
Abstract
The relationship of chronic daily headache (CDH) and childhood adversity is still controversial. We therefore conducted a survey for CDH (≥15 days/month, average ≥ 2 h/day) among all students in three public schools in Taiwan. The Global Family Environment Scale (GFES), which yields a score according to childhood adverse events in the family, was used to compare childhood adversity between cases of CDH and their age- and sex-matched controls. In total, 4645 students were surveyed and 58 with CDH were identified. Significantly lower GFES scores, indicative of worse childhood adversities, were evident in the CDH group (76.7 ± 19.2), compared with the control group (86.0 ± 8.9, P = 0.001). Physical abuse (10% vs. 0, P = 0.012) and parental divorce (17% vs. 3%, odds ratio = 5.8, P = 0.015) were more frequent in the CDH group. The results indicate that childhood adversitys may contribute to greater risk of the development of CDH in young adolescents.
Introduction
Increased morbidity to depression and other psychiatric disorder is a long-term consequence of childhood adversity such as abuse and neglect (1, 2). However, whether chronic pain, such as chronic headache, also increases after childhood adversity is still controversial, with the available research displaying variant results (3–5). The discrepancy of the results may arise from methodological problems, such as selection bias of samples and recall bias of subjects. The long period of time between childhood traumas and the occurrence of pain may also hinder such investigation (6). Hence, more research is needed to elucidate the relationship between headache and childhood adverse events (AEs).
Chronic daily headache (CDH) is a severe and disabling condition. It occurs in about 3–5% of the general population (7, 8) and greatly impairs the victim's quality of life and working performance (9). Characteristics of CDH in adolescents are less well studied. Whether adolescent CDH is linked with childhood adversity is little understood.
Studies in adolescents can be helpful in elucidating the relationship between childhood adversity and pain in later life, because information on childhood events is more available in adolescents. The time lag between adolescence and childhood is relatively short compared with adults. Furthermore, teachers and other family members may provide more childhood history of the subjects.
Third-party information is particularly valuable, since sufferers’ recall may be biased, because of their greater than normal efforts at recall and a tendency to remember the past in a more negative way (10). A comprehensive and systematic approach to childhood family information, via the recruitment of teachers and carers, as well as subjects, in the evaluation can help reduce recall bias of the subjects’ own memory.
This approach was adopted in the present study, which was designed to assess childhood family events in adolescents with CDH in a community population to examine whether childhood adversities are associated with CDH in later life.
Subjects and methods
Subjects
Subjects were all students in three public junior high schools in Taiwan. Two schools were in metropolitan Taipei and one was in rural south-eastern Taiwan. All the students were between 13 and 15 years old, equal to Grades 7–9 in the American educational system. Since there is no delay in our junior high schools, all students in the same class were of the same age.
Junior high school education is mandatory in Taiwan, and over 90% of the residents of this age group in these school districts attend public schools, from diverse economic backgrounds. The remaining adolescents attend private schools. Thus, the recruitment of students from the public system represented the overwhelming majority of this student population.
After cases with CDH were identified (see below), control subjects were selected first by adding and then by reducing the number of the cases by 5 or 10. The rationale for the control determination reflected the structure of the Taiwanese school system. In this system, each public school student is assigned a number in the class. If the student with the number equal to the case's number increased by 5 was of the same sex, then he or she was selected as the control. If that student was not of the same sex, than the student with the number equal to the case's number decreased by 5 was selected if he or she was of the same sex. If neither combination worked, then the class number increased or decreased by 10 was tried.
Students in the control group were not excluded if they experienced some non-chronic episodic headaches.
Diagnosis of CDH
The two-stage headache survey used in the present study was published previously in a study of headache in adolescents (11). First, all students filled out a headache-screening questionnaire. All subjects who reported having headaches on ≥ 7 days per month or were absent from school due to headache over 3 days during the last semester were examined by trained senior neurologists through a standardized systematic diagnostic procedure for the diagnosis of CDH and its subtypes.
CDH was defined as a headache frequency of at least 15 days with headache per month for at least 3 months. The average headache duration should be at least 2 h per day. More details of the screening and diagnostic processes and the prevalence of CDH in adolescents will be presented in another communication. CDH were further classified into three types, i.e. chronic migraine, chronic tension-type headache, and unclassified headache according to criteria proposed by Silberstein et al. (12).
