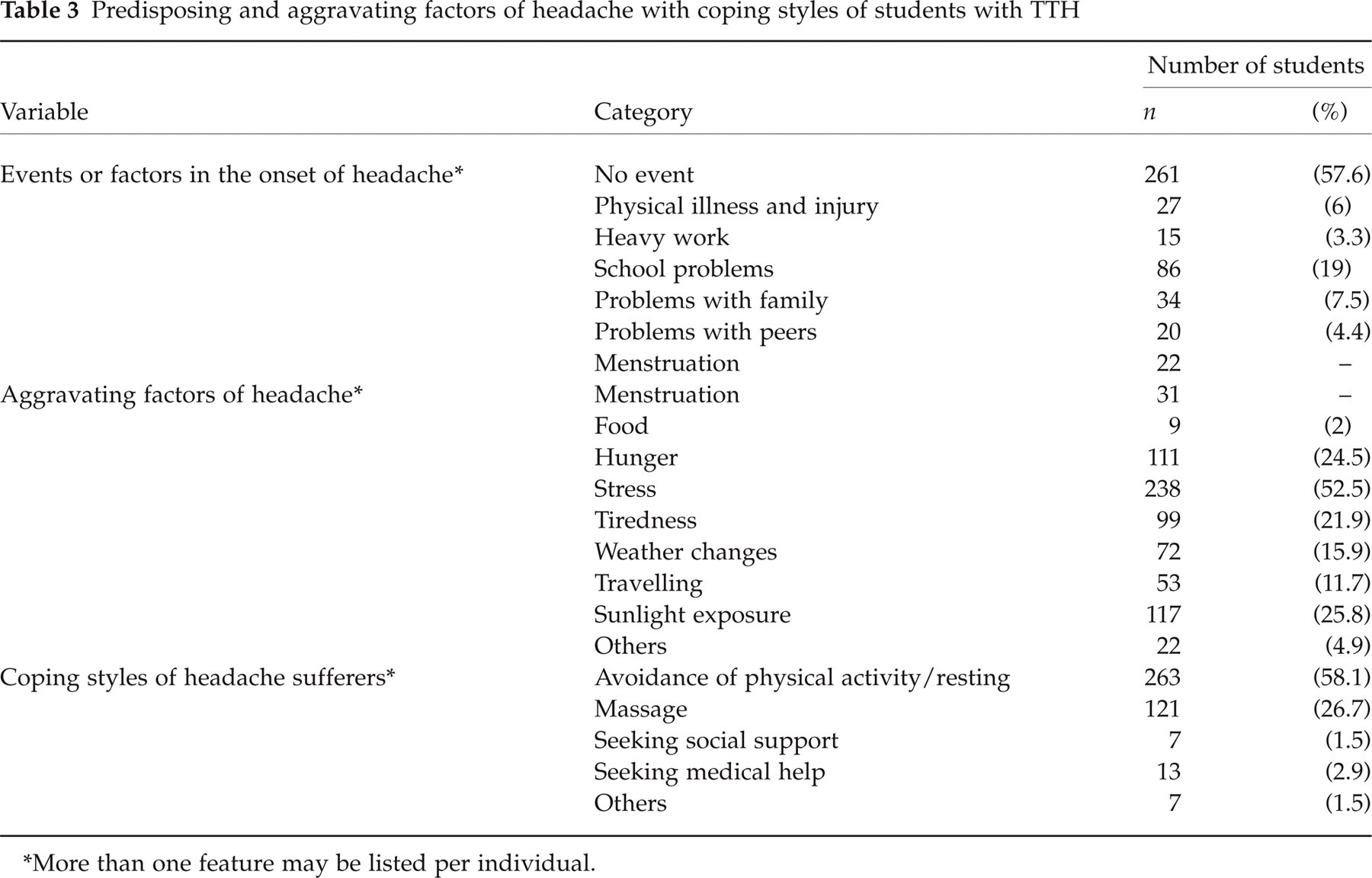
More than one feature may be listed per individual.
Discussion
In this study we aimed to investigate the prevalence, clinical characteristics and psychosocial aspects of TTH in a student population, aged 17–21 years. Eighteen percent of subjects fulfilled the IHS criteria completely for ETTH and 1.88% fulfilled the criteria of CTTH. The Headache Research Group using the IHS criteria investigated the epidemiology of headache in Turkey, in 1997 (13). The sample consisted of 2007 participants from different regions of Turkey, aged between 15 and 55 years old. The prevalence of TTH in this study was 31.7% (31.3% for women; 32.1% for men). The prevalence of TTH varies over a wide range from 1.3% to 65% in men and 2.7% to 86% in women (4–9). Our prevalence rate is lower than those reported in most other studies, including the study which was conducted in Turkey. There could be some explanations for this discrepancy. First, most of the other studies were conducted on a wide range of age groups, generally 15–65 years (5–7,9, 13). This study included only a very young population aged 17–21 years. However, the prevalence of TTH was 12.2% (11.1% for women; 13.9% for men) in a study of Deleu et al. (11) in medical students, aged 18–26 years, in Oman. In a similar student population, aged 22–27 years in Athens, the prevalence of TTH was 9.5% (5.9% for men; 13.7 for women) (10). In both sexes, the prevalence of TTH seems to peak between the ages 30 and 39 and then decline with age and the most common onset of TTH is in the second decennium (1). Therefore, this lower prevalence rate may be specific for this age group. Second, the study design and methodology could affect the prevalence rate of TTH. We used a self-reported questionnaire and there was no following clinical interview or neurological examination. For this reason we applied the strict IHS diagnostic criteria to the population and used a clear-cut case definition. It has been recently argued that the IHS criteria for the diagnosis of TTH is generally more specific and less sensitive, leading to high false negatives and an underestimation of the true prevalence of the condition (14–16). Third, there may be cultural, regional and genetic differences for the prevalence of TTH. Generally, the prevalences of both migraine and TTH are higher in western cultures (5, 7, 9) than those in eastern cultures (4, 17) and our findings are similar to the results of eastern cultures.
