
Abstract
The first description of what subsequently came to be known as the red ear syndrome (RES) was by Lance in 1994 (1) (Table 1, cases 2-4). Subsequently he reported a total of 12 patients with what he called the red ear syndrome (2) (Table 1). The syndrome was characterized by attacks of unilateral ear discomfort or burning during which the ear became red. The discomfort often extended beyond the ear. He reported an association with upper cervical disorders, glossopharyngeal and trigeminal neuralgia, temporomandibular joint (TMJ) dysfunction, and a thalamic syndrome. In two of the 12 cases (Table 1, cases 11 and 12) no cause was apparent. In some cases the episodes were spontaneous and in others they were precipitated by touch, exertion, heat or cold, neck movements, stress, cleaning the ear, washing hair or brushing it the wrong way, and eating or drinking. While some of their patients had a history of headaches (including migraines), a consistent relationship to migraine headaches was not identified.
Introduction
The first description of what subsequently came to be known as the red ear syndrome (RES) was by Lance in 1994 (1) (Table 1, cases 2–4). Subsequently he reported a total of 12 patients with what he called the red ear syndrome (2) (Table 1). The syndrome was characterized by attacks of unilateral ear discomfort or burning during which the ear became red. The discomfort often extended beyond the ear. He reported an association with upper cervical disorders, glossopharyngeal and trigeminal neuralgia, temporomandibular joint (TMJ) dysfunction, and a thalamic syndrome. In two of the 12 cases (Table 1, cases 11 and 12) no cause was apparent. In some cases the episodes were spontaneous and in others they were precipitated by touch, exertion, heat or cold, neck movements, stress, cleaning the ear, washing hair or brushing it the wrong way, and eating or drinking. While some of their patients had a history of headaches (including migraines), a consistent relationship to migraine headaches was not identified.
Clinical characteristics in the red ear syndrome cases reported by Lance (2)

TMJ; temporomandibular joint, +:, favourable response of pain or paresthesia, –:, lack of response of pain or paresthesia; NA, information not available.
A striking association with migraine headaches was reported by Raieli et al. in 2002 (3). They reported eight patients (seven children and one adult) with migraine headaches, all of whom had what was felt to be idiopathic red ear syndrome (Table 2). The RES episodes often occurred in association with the migraine, but at times were seen to occur in isolation. Raieli et al. suggest that the RES be included in the ‘not classifiable’ category of the secondary headache disorders group of the International Headache Society (IHS) classification of headache disorders.
Clinical characteristics of the red ear syndrome cases reported by Raieli et al. (3)
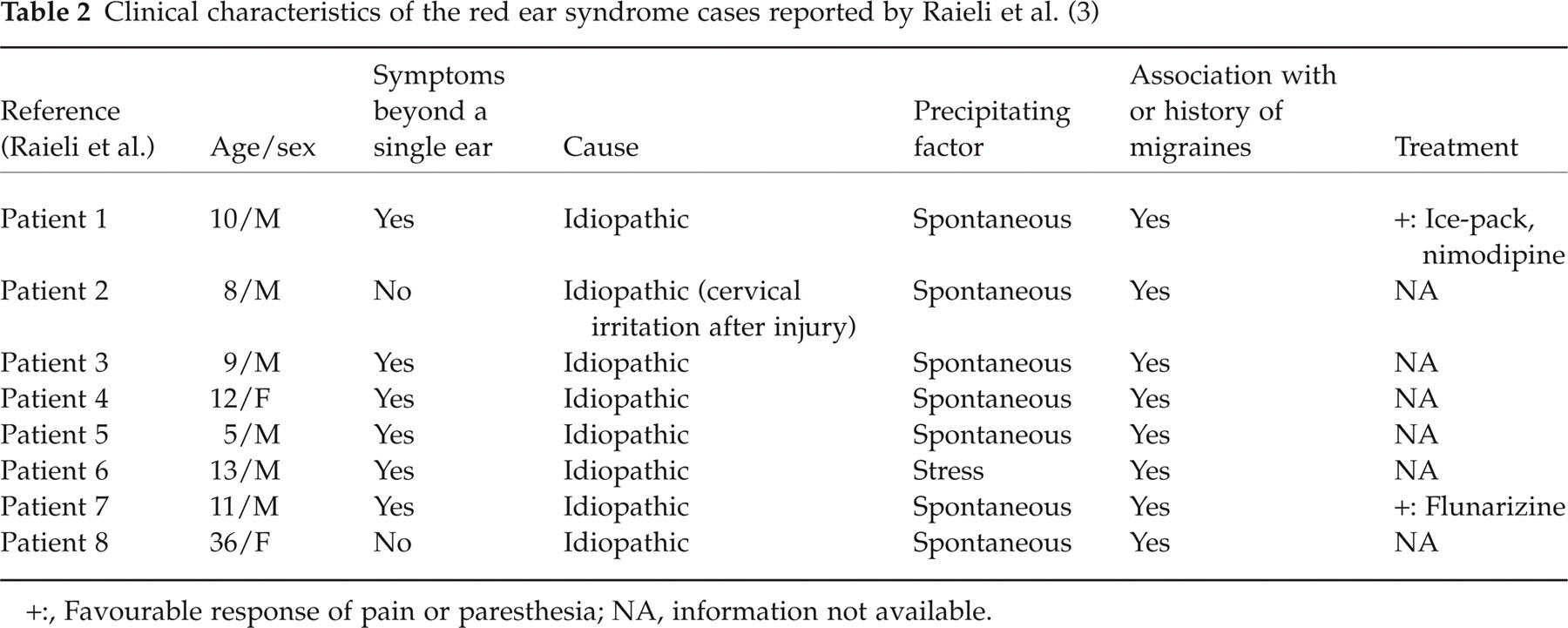
+:, Favourable response of pain or paresthesia; NA, information not available.
We report two patients with the RES. The literature on the entity is reviewed and a unifying pathophysiological hypothesis is suggested.
Case reports
Patient 1