Assessment of childhood adverse events
The Global Family Environment Scale (GFES) was used to evaluate childhood family environment in cases of CDH and their controls. The GFES is a global rating scale that quantifies inadequate family environment and adverse family events during childhood. GFES ratings are based on positive and objective evidence of family events occurs before the age of 12 years (13). It is not a rating of subjective satisfaction with family relationship or ambience.
Raters should comprehensively collect and evaluate all evidences of AEs during childhood. The GEFS rating gives concrete examples of events to score in a range. For example, a generally adequate family environment will score between 81 and 90. The frequent absence of a parent due to job or illness will be a slightly unsatisfactory family environment, scoring between 71 and 80. Moderate parental discord resulting in separation and divorce will be a moderately unsatisfactory family environment, scoring between 51 and 70. Hostile separation with problems of custody or some abuse by parental figures or siblings will result in a poor family environment, scoring between 31 and 50. Evidence of substantial abuse or neglect will result in a very poor family environment, scoring between 11 and 30. A family consisting of a single parent is not in itself regarded as an adversity.
Given the long-term enduring character of CDH, it is very difficult for sufferers and their family members not to mention the suffering. To keep the evaluation of childhood family environment as blind to the condition of headache as possible, we adopted a two-stage assessment.
First, the students’ own teachers gathered information of their childhood family through interviews with students and their family members. Research has established that those who administer the GFES can be trained by a manual, and that the rating test is reliable across different cultures (14). We developed a checklist to ensure all data needed in the GFES were routinely collected during these teacher interviews. Teachers assessed the students’ childhood family environment and reported a vignette describing it and the answers to the checklist in a case report form. Therefore, information such as students’ major caretakers, household, parents’ marital status, affection, expectation, discipline, punishment, neglect and abuse was routinely gathered.
Second, three senior clinicians, who were trained in the reliability of the GFES and were blind to the subjects’ headache condition, read the case report form together and gave a score on the basis of consensus. They also coded the occurrence of abuse, neglect, parental divorce, and conflicts in custody according to the information described in the case report form.
Statistical analysis
The score of GFES was analysed by Student's t-test and one-way ANOVA. The occurrence of child abuse, neglect, and parental divorce was analysed by χ2 test. A P-value of 0.05 was regarded as significant. Two-tailed tests were used throughout the study.
Results
A total of 4645 students were surveyed in the three public schools. The respondent rate was 97.6%. Fifty-eight (1.2%) students had CDH. This group comprised 39 girls (67.2%) and 19 boys (32.8%). Of the 58 students, 22 (37.9%) were in 7th grade, 13 (22.4%) were in 8th grade, and 23 (39.7%) were in 9th grade. Forty-one (70.7%) of the 58 students had chronic migraine, 10 (17.2%) had chronic tension-type headache and seven (12.1%) had unclassified CDH.
Table 1 shows the GFES scores of the different groups. In the CDH group, the mean score of the GFES was 76.7 ± 19.2. The scores were not different between boys (79.8 ± 19.2) and girls (75.2 ± 19.3, P = 0.479). However, the mean GFES scores were significantly different among grades (P = 0.043, one-way ANOVA). Students in 7th grade had a lower mean GFES than students in 9th grade (68.7 ± 22.6 vs. 81.9 ± 16.5; P = 0.02, one-way ANOVA and post hoc LSD test). Among the different subtypes of CDH, the average GFES scores were 73.9 ± 21.0 in the chronic migraine group, 80.0 ± 14.7 and in the chronic tension-type group, and 88.3 ± 2.4 in the unclassified group. These differences were not significant (one-way ANOVA test).
Comparison of mean Global Family Environment Scale (GFES) scores between chronic daily headache (CDH) subjects and controls

∗Mean ± SD.
Table 1 also displays the data for the control population. Among the 58 randomly selected students that were controlled for sex and age, eight (14%) had headache frequencies between 1 and 14 days per month and the remaining had headache frequencies of < 1 day per month. The mean GEFS score was 86.0 ± 8.9. The mean GFES scores of different sex and grades in the control group are also shown in Table 1. There were no differences either between boys and girls or among students of each grade.
As shown in Table 1, the CDH group had a significantly lower GFES score than the control group (P = 0.001, t-test). In both boys and girls, the GFES scores were still significantly lower in the CDH group compared with controls. When subjects were divided into grade 7, 8, or 9, the CDH group still had significantly lower GFES scores in each grade than the controls.
