
Abstract
The aim of this study was to investigate whether chronic daily headache (CDH) and temporomandibular disorders (TMD) patients present with different psychological and sleep quality characteristics. Sixty-seven patients diagnosed with CDH, according to classification criteria from Silberstein et al., were matched by age and sex with 67 patients who had a primary diagnosis of myofascial pain (MP) and 67 patients with a primary diagnosis of TMJ intracapsular pain (IC) according to the Research Diagnostic Criteria for TMD. The CDH group was comprised of three mutually exclusive diagnostic groups: chronic migraine (n = 35); chronic tension-type headache (n = 26); ‘other CDH’ (n = 6). All patients completed a battery of psychological and sleep quality questionnaires. All CDH subgroups showed similar psychological and sleep quality profiles. Pain intensity and duration were controlled in the multivariate analyses (M
Keywords
Introduction
Temporomandibular disorders (TMD) represent a collective term embracing a number of clinical problems that involve the masticatory muscles, the temporomandibular joint (TMJ), or both (1). TMJ dysfunction is frequently described as an achy, sharp pain, localized in the preauricular area, accompanied by clicking, crepitation, and catching or locking of the TMJ. Masticatory muscle pain is described as a diffuse, dull pain in and around the jaw-muscle area. TMD are generally aggravated by jaw function and may also be associated with symptoms such as facial pain, headache, otalgia and cervical pain.
Chronic daily headache (CDH) has been defined by several authors as a constant experience of head pain lasting no less than 4 h for more than 15 days per month (2). CDH is therefore not a specific clinical entity but rather a descriptive term comprising various primary headache entities such as chronic migraine and chronic tension-type headache. Even though relatively infrequent in general practice, CDH is the major reason for consultation in headache specialty clinics. CDH is estimated to affect around 4% of the general population and defines a group of patients that require distinct diagnostic and management needs (3). Although not life threatening, CDH can often be incapacitating with a substantial impact on the patient's social life and work performance.
Despite the extensive amount of studies addressing primary headache and TMD comorbidity (4, 5), studies investigating psychological and sleep quality differences between TMD and CDH populations are scarce in the literature (6). Additionally, no studies examining these issues have been published that have controlled for pain duration and intensity. Consequently, more studies are needed to determine whether psychological and sleep quality differences between TMD and CDH are the result of pain intensity and duration effects or the consequence of true psychological and sleep quality differences between these pain populations. This study is directed towards these unanswered questions.
Materials and methods
During the study period, a total of 100 consecutive adult headache patients were seen at the Orofacial Pain Center of the University of the Kentucky Dental School. Prior to the initial examination, all patients completed an orofacial pain questionnaire and a battery of psychological questionnaires. The psychological questionnaires included the Symptom Check List-90-Revised (SCL-90-R), the Pittsburg Sleep Quality Index (PSQI), the PCL-C questionnaire, and the Multidimensional Pain Inventory (MPI). These questionnaires cover a wide range of symptoms and behaviours that are important in the development of a comprehensive treatment/management plan for the patient.
The examinations were conducted by dentists with advanced training in the diagnosis of orofacial pain conditions. No formal reliability data were collected, but all examiners were trained in the Orofacial Pain Center of the University of Kentucky within the guidelines of the American Academy of Orofacial Pain (1). The information obtained provided the basis for primary and secondary diagnoses. The IHS classification criteria (7) were used for headache diagnoses except in those patients who fulfilled the criteria for chronic daily headache (CDH) (number of headache days was > 15 days/month, and > 4 h/day). Correspondingly, patients who fulfilled the criteria for CDH were diagnosed according to the revised IHS criteria for CDH proposed by Silberstein et al. (2). The patients were classified, on the basis of their history and clinical examinations, as suffering from CDH (n = 67) and ‘other’ headaches (n = 33). Subsequently, only patients fulfilling a diagnosis of CDH were selected for the study. Patients presenting two or more headache diagnosis (i.e CDH and TMD) were included in the ‘other’ headaches group and therefore were excluded from the study. CDH patients were diagnosed into three mutually exclusive diagnoses, that is, chronic migraine (n = 35), chronic tension-type headache (n = 26), and ‘other CDH’ (n = 6). The ‘other CDH’ group was comprised of patients who had a diagnosis of either hemicrania continua (HC) or new-daily persistent-headache (NDPH). Since an indomethacin test was not performed in these patients (all presented unilateral headaches), a differentiation between HC and NDPH was not possible. Consequently, the ‘other CDH’ patients were diagnosed as having a CDH not fulfilling criteria for either chronic migraine or chronic tension-type headache.