A 66-year-old man was seen by us because of a 4-week history of attacks of burning and warm feeling involving the left ear. He recalled having twisted his neck while doing sit-ups a day before the onset of this symptom. The attacks happened once every 2–3 h and each attack lasted for 20–30 s. His wife had noted that the ear became obviously red during the attack. A cervical spine magnetic resonance imaging (MRI) revealed moderately severe degenerative changes at C4 and C5 interspace with narrowing of the left C4 neural foramen. He had a history of Barrett's oesophagus and was taking omeprazole. He did not have a personal or family history of headaches. The neurological examination was normal. An attack was witnessed during the examination. The left ear became red and warm and the patient was aware of a burning sensation and warmth. He was able to induce the attack consistently by gently rubbing the ear one or two times.
Patient 2
A 66-year-old man was referred to us for evaluation of a segmental pruritus. For 4 years he had been symptomatic with a tingling sensation over the right supraclavicular region which was brought on when he would turn his head to the right. An associated complaint was spontaneous and neck movement induced itching involving the right ear, lower face and neck. There was a burning sensation and warmth in the area involved by the pruritus. A cervical spine MRI was remarkable for a prominent dorsal end plate spur at the C4 interspace on the right side that was narrowing the right C4 neural foramen. He was advised to discontinue tramadol and oxycodone. He was also placed on neck traction for the neck pain. His pruritus improved, but even at 2 months’ follow-up the spontaneous right ear and lower face pruritus and burning was still present. His past history was remarkable for atrial fibrillation, coronary artery disease, asthma, and sleep apnoea. He had a lumbar laminectomy done 3 years ago for a right L5 and S1 radiculopathy. There was no personal or family history of headaches. His medications included amiodarone, hydrochlorthiazide, diltiazem, rabeprazole, montelukast sodium, and albuterol and ipratropium inhalers. His neurological examination was unremarkable. Note was made of the fact that if the patient turned his head to the right and keep it in that position for a minute, he would become symptomatic with right ear, face, and neck pruritus.
Discussion
In addition to the cases reported by Lance (2) and Raieli (3), there are other isolated reports of patients with similar phenomena (4, 5), one being in a child with severe neuropsychiatric manifestations due to systemic lupus erythematosus who presented with an unexplained red ear phenomenon (6). Features of the red ear syndrome were reported to be present in two patients with chronic paroxysmal hemicrania (CPH) and one patient with extratrigeminal episodic paroxysmal hemicrania (EPH) (7, 8). These authors suggest that this symptom complex be included with the trigemino-autonomic cephalalgias [short-lasting, unilateral, neuralgiform headache attacks with conjunctival injection and tearing (SUNCT), hemicrania continua, CPH, EPH, and cluster headache] described by Goadsby and Lipton (9).