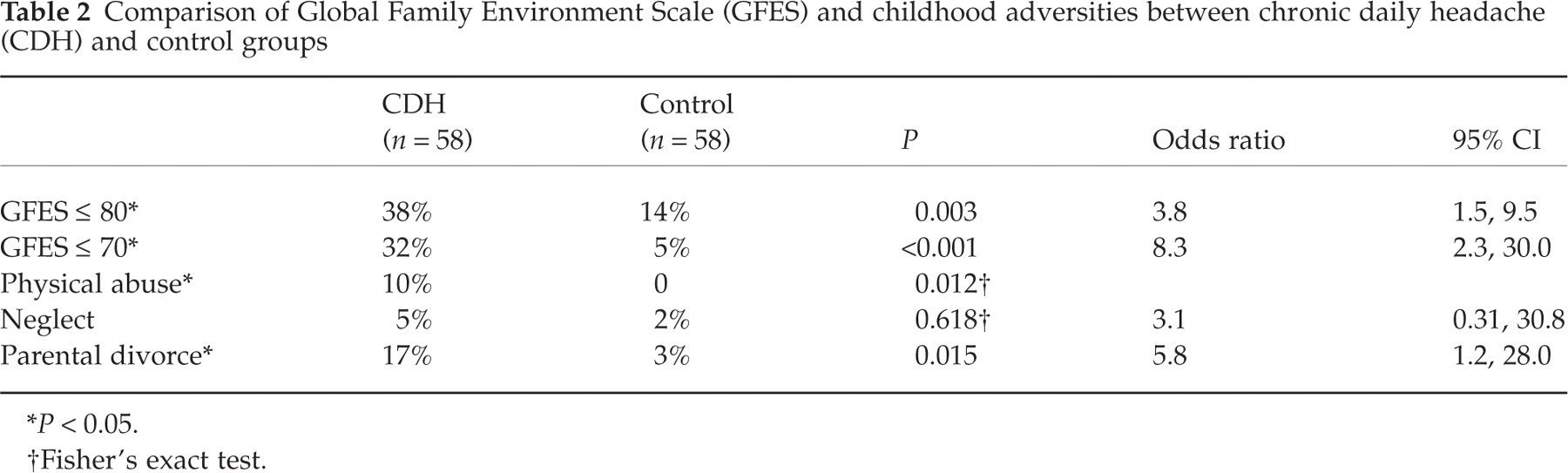
Table 2 shows that the percentages of subjects who had a GFES of ≤ 80 (i.e. equal to or worse than a slightly unsatisfactory family environment) and who had a GFES of ≤ 70 (i.e. equal to or worse than a moderately unsatisfactory family environment) were significantly higher in the CDH group than in the control group. Table 2 also shows that physical abuse had occurred in the childhood of six subjects, all of whom were in the CDH group. The difference was significant (P = 0.027, Fisher's exact test). No case of childhood sexual abuse was found either in the CDH group or in the control group. Three students in the CDH group and one student in the control group were victims of child neglect. The difference was insignificant (P = 0.6, Fisher's exact test). Ten subjects with CDH experienced parental divorce during childhood, which was significantly more frequent than the two students in the control group (P = 0.015, χ2 test). The frequencies of parental divorce were similar between chronic migraine subtype (eight of 41, 19.5%) and chronic tension-type headache (two of 10, 20%). Seven (58%) of the 12 divorces involved a parental conflict in child custody. However, the frequencies of custody conflict were not significantly different between the CDH group (six of 41, 14.6%) and control group (one of 10, 10.0%; P = 0.114, Fisher's exact test).
Comparison of Global Family Environment Scale (GFES) and childhood adversities between chronic daily headache (CDH) and control groups
∗P < 0.05.
†Fisher's exact test.
Discussion
In the present study we have shown that CDH in young adolescents is associated with family adversity, physical abuse, and parental divorce occurring during childhood. These results were obtained in a convenient sample that was representative of the community population.
Victims of child abuse tend to utilize healthcare services more frequently during their later life (15). Thus, selection bias has hampered the study of child abuse history in clinical samples. In the present study, our CDH subjects were identified through our community survey. Therefore, the results may not be affected by differences in subjects’ help-seeking behaviour.