The CDH patients (n = 67) were matched by age and sex with 67 patients seen in the Orofacial Pain Center with a primary diagnosis of masticatory myofascial pain (MP) and 67 patients with a primary diagnosis of TMJ intracapsular pain (IC) according to the Research Diagnostic Criteria (RDC) for TMD (8). The IC group was composed of patients diagnosed with TMJ disc displacement with reduction (RDC group IIa), TMJ disc displacement without reduction with or without limited mouth opening (RDC group IIb and IIc), TMJ arthralgia (RDC group IIIa), and/or osteoarthritis (RDC group IIIb). All patients with a diagnosis of TMJ disc displacement had TMJ arthralgia or osteoarthritis as a secondary diagnosis. The MP group was composed of patients diagnosed with MP without limited mouth opening (RDC Ia), and MP with limited opening (Ib). MP patients with a secondary diagnosis of TMJ pain, and TMJ pain patients with a secondary diagnosis of MP, were not selected for this study. Additionally, MP and IC patients presenting other forms of headache (IHS classification criteria) as a secondary and/or tertiary diagnosis were also excluded from the study. The patient's data were collected following the same clinical and diagnostic procedures as for the headache patients.
Subjects
The overall patient population was comprised of 201 subjects (CDH: n= 67; MP: n= 67; IC: n= 67). The patients were between 18 and 69-year-old-with a mean age of 36.5 years (SD = 11.4). The overall sample was 81% female, with 54 females and 13 males in each group (CDH, MP, IC). There was no significant difference in age between the three diagnostic groups, F (2, 199) = 0.018, P= 0.982).
Physical measures
The physiological measures of systolic blood pressure (SBP), diastolic blood pressure (DBP), and heart rate (HR) were recorded using a Paramed 9200 automated blood pressure cuff. The cuff was placed on the patient's left arm.
Psychological measures
The SCL-90-R (9) is a 90-item multidimensional self-report inventory that measures nine dimensions of psychological functioning, including somatization (SOM), obsessive-compulsive behaviour (OC), interpersonal sensitivity (IS), depression (DEP), anxiety (ANX), hostility (HOS), phobic anxiety (PHOB), paranoid ideation (PAR), and psychoticism (PSY). Test-retest reliabilities range from r = 0.78–0.90 for nonpatient samples, and internal consistencies range from 0.77 to 0.90.
The MPI (10) assesses pain severity, social and physical activities, affective distress, social support, and feelings of life control. It also classifies respondents into one of six categories: adaptive coper, dysfunctional, interpersonally distress, hybrid, anomalous, and unanalysable. Test-retest reliabilities of scale scores range from r = 0.68–0.86, and internal consistencies range from 0.73 to 0.90.
The PSQI (11) requests information regarding the number of hours spent in bed and asleep, frequency and reasons for awakening, and difficulty returning to sleep after awakening. The PSQI has been shown to be a valid and reliable assessment to overall sleep quality and disturbance, with good test-retest reliability (r = 0.85) and internal consistency (α= 0.83).
The PCL-C (12) questionnaire is a 17-item measure designed to assess symptoms of Post-Traumatic-Stress-Disorder (PTSD). Patients are asked to report problems or complaints they may have experienced in the last month in response to a stressful situation. Responses include, but are not limited to, flashbacks, distressing dreams, hyper-vigilance, impaired concentration, and avoidance behaviours. The PCL has exhibited test-retest stability (r = 0.96), good overall internal consistency (α= 0.92), and provides a valid and reliable assessment of the presence of PTSD symptoms.
The orofacial pain questionnaire asks patients to describe their pain experience using descriptors from the McGill Pain Questionnaire (13). These descriptors are divided into sensory and affective classifications. The sensory category contains terms such as throbbing, shooting, stabbing, and aching, while the affective category contains terms such as sickening, exhausting, and punishing.