A female preponderance (female/male ratio: 2.1) in the prevalence of TTH in this study is in accordance with results of other prior studies (8).
Sixty-eight percent of TTH sufferers had suffered the headaches for 6 months or longer suggesting that TTH tends to be a chronic condition. The most frequently reported symptoms about localization (forehead, 47.4%) (11), frequency (fewer than 3 per month, 70.6%) (6, 7), intensity (mild, 67.5%; moderate, 29.4%; severe, 3.1%) (11) and associated symptoms (phonophobia, 45%) (8) of headache in this study are consistent with the findings of previous studies. Unlike other studies (2), throbbing pain was the most frequent pain quality followed by pressing (26.3%) and tightening (15%) in this study. This result is similar to the finding of another study (8) suggesting that throbbing pain may be an important feature of TTH.
About half of students with TTH (49.4%) reported the existence of the same type of headache in other family members, a similar result found in other studies (11). This finding may reflect genetic effects in the aetiology of TTH.
A total of 52.4% of headache sufferers reported using analgesics for their headaches. This rate is lower than that found in another study (11). Eighty-four percent of the subjects with TTH had never contacted any health-care facilities for their headaches. Additionally, only 2.9% of headache sufferers sought medical help during their headache attacks. These findings show that the utilization of medical services was not common in this study population, confirming the fact that TTH is an under-treated condition (1, 18).
Disabilities due to headache were reported by 10.2% of headache sufferers in physical activity, 11.9% in social activity, 11.3% in self-care and 12.4% in academic performance. These values are lower than those in prior studies (5, 8).
Fifty-eight percent of subjects with TTH reported no stressful life event prior the onset of headache. The rest of students reported one or more psychosocial factors in the onset of their headaches. The most frequent psychosocial factors were academic problems (19.1%) and problems within the family (7.5%). A higher frequency of stressful life events in the onset of headache has been found in other headache studies (19–21). In a study of adolescents with chronic daily headache, the majority of cases reported the onset of headache within 1 years of a major loss in the family, such as divorce or death (22). Psychosocial stress may contribute to the onset of headache both directly or by facilitating mood, anxiety or somatoform disorders (23). Because our study group is a student population, academic problems as the most frequent predisposing factor may be a relevant result for this group. According to other previous studies conducted in adolescents, problems and stress at school are commonly put forward as predisposing or trigger factors of headache (24, 25). Young headache patients spend more time on their homework, have difficulty in relaxing, and are more often tired after school than headache-free controls (26–28).
The most frequently reported aggravating factor of headache in students with TTH was emotional problems and stress (52.5%), following by sunlight exposure (25.8%), hunger (24.5%) and physical exertion (21.9%). Stress as a most common precipitant has been found in other studies (11, 17) and it triggers up to 80% of tension-type headaches (18). Emotions have biochemical effects in the body, and mental stress alone can elicit muscle contraction through the limbic system (18).
The two most common coping mechanisms of headache sufferers were resting/avoidance of physical activity (58.1%) and massage (26.7%). Active coping mechanisms like seeking medical help were used by only 2.9% of headache sufferers. A total of 1.5% used social supports. These results show that our study population had less effective coping strategies to manage their pain. Studies have demonstrated that patients with tension-type headache have similar major stressful life events but perceive more events as ‘hassles’ and have less effective coping strategies (e.g. avoidance, self-criticism, lack of use of social supports) (29).
In conclusion, in this first study focusing on the epidemiology of TTH in a large, young Turkish population, the prevalence of TTH was 20.4%. Study design was a self-administered questionnaire, and there were no clinical interview or examination, but we used a clear-cut case definition to increase the reliability. Clinical characteristics of TTH were similar to those found in other studies. Psychosocial factors were important features of TTH in this study. A significant portion of headache sufferers (43.7%) had one or more stressful life events before the onset of headache and for more than half of the headache sufferers stress was the most common aggravating factor of their headaches (52%). Besides, headache sufferers had passive coping styles to manage their headaches. Finally, tension-type headache is not a rare condition and psychosocial factors are always taken into consideration for diagnosis and treatment of tension-type headache.
Footnotes
Acknowledgements
Special thanks to Dr Suleyman Ozyalcin from the Division of Algology, Department of Anesthesiology, Istanbul Medical Faculty, Istanbul University, for his assistance in setting up the study and providing the sample group.