Note that neither of our two patients had a history of migraine headaches. A review of the reported cases seems to suggest that those patients in whom the RES is associated with migraine headaches have spontaneous attacks and are younger; whereas those patients in whom the RES may be related to an upper cervical pathology have an identified precipitating factor and are in an older age group. The initial report was entitled ‘The mystery of one red ear’ (1). That the disorder may not be strictly unilateral was first suggested by Hirsch (10). Five of 29 headache patients studied by him had frequent red discoloration of the ears independent of headache (11). Subsequent reports have confirmed this. This highlights a similarity to migrainous phenomena.
An understanding of a possible pathophysiological hypothesis that can explain the RES requires an understanding of the neural and vascular supply of the ear. The ear lobe is innervated by C2 and C3 nerve roots via the greater auricular nerve. The anterosuperior aspect of the ear is supplied by the auriculotemporal branch of the mandibular division of the trigeminal nerve. The zygomaticofacial branch of the infraorbital division of maxillary division of trigeminal nerve supplies the cheek. The ear receives its blood supply from the external carotid artery via an anastomosis between the anterior auricular branches of the middle temporal artery and the posterior auricular artery. The trigeminal nerve also provides sensory innervation of the external carotid artery. Sympathetic innervation of the facial skin includes vasoconstrictor and vasodilator fibres (12). In humans release of sympathetic vasoconstriction plays the dominant role in increase in ear temperature. Parasympathetic vasodilatation is most marked in the nose and cheek and least apparent in the ear (13). Red ears are a result of activation of sympathetic vasodilatation or inhibition of sympathetic vasoconstriction.
It has been shown that electrical stimulation of the third cervical root causes vasodilatation of the ear and the part of the cheek adjacent to the ear (14). Lance proposed that irritation of the C3 root by an upper cervical lesion could result in an antidromic discharge of impulses along the third cervical root and release of vasodilator peptides from afferent nerve terminals (2). These include substance P, calcitonin gene-related peptide (CGRP), and nitric oxide, and are responsible for pain and vasodilatation. Studies in rats have shown that central projections from neurones innervating the lower lip extend as far caudally as C4 (15). Since afferents from the upper cervical roots converge on the spinal nucleus of the trigeminal nerve, symptoms could be seen in the region of the sensory distribution of the trigeminal nerve. A local axon reflex could explain cases associated with temporomandibular joint dysfunction, and cases in which heat and touch provoke the symptom (2). The induction of RES by rubbing the ear in our first patient suggests an axon reflex with release of vasodilator peptides. RES in association with glossopharyngeal neuralgia could be caused by involvement of pain afferents from the glossopharyngeal nerve that join the spinal tract (2). This hypothesis would not explain the well-documented idiopathic cases that have been associated with migraine headaches. Goadsby and Lipton suggest that both paroxysmal hemicrania and RES might be due to a pathogenic mechanism based on a brain stem connection between the trigeminal nerve and the facial parasympathetic outflow (9). The anatomic substrate for a unifying hypothesis to explain our current knowledge of RES would be the overlap between the neurones of the pars caudalis component of the trigeminal nucleus and the upper cervical cord. Presence of symptoms beyond the distribution of the trigeminal nerve reflects this overlap. This has also been felt to be the reason why some migraineurs have neck pain that can occur independent of a typical migraine headache and still respond to migraine-specific therapies (16). Trigeminovascular activation, as is believed to occur in migraine headaches (17), could explain occurrence of RES in patients who do not have a upper cervical pathology.
A review of literature suggests that the involvement may be unilateral or bilateral, symptoms are often present beyond the ear, colour change is only one of many symptoms that patients report, and the varied aetiology and associations raise some scepticism about use of the term in a syndromic context. The term RES should be retained until the mechanism is clarified. The proximate cause of some components of the syndrome may be dysregulation of sympathetic outflow. The same may be due to an upper cervical pathology or due to involvement of the trigeminovascular system, as is seen in migraineurs. Due to the varied aetiology we do not believe that it can be regarded as a form of trigemino-autonomic cephalgia or have a place in the IHS classification of secondary headaches. It is best viewed as an entity that may have primary and secondary forms, with the primary form probably being a migrainous phenomenon. The secondary form seems to be a neuralgiform radiculopathy involving the C3 root with release of vasodilator peptides or nitric oxide.