Statistical analysis
Analysis of variance (
Results
Preliminary analysis
The CDH subpopulations (chronic migraine, chronic tension-type headache, and ‘other CDH’) that make up the CDH group for this study were analysed on a number of domains to determine if there were any significant differences between these diagnostic categories that might preclude grouping them together for further comparison with the MP and IC diagnostic groups. There were no significant differences between the CDH subpopulations on all psychological and sleep quality domain variables, including pain severity, pain duration, affect and sensory pain descriptors, psychological characteristics (SCL-90-R dimension scores, MPI scale scores), sleep quality scores, and post traumatic stress symptoms.
Pain severity and duration
Differences in pain severity were determined by comparing scores on the MPI pain severity scale between the groups. Mean pain severity for the groups was as follows: CDH group mean = 41.8, SD = 11.6; MP group mean = 43.7, SD = 10.8; IC group mean = 38.6, SD = 11.1. There was an overall significant difference between the three groups on pain severity, F (2, 199) = 3.68, P= 0.027). Post-hoc comparisons showed a significant difference between the MP and IC groups (P = 0.024), with no significant difference between the CDH group and the other two groups.
Pain duration was similarly tested between the groups. Mean pain duration for the groups was as follows (in months): CDH group mean = 74.7, SD = 96.2; MP group mean = 66.2, SD = 78.8; IC group mean = 42.1, SD = 54.2. There was a significant difference between the three groups on pain duration, F (2, 199) = 3.13, P= 0.046). Post-hoc comparisons showed a significant difference between the CDH and IC groups (P = 0.05), with no significant difference between the MP group and the other two groups. Due to the significant differences between groups on pain severity and duration, these variables were controlled for in the remaining multivariate analyses by treating them as covariates.
Affect and sensory pain descriptors
The descriptive terms used to differentiate between sensory pain experiences and affective pain experiences from the McGill Pain Questionnaire in the medical/dental history questionnaire were used to determine if there was a significant difference in how the three diagnostic groups classified their experience of pain. The sums of the number of affective descriptors and sensory descriptors endorsed by each patient were calculated and a comparison was made between the groups. There was a significant difference between the groups on number of affective descriptors endorsed, F (2, 199) = 7.49, P= 0.001. The CDH group endorsed more affective descriptors of their pain experience (M = 0.94, SD = 1.1) than the IC group (M = 0.36, SD = 0.60), P= 0.001. There was no significant difference between the number affective descriptors endorsed between the MP group (M = 0.72, SD = 0.88) and the other two groups. There was also a significant difference between the three groups when compared on the sum of sensory descriptors of pain, F (2, 199) = 4.67, P= 0.010. The MP group endorsed more sensory descriptors (M = 3.3, SD = 2.2), than the IC group (M = 2.3, SD = 1.5), P= 0.008. There was no significant difference between the number of sensory descriptors endorsed between the CDH group (M = 2.9, SD = 1.8) and the other two groups.
Psychological characteristics
When psychological symptoms were compared, there were statistically significant differences (P < 0.01) between the three groups on four of the nine dimensions of the SCL-90-R (somatization, obsessive-compulsive, depression, and anxiety). The groups also showed a statistically significant difference on the Global Severity Index, F (2, 197) = 8.25; P < 0.000, which is a composite measure of overall distress. The Global Severity Index combines information concerning the number and intensity of symptoms reported(see Table 1). Post-hoc comparisons showed significant differences between the MP and IC groups on all four of the dimensions (all P < 0.01), with the MP reporting more psychological distress in each case. The CDH group scored significantly higher on the somatization subscale than the IC group (P < 0.05). There was also a significant difference between the MP and IC groups on the GSI (P < 0.01). There were no other significant differences between the CDH group and the other groups on the SCL-90-R dimensions. Figure 1 depicts a graphical description of SCL-90-R mean T-scores for the three diagnostic groups.

SCL-90-R dimension means T-scores by group. ∗Indicates statistically significant difference between groups on these dimensions (P < 0.01). SCL-90-R, Symptom checklist 90 - revised. CDH, chronic daily headache; MP, myofascial pain; IC, intracranial pain. • CDH; ▪ MP; ▴ IC.
SCL-90-R symptom dimension means and standard deviations

Associated with analysis of covariance, with pain severity and pain duration as covariates.