Recall bias of a retrospective case–control study generally originates from differences in the effort and in the way the subjects recollect their past. Those who experienced suffering may try harder than the controls to recall past events. Pain may also result in a biased negative memory of the past (10). In our study, the GFES required evidence of objective events gathered from as many resources as possible. Compared with self-reports that rely on subjects’ own recollection, our results may be less affected by recall bias of the subjects suffering from pain.
A prospective study can avoid recall bias. In a recent prospective study of abuse and pain, Raphel et al. found no association between pain and abuse in victims of court-convicted abuse or neglect (5). However, the study was limited by using court conviction as the only definition of child abuse. If there was no court-convicted abuse during the follow-up period, the subject was considered to be free from abuse. Court-convicted abuse comprises only a small proportion of cases of abuse and neglect, and these victims may receive more social support and care than do the majority of abuse victims. Therefore, court-convicted cases may not be representative of child abuse and neglect in the community (16).
Of particular note in the present study was the> 5 odds ratio in the association between childhood parental divorce and CDH. Divorce is more easily reported and less prone to distortion of false or repressed memory than are child abuse and neglect. Divorce has been implicated with recurrent headache in adolescents (17), and tension-type headache (but not migraine) in children and adolescents (18). In the present study the rates of parental divorce between our chronic migraine subjects and chronic tension-type headache sufferers were not different. Parental divorce in adolescent CDH and its subtypes warrant more attention from clinicians and researchers. The frequency of parental divorce in our control group is similar to that of the general population in Taiwan (4% in National Population Survey (19)).
The six cases of physical abuse in the study were all in the CDH group, suggesting a strong link between childhood physical abuse and headache. Theories have tried to explain the correlation of physical abuse and pain, including Engle's psychodynamic explanation (20) and a hypothesis that pain perception may be altered in abused individuals (21). In contrast, Toomey et al. suggest that it is coping with pain that differs between abused and non-abused patients, not the perception of pain. They found that punishing response and loss of control of pain were higher in abused patients with chronic pain, indicative of worse coping in the abused patients. However, the description of pain was not different between abused and non-abused patients, suggesting similar perceptions of pain (22, 23). In parallel with the finding was the report that maladaptive coping with pain and generalized poor coping in life were associated with childhood adversity, chronicity of pain, and psychiatric morbidity (24).
Depression may also link childhood adversity with CDH. Depression may trigger the transformation of episodic headaches into CDH (25). Since child abuse is associated with depression in later life (1, 2), they may be further involved in the development of CDH in subjects with episodic headache.
The present study documented a higher GFES in those CDH subjects in grade 7 than in grade 9. This observation suggests a stronger relationship between childhood adversity and CDH in younger children than in slightly older children. Conceivably, younger children may be more susceptible to childhood adversity, perhaps due to being less removed temporally from the occurrence of the adversity, or to a less mature personality in the younger adolescents. The role of the age at which the CDH occurs in relation to the childhood trauma deserves more investigation. Of similar interest is the age at which the trauma occurs. One study has shown that childhood sexual assault outweighs adulthood assault in the association with CDH (4). However, only childhood abuse was investigated in the present study.
The fact that no sexual abuse was found in this study may reflect the difficulty of identifying victims of sexual abuse. It is also possible that abuse and neglect are rare in our communities; however, no epidemiological data of abuse or neglect are available in Taiwan. No association between neglect and CDH can be drawn from our study, perhaps due to the small number of neglected students in the study.
The present study tried to assess CDH and childhood adversity in a community population free from the selection bias of clinical samples. Because of the high questionnaire response rate and the homogeneity of the junior high school system in Taiwan, we are confident that the small student population provides a representative sample of 13–15-year-old Taiwanese adolescents.
The GFES has been applied successfully to the study of psychiatric samples. Here we have shown that the GFES is also a useful tool in samples of physical illness. Through the application of the GFES, we found that childhood adversity, including physical abuse and parental divorce, were risk factors of CDH in adolescents. Thus, in conclusion, we suggest that a traumatic childhood family environment may predispose to CDH in early adolescence and that psychosocial development may play a role in the formation of adolescent CDH.
Footnotes
Acknowledgements
Presented in part at The 10th Congress of the Asian College of Psychosomatic Medicine, Taipei, Taiwan, 29 September 2002.