
Abstract
Migraine induces disability and an impaired quality of life, even between attacks. As most studies are based on subjective reports only, this study was set up to objectively quantify the interictal daily activities and heart rate of migraine patients, in relation to their subjectively reported highest realizable level of activity and of symptoms of mood in their habitual environment. Measurements were obtained during a migraine-free 2-day period of 24 patients (age range: 21-57 years) and 24 controls (age range: 18-59 years). Accelerometry was used to quantify the time spent in different postures and movements. The subjective parameters were documented by daily log. Whereas heart rate was similar for patients and controls, migraineurs were found to be significantly less physically active than controls and reported a significantly lower realizable level of activity. In addition, when active, their body motility was less than that of controls. Migraine patients also showed a higher level of sleepiness and lower level of vigour. These interictal behavioural and subjective phenemona objectively illustrate the individual and societal burden of migraine and its chronic impact on both domains.
Introduction
During the last 10 years it became increasingly clear that pain indices (the pattern of symptoms, the frequency and severity of attacks) alone provide incomplete information about the impact of migraine on the patient. To adequately describe and evaluate this impact, information about the psychological, social, and behavioural effects on the level of functioning during the attack is also needed. Hence, disability scales and Health-related Quality of Life (HRQoL) instruments that promised to provide this additional information came into use, enabling clinicians to distinguish between the less and more disabled patient, to tailor treatment and measure its effect. The resulting information was also useful to policy makers allocating health care resources (1–3). Findings of many studies utilizing these questionnaires indicate that, compared with the general population and other populations with chronic illnesses, during an attack migraineurs are disabled and exhibit an impaired quality of life. They report emotional disturbances, difficulty or limitation in performing daily activities, interference with social and sexual activities (4–7). Migraine not only causes suffering for individuals. It also has an impact on society. This collective impact of migraine is measured by assessing the direct and indirect costs for society. Direct costs encompass the costs of diagnosing and treating; indirect costs include the economic effects on productivity at work, at home and in other roles. Studies on both direct and indirect costs reveal that the collective burden of migraine is substantial (for the USA about £13 billion a year; for the Netherlands about 300 Euro a year) and illustrate the need for improved strategies to target migraine treatment (3, 6, 8–13).
Recently, it was recognized that the individual burden of migraine extends beyond the episodes of attacks. The results of several studies showed that migraine also induces an impaired HRQoL between attacks (5, 9, 14–16). Co-morbidity can only partly explain this impaired status (17). Compared with controls, migraine patients were found to perceive more symptoms and greater emotional distress, as well as disturbed contentment, vitality and sleep (18). There is an enduring disposition to attacks and there may be changes in behaviour and mood, long-term adoption of the sick-role with disruption at work, school, and in social roles and sexual relationships (5, 19). Therefore, in many cases, migraine should be considered a chronic rather than an episodic illness (16). These chronic aspects are characterized by how the condition changes an individual's behaviour and induces disability between attacks. It therefore is important to assess the interictal behaviour and mood changes, all the more because a significant relationship may exist between the interictal (limitation of) activity of the patient and the concurrent quality of life – as such a relationship was established during migraine attacks (20, 21).
Until now research related to interictal mood and daily functioning has been based on subjective reports only (4, 14, 17, 18, 22–24). In our study, however, the daily functioning was also recorded using ambulatory accelerometry. In a previous study we have shown that this method, which provides an objective, reliable and valid quantification and classification of the behavioural aspects of daily functioning (such as lying, sitting, standing, physical activities and locomotion) (25–29), is feasible to perform before, during and after a migraine attack (21).