When superscripts are the same between two groups on a measure, posthoc comparison indicate no significant difference in group means. When superscripts are different, posthoc comparison indicate significant difference between group means at P < 0.01. SCL-90-R, Symptom CheckList 90 – Revised; CDH,Chronic Daily headache; MP, Myofascial pain; IC, Intracapsular pain.
There were significant differences between the three groups on the life interference and life control subscales of the MPI (see Table 2). Post-hoc comparisons showed significant differences between all three groups on life interference (P < 0.01) with the CDH group reporting the most interference and the IC group reporting the least. There was also a significant difference between the IC and the other two groups on life control and affective distress, with the IC group reporting more control (P < 0.01) than both the CDH and MP groups. There were no other statistically significant differences noted between the groups on the subgroups of the MPI.
Multi-dimensional Pain Inventory means and standard deviations
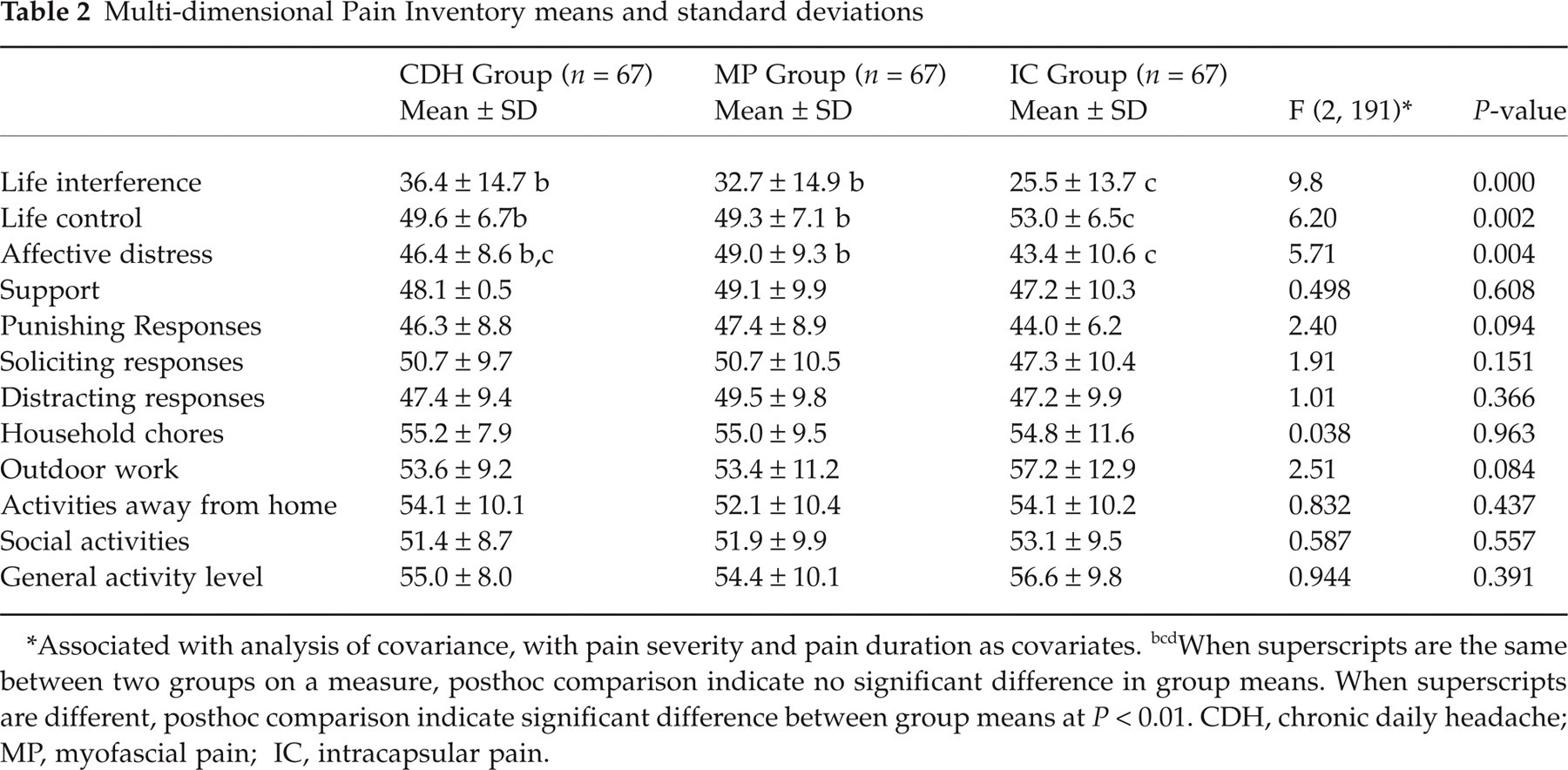
Associated with analysis of covariance, with pain severity and pain duration as covariates.
When superscripts are the same between two groups on a measure, posthoc comparison indicate no significant difference in group means. When superscripts are different, posthoc comparison indicate significant difference between group means at P < 0.01. CDH, chronic daily headache; MP, myofascial pain; IC, intracapsular pain.
The groups were also compared on the number of patients who met criteria for the different profile classifications on the MPI. χ2 analysis indicated a significant difference between the groups on the number of patients in each profile classification (χ2 = 21.6, P= 0.017). Specifically, there were more dysfunctional and interpersonally distressed profiles in both the CDH and MP groups than in the IC group.
Sleep quality
The PSQI gives a total score, representing overall sleep quality, as well as several subscale scores. The three groups showed statistically significant differences on the PSQI total score, sleep duration, sleep disturbances, use of sleep medication, and daytime dysfunction(see Table 3). Post-hoc comparisons indicated more overall sleep dysfunction in the MP group, than in the IC and CDH groups (P < 0.01). The MP and the CDH groups reported significantly more daytime dysfunction (P < 0.01) than the IC group. Compared to the CDH group, the MP group also reported significantly poorer sleep duration (P < 0.01. The CDH group reported significantly more daytime dysfunction than the IC group (P < 0.01). There were no other significant differences between the groups on the PSQI scores.
PSQI means and standard deviations

Associated with analysis of covariance, with pain severity and pain duration as covariates.
When superscripts are the same between two groups on a measure, posthoc comparison indicate no significant difference in group means. When superscripts are different, posthoc comparison indicate significant difference between group means at P < 0.01. PSQI, Pittsburgh Sleep Quality Index; CDH, Chronic Daily Headache; MP, Myofascial Pain;. IC, ntracapsular Pain.
Post traumatic stress symptoms
The total score obtained from the PCL was used to determine if there was a significant difference in PTSD symptoms between the three diagnostic groups. There was a significant difference between the number of patients reporting serious life stressors between the three groups (χ2 = 7.16 P= 0.028) with the CDH and MP group reporting more life stressors than the IC group. There was no significant difference, however, in the PCL total score, or on the PCL subscales (reexperiencing, avoidance, and arousal) between the three groups in the multivariate context (P > 0.01), indicating no difference in traumatic experiences or PTSD symptoms between the groups.
Physical measures
During the initial visit to the Center, diastolic blood pressure (DBP), systolic blood pressure (SBP) and heart rate (HR) were recorded. There were no significant difference found between the three diagnostic groups for SBP (CDH group: mean = 130.1, SD = 23.2; MP group: mean = 132.3, SD = 22.3; IC group: mean = 128.9, SD = 18.1), DBP (CDH group: mean = 73.3, SD = 14.7; MP group: mean = 74.9, SD = 13.0; IC group: mean = 70.7, SD = 14.1), or HR (CDH group: mean = 78.6, SD = 13.9; MP group: mean = 75.5, SD = 11.7; IC group: mean = 76.7, SD = 11.0).
Discussion
The aim of the present study was to investigate psychological and sleep quality differences among three distinct facial pain groups, that is chronic daily headache, myofascial pain and TMJ intracapsular pain patients. Given this focus, no nonpatient control group was included in the data analyses. Nevertheless, the psychological and sleep quality measures used during the present study have established norms with cut-off scores of clinical significance which are normally two standard deviations over the general population average score (e.g. in the case of the SCL90-R subscales a score of greater than 70T). Consequently, these cut-off points may be used by the reader to evaluate the difference in psychological distress between the selected facial pain groups and the general population.