The possible involvement of the autonomic nervous system in migraine mechanisms has long been a subject of interest. Autonomic dysfunction in migraine patients outside attacks usually was studied in vitro (30–32). These studies, including those on heart rate fluctuations, have produced contradictory results. Thomsen et al. observed a mild parasympathetic interictal hypofunctioning with preserved sympathetic functioning (33). Cortelli et al. found no impairment of the autonomic control of the cardiovascular system in migraine without aura in the headache-free interval (34), whereas Pogacnik et al. concluded that the sympathetic function is impaired (35). Results of in vivo studies monitoring the ambulatory heart rate of migraineurs suggested a hypofunction of the parasympathetic nervous system during normal daily activity in the headache-free period (36), or a clear sympathetic instability (32). Heart rate is influenced by changes in postures and movements. By using ambulatory accelerometry it becomes possible to control for the effect of body postures and physical activities on heart rate variability. Therefore, in addition to the parameters mentioned above, we also recorded the ambulatory ECG of the subjects.
The aims of the present study were:
to quantify the normal daily interictal activities of patients with migraine in their habitual environment;
to determine the ambulatory recorded interictal mean heart rate of migraineurs, during the various body postures and physical activities;
to assess interictal subjective symptoms reflecting mood, sleepiness, and level of functioning, in patients with migraine in their habitual environment;
to compare the outcome of all these parameters with that of a control group which had been matched for age, gender and occupation.
Methods
Subjects
Twenty-four migraine patients participated in this study. They were recruited consecutively between 1 November and 31 December 1999 by means of advertisements in the area in and around Rotterdam. These subjects were diagnosed by a neurologist of the Ikazia Hospital Rotterdam (LJMMM) as having migraine (18 patients without aura, four with aura, two with both forms) according to the criteria of the Headache Classification Committee of the International Headache Society (37). For eligibility of the patients, reference is made to the in- and exclusion criteria listed in Table 1. A control group of 24 subjects, matched with the migraine patients for gender and age, was recruited. They were also matched, as much as possible, for type of occupation, on the basis of the inherent general level of daily activity any occupation entails. Fourteen were recruited from (relatives of) faculty members and students of the Erasmus University Rotterdam, in addition to 10 people who responded to local advertisements. They were in good physical and mental health and free from drugs during the study and at least 2 months prior to it. If they had a history of chronic headache complaints, psychiatric illness or alcohol abuse, then they were excluded from the study. So were those who experienced recent circadian shifts, including working at night. The study was conducted at the Erasmus Medical Centre in Rotterdam, the Netherlands, and had received the approval of the Medical Ethics Committee. All subjects provided written informed consent once they understood the nature and scope of the study.
Inclusion and exclusion criteria
Procedures and measurements
During a migraine-free 2-day period, measurements were obtained in the habitual environment of the participant. On the morning of the first day the procedure was explained and the sensors attached. Instructions were given regarding the use of the equipment and the daily log was explained. The following measurements were made.
Accelerometer signals
Four uni-axial piezo-resistive accelerometers were employed to classify static and dynamic activity. The data-acquisition of the accelerometer signals was done by means of a portable digital recorder (Vitaport TM System; TEMEC Instruments, the Netherlands) which was carried on a belt around the waist. For a detailed description of this method of data-acquisition, see our previous publication (21). The static activities comprised three different body postures – lying, sitting, and standing; the dynamic activity three types of movements – general movement (unspecified non-cyclic movements), walking (including climbing stairs), and cycling. The accelerometers were also employed to quantify the time spent in the different body postures or as movements. Furthermore, an index of the motility (motility is defined as ‘the intensity of body segment movements, measured with accelerometry’ (38)) of the body during these different postures (static motility) and movements (dynamic motility) was calculated. The number of postural transitions between lying, sitting and standing was calculated as well.
ECG signal
ECG was recorded from a precordial lead by means of adhesive disposable Ag/AgCl electrodes. The ECG signal was stored at a sample rate of 128 Hz on the Vitaport recorder. In order to analyse heart rate, interbeat-interval (IBI) time series were obtained from the R-R waves of the raw ECG signal. The IBI series were checked for presence of movement artefacts and incidental R-wave detection failures, which were corrected by means of linear interpolation techniques. IBI series were converted to heart rate series; mean heart rate levels were computed of the different classes of body postures and physical activities.