Chronic daily headache is the predominant diagnosis among patients visiting headache centres, and represents a major challenge for headache specialists (14). Few studies, however, have analysed the possible psychological differences among different CDH subpopulations (15) (i.e chronic migraine vs. chronic tension-type headache). Our study results differ from those of Wang et al. (15), who found higher levels of psychological distress in chronic migraine patients than in chronic tension-type headache patients. The number of patients in our CDH subgroups, however, was too small to draw definitive conclusions regarding these matters. Further research is needed to clarify whether CDH subpopulations present distinct psychological and sleep quality profiles from one another.
Headaches are also frequent complaints of patients with TMD (4). Even so, studies analysing psychological differences between CDH and TMD patients are sparse in the literature (6). The present study revealed higher levels of psychological distress among CDH and MP groups than among the IC group on most psychological domains. Although the MP group revealed numerically higher levels of psychological distress on most psychological domains than the CDH group, these differences were not statistically significant.
Our findings are generally consistent with the results of Mongini et al. (6) who also found lower levels of psychological distress in TMJ pain patients than in facial pain and CDH patients. Since the Mongini et al. (6) study did not control for pain duration and intensity in the different diagnostic groups, our findings strengthen their results. In the present sample, we also found statistically significant differences in life stressors with the CDH and MP groups reporting more life stressors than the IC group. There were no statistically significant differences, however, between TMD and CDH patients on the PCL total score or on the PCL subscales, including reexperiencing, avoidance, and arousal. Additionally, none of the patient groups overall scored over 39 on the PCL total score which is generally considered the cut-off point for PCL-C clinical significance (12). These findings suggest that only a small number of patients may be affected by post-traumatic stress in the present sample. This finding is rather surprising given the evidence from other chronic pain samples that indicate a high prevalence of significant life stressors in these populations (16).
Several lines of evidence indicate that PTSD symptoms are most prevalent among chronic pain patients with dysfunctional profiles compared to those with adaptive coper or interpersonally distressed profiles (17). Our study results support this hypothesis since both PCL-C scores and dysfunctional profiles were numerically higher in the MP and CDH groups, than in the IC group. Additionally, only a small percentage of the overall sample presented with dysfunctional profiles, and this may explain the low prevalence of PTSD symptoms.
Research has indicated that the severity of anxiety disorders and life interference may be positively correlated with the severity of PTSD symptoms in chronic pain patients (18). Furthermore, other studies suggest that patients with persistent headache pain and those with musculoskeletal pain who present with dysfunctional profiles tend to have elevated anxiety sensitivity relative to other pain populations (17). In the present study, those patient groups with higher PCL-C scores, that is CDH and MP groups, also revealed the highest levels of anxiety, life interference, and affective distress, the lowest life control scores, and the highest number of dysfunctional profiles. Therefore, anxiety disorders and PTSD symptoms seem to be highly prevalent in patients with dysfunctional patterns of pain behaviours.
Our study also revealed significant differences between the MP and IC group on four of the nine dimensions of the SCL-90-R (somatization, obsessive compulsive, depression, and anxiety). These groups were also statistically different on the Global Severity Index, which is a composite measure of overall distress. Our results are in agreement with other studies in the field of TMD that indicate higher levels of psychological distress in MP patients than in TMJ pain patients (19). Michelotti et al. (20), on the other hand, did not observe psychological differences between MP and IC patients, although this may be due to methodological differences such as sample selection criteria, and pain duration and intensity discrepancies between the different study populations.
There is evidence that high levels of pain duration and intensity may partially account for the higher levels of depression and anxiety observed in chronic pain patients (21, 22). Therefore, the psychosocial differences observed between MP and IC patients in previous studies could be attributed directly to a difference in pain intensity and duration among the different pain populations. In light of the current findings and those of Lindroth et al. (19), both of which controlled for pain intensity and duration, there seems to be compelling evidence for higher levels of psychological distress among MP patients as compared to IC patients regardless of pain intensity and pain duration.
It is noteworthy that only the MP group scored 63 or more on two of the SCL-90-R dimensions (somatization and obsessive compulsive behaviour). Scores greater than 63-T are considered by most authors as the ‘cut-off’ point for clinical significance (21). Also neither the CDH nor the IC group scored over 63 on any of the SCL-90-R dimensions. All groups, however, scored higher than the average general population means in all SCL-90-R dimensions. Given these findings, it is important to screen for major psychological distress when evaluating these chronic pain populations because there is the possibility that such issues may be significant for developing a comprehensive treatment plan.
Sleep disturbances are extremely prevalent among pain populations (23). Few studies, however, have provided information about sleep quality differences between TMD and CDH populations. Our study results showed more overall sleep dysfunction in MP group than in the CDH and IC groups. Our sleep findings are generally consistent with Mongini et al. (6) who also observed a higher prevalence of sleep disorders, as identified by the MPI questionnaire, among facial pain patients when compared to primary headache and IC patients. Their results did not reveal sleep quality differences between primary headache and TMJ pain patients. To the best of our knowledge, our study is the first to evaluate sleep quality differences between TMD and CDH populations by using a specialized sleep quality questionnaire (PSQI). A detailed analysis of our data shows that the MP group also had more daytime dysfunction than the IC group. Additionally, the CDH group had significantly poorer sleep duration than the MP group. Furthermore, since our study design controlled for pain intensity and duration, the sleep quality differences observed between our study groups could not be attributed to a difference in pain intensity or duration among the different pain populations. These findings regarding sleep differences may be therefore the result of true pathophysiological differences between IC, MP, and CDH patients. The more diffuse nature of pain and its higher capacity to generate central excitatory effects in CDH and MP patients, may account for some of the sleep quality differences observed between these pain populations and patients diagnosed with IC pain.
It is possible that sleep disturbances may be a consequence of pain per se and are not necessarily related to a specific pain disorder (24). Some investigators have reported that while pain intensity and duration may be important in the development of sleep disturbances, other variables such as concomitant fatigue, medication overuse, mood disturbance or depression, may also play an important role in sleep disturbance pathogenesis (25; 26). Our study results support this latter hypothesis since sleep disturbance and psychological distress scores were significantly higher in the MP and CDH group, than in the IC group.
Sleep disturbance may key factor in MP and CDH pathophysiology. It is well established that the balance between hypothalamic growth hormone-releasing hormone (GHRH) and corticotropin-releasing hormone (CRH) plays a key role in normal and pathological sleep regulation (27). GHRH stimulates deep sleep (stages 3 and 4) and growth hormone (GH) secretion but inhibits cortisol release, whereas CRH disrupts deep sleep and decreases GH secretion. During normal ageing and during depression, the GHRH:CRH ratio is distorted in favour of CRH, resulting in disturbances in sleep endocrine activity (27). Since GH is known to play a crucial role in skeletal muscle synthesis and repair, deep sleep deprivation, which alters GH synthesis, may compromise muscle healing in MP patients. Further research is warranted to examine the effects of GH deficiencies in the pathogenesis of MP disorders.
Hypothalamic dysfunction has also been implicated in transformed migraine pathogenesis. Several authors have reported abnormal patterns of hypothalamic hormonal secretion in transformed migraine patients when compared to normal individuals, including increased cortisol concentrations, and lower melatonin concentrations (28). Furthermore, recent evidence suggests that a dysfunction of the central serotonergic system, which has been implicated in pain control and sleep regulation, may be strongly related to hormonal hypothalamic-pituitary-adrenal axis (HPA) alterations in chronic tension-type headache patients (29). Research findings have also revealed that depression and anxiety disorders may be associated with HPA axis and autonomic nervous system (ANS) up-regulation, and inhibition of vegetative processes likely to impede survival during a life threatening situation (i.e sleep and endocrine programs for growth) (30). Therefore, psychological distress and sleep disturbances in MP and CDH patients may be both the cause and/or result of ANS and HPA axis dysfunction.
This study confirms and extends previous reports addressing psychological differences between TMD and CDH populations. Although CDH patients generally reported lower levels of psychological distress than MP patients, these differences between these groups were not statistically significant. Chronic daily headache patients also showed numerically higher levels of psychological distress and sleep disturbance than IC patients. However, most of these differences, although sometimes statistically significant, remained within one standard deviation of one another, and this raises questions about their ultimate clinical significance, for this sample at least. Therefore, further research is needed to determine whether CDH, MP, and IC populations require distinct psychological management as a part of a multidimensional treatment approach.