The daily log
During the measurement period, the subjects kept a daily log to document relevant events (start-sleep period; end-sleep period; special types of physical activities or psychological events). The daily log included four brief questionnaires.
Subjective Sleep Quality Scale (SSQ). An 11-true-false item questionnaire to assess subjective sleep quality, to be filled in at breakfast (39).
Stanford Sleepiness Scale (SSS, Dutch translation). The SSS consists of a 7-point scale with items ranging from ‘feeling active, alert’ to ‘cannot stay awake, sleep onset appears imminent’, to be filled in at breakfast, lunch, dinner, and before sleep (40). Subjects were instructed to have their scores at breakfast reflect the period between rising out of bed and taking their breakfast; the other moments of measurement had to reflect the previous period of the day, i.e. morning, afternoon and evening.
Level of Functioning (LOF). The LOF is an ad-hoc constructed, short Guttman Scale on daily functioning with seven items ranging from ‘is only capable of lying on bed’ to ‘is capable to perform heavy physical activities’. The subjects were asked to fill in the LOF questionnaire at the same points in time as the SSS.
Profile Of Mood States (POMS; validated Dutch version) (41). It was used to measure depression, anger, fatigue, vigour and tension. Reliability and validity of the Dutch version proved to be sufficient (41). The POMS was also filled in at the same points in time as the SSS.
The participants were instructed to perform their normal daily activities and to follow their habitual pattern of eating, smoking and drinking during the measurement period, and to avoid abnormal physical and mental exertions.
Data analysis
Because the first day of measurement was considered as a habituation period, the data collected on the second day were used for analysis.
In order to analyse the kinematic parameters, this second day was divided into three intervals: (i) from rising up in the morning till noon; (ii) from noon till 18.00 h; (iii) from 18.00 h till going to sleep. Because the first and third period varied in duration, the proportion of time spent in a posture (summation of lying, sitting or standing) and as movement (summation of walking, cycling or as unspecified movements) during the three periods were computed. To quantify the motility during sitting and standing, the periods spent in these postures while using public or private transport were not included.
Sample size calculation and statistical analysis
The proportion of time being active during the daily periods was a main outcome measure. Therefore, the required sample size was calculated with α= 5% and β= 20%, assuming a minimum difference of five per cent between both experimental groups in the proportion of time spent being dynamically active per daily period. Differences between the migraine and the control group on variables with a normal distribution were tested with the independent-samples T-test; those with a skewed distribution with the Mann–Whitney U-test. Differences between migraine and control subjects were further analysed using binary logistic regression analysis. Predictor variables entered into the regression equation were those variables which revealed a significant difference between the experimental groups at any moment of measurement, namely sleepiness, vigour, level of functioning, relative duration of dynamic activity (the proportion of time spent during dynamic activity), static and dynamic motility, and relative duration of lying down. To reduce the number of tests performed and to improve interpretation of findings, the predictors entered into the regression equation were based on variables reflecting the whole daytime period. The model was estimated using the backward stepwise selection method (Backward: LR). The alpha of the tests was set at 0.05. The analyses were performed with the Statistical Package for the Social Sciences (SPSS for Windows, version 9.0 (SPSS Inc., Chicago, IL, USA)).
Results
Control subjects and patients did not differ in age (P = 0.84) and in male-female ratio. They were also comparable regarding their occupation (see Table 2).
Demographic characteristics of the subjects

Body postures and physical activities
The recording of the kinematic parameters and of heart rate of one patient was not successful. Therefore, the number of valid cases with data on these variables was 23 and those with data on the subjective variables 24.
The statistical tests revealed that the relative duration of dynamic activity (summation of time spent as walking, cycling, or as unspecified movements) of the migraineurs was significantly shorter during the afternoon and during the evening (see Fig. 1). (As the relative duration of body postures is linear, dependent on the relative duration of dynamic activity, scores on this parameter also showed a significant difference between the groups in the same daily periods). The dynamic motility of the patients with migraine was significantly lower during all three daily periods than that of the control subjects (see Fig. 2). Compared with controls, migraine patients were also found to spend a significantly larger part of their afternoon lying down; in the evening, the motility of their body during lying, sitting, and standing (static motility) was significantly lower (see Table 3).
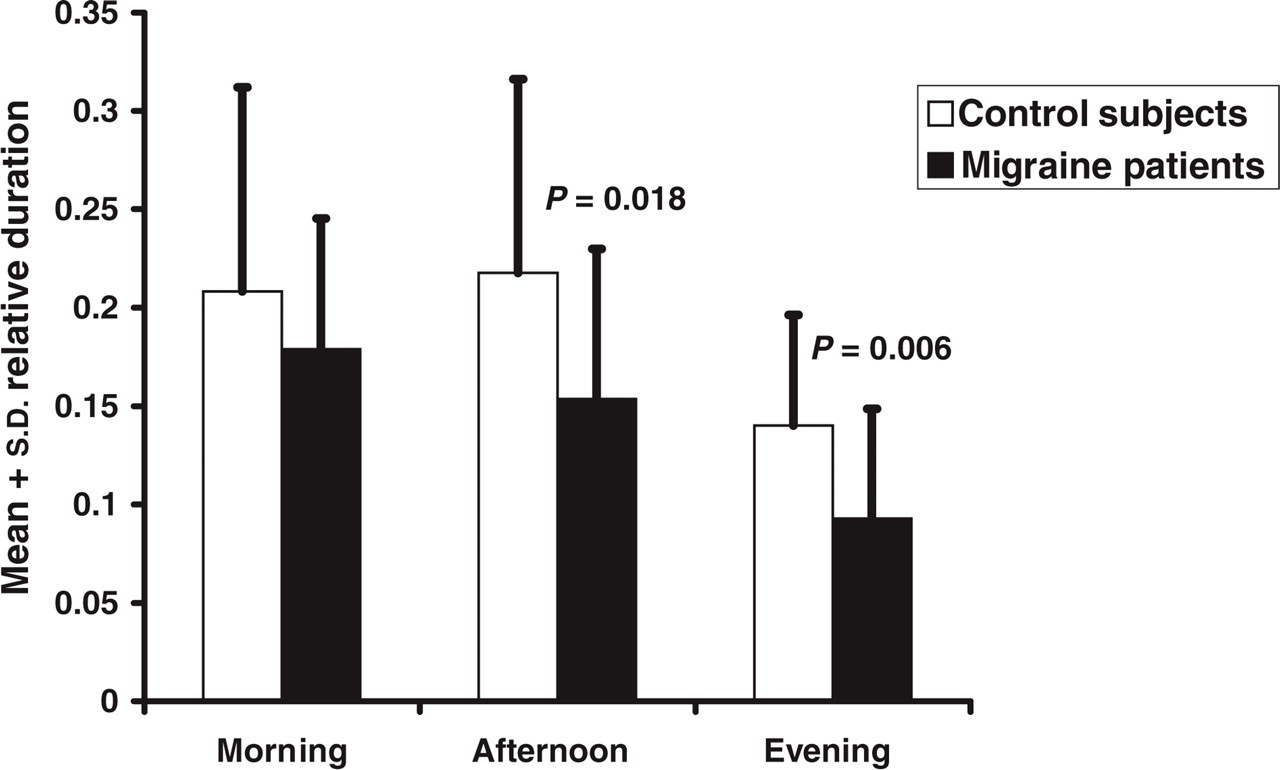
Mean and standard deviation of the proportion of time the control subjects and the migraine patients displayed dynamic activity during the morning, afternoon and evening. Significant differences between the groups during the afternoon (P = 0.018) and the evening (P = 0.006) are also depicted.

Mean and standard deviation of the dynamic motility of the control subjects and the migraine patients during the morning, afternoon and evening. Significant differences between the groups during the morning (P = 0.047), the afternoon (P = 0.016), and the evening (P = 0.025) are also depicted.
Mean (S.D.) of physical activity parameters per daily period, for controls and migraine patients

Trans., transitions; rel., relative duration, i.e. proportion of time spent in that posture.
∗Significant difference between the experimental groups.
Heart rate
For all daily periods, no significant differences regarding mean heart rate levels were observed during lying, sitting, standing, or during dynamic activities (see Table 4). Also, during the night the migraineurs did not significantly differ from the controls on this parameter (mean heart rate of the migraineurs was 66.7 beats per minute (b.p.m.) (S.D. 7.52) and that of the controls 65.1 b.p.m. (S.D. 6.44)).
Mean (S.D.) of heart rate per activity category, per daily period and for controls and migraine patients separately
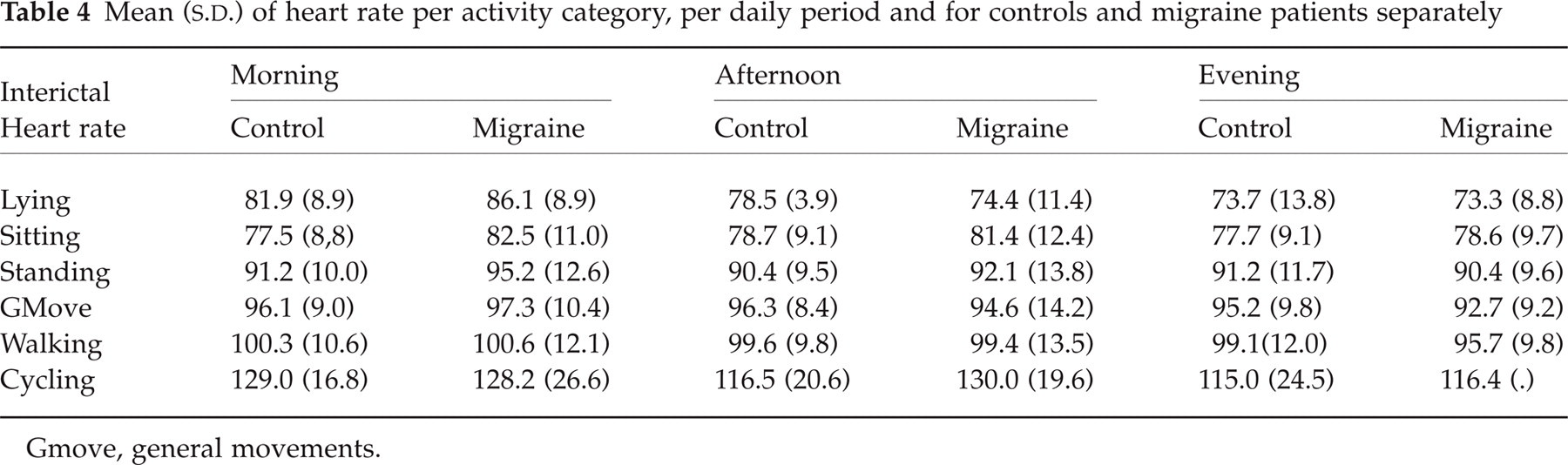
Gmove, general movements.
Subjective daily log parameters
Compared with controls, patients with migraine reported significantly higher levels of sleepiness during the morning and the evening.
In addition, they reported significantly lower realizable levels of functioning (during the morning and the afternoon) and of vigour (during the whole day) (see Table 5). No significant differences were observed regarding the other subscales of the POMS.
Median (interquartile distance) of subjective parameters per daily period, for controls and migraine patients separately

LOF, level of functioning.
∗Significant difference between control subjects and migraine patients.
Logistic regression analysis
The binary logistic regression analysis resulted in a linear combination of the level of sleepiness (coefficient B of this covariate was 1.1902; P = 0.007) and the relative duration of dynamic activity (B =−14.8806; P = 0.006), both variables reflecting the whole daytime period. Entering these covariates into the regression equation resulted in a post-diction of the subject's group classification with an overall accuracy of 75.5% (control subjects with an accuracy of 75%, patients with 76%).
Discussion
Although interictal chronobiological data are now being collected more frequently in headache research (33), the results of the vast majority of ambulatory studies on interictal impact of migraine are based on subjective self-reports. They indicate that the impact of migraine is not restricted to the episode in which the patient suffers from an attack. The current study using the objective, reliable, and valid method of ambulatory accelerometry to classify and quantify overt behaviour confirms this finding, as it indicates an interference of migraine with interictal physical activity. Compared with healthy controls, migraine patients spent relatively less time being active (summation of time spent as walking, cycling, or as unspecified movements). Moreover, if active, the motility of the body was found to be lower than that of the control subjects, i.e. migraineurs appeared to move more calmly and more prudently. Because the level of motility differed between the three types of movement (general movement, walking, and cycling), the aforementioned result could be caused by a difference between both groups in the proportion of time spent during the three modi of movement within the daily periods. Post-hoc analysis, however, did not reveal such differences. The relevance of kinematic parameters in differentiating migraineurs from healthy controls is also apparent from the results of the binary logistic regression analysis. The relative duration of dynamic activity during the day turned out to be one of the two important variables on the basis of which the participant's membership of either the control or patient group could be post- dicted. Interpretation of the results on the kinematic parameters is challenging, because they cannot be compared with those of previous studies, as these parameters have not been measured before (in the same way). All subjects were medication-free and not on any prophylactic treatment during the 48-h period of measurement. Therefore, effects of medication cannot explain the difference in dynamic activity and dynamic motility. Nor can it be attributed to a difference in concomitant feelings of depression or tension – symptoms of depression and anxiety have been claimed to be more frequent among migraine sufferers – because the experimental groups did not differ on these parameters (see Table 5). As a certain level of physical activity is required to exercise a particular profession, the participants of both groups were pairwise matched for occupation in order to level the physical activity of both groups. Moreover, the relative duration of dynamic activities of the control group within the 24 hours of the day used for analysis was 12%. This figure is consistent with those of reference groups configuring in previous research using ambulatory accelerometry (42, 43). Therefore, methodological shortcomings in representativeness of the experimental groups or the comparability between them also cannot be accountable for the observed difference in dynamic activity and dynamic motility between the groups.
But a change in the patients’ behaviour, i.e. an over-the-years-of-suffering acquired habit to anticipate an acute attack might offer an explanation (14). As the aggravation of headache by physical activity is a discriminative feature of a migraine attack (37), migraineurs might try to avoid the aggravation by moving less, and more carefully, explaining the observed reduced ictal dynamic activity and dynamic motility compared with an interictal period (21). Furthermore, the results of this study show that, during headache-free periods, the level of dynamic activity and dynamic motility of migraineurs is still lower than that of healthy controls. So, the ictal behavioural pattern of activity and motility might have been generalized to the interictal periods and have become a (learned) habit, now serving the purpose of avoiding an acute attack. This explanation is in accordance with the results of the study by Cavallini et al. (1995), who conclude that many headache patients experience distress from the imminence of attacks in the intervals between them. This distress pushes them to take the precautions necessary to avoid an attack (5).
The lower level of motility of the patients during physical activity might, however, also originate in a difference in central nervous system functioning. The finding that migraineurs reported to be more sleepy and less vigorous and only able to function at a lower level of activity during daytime (periods) than controls did, and the fact that these results cannot be explained by differences in subjective fatigue (there were no significant differences in fatigue between controls and patients), or by the effects of medication, adds to the plausibility of this assumption. Future research might aim at clarifying this issue by investigating a possible relation between the length of history of migraine and the kinematic and subjective parameters.
Mean heart rate levels during static acivity (lying, sitting, and standing) controlled for body posture and movement, did not differ between the experimental groups. They also did not differ during dynamic activity (general movement, walking, and cycling). In our study, mean R-R intervals were analysed, while in many of the studies referred to, spectral analyses of the beat-to-beat variations were performed. Therefore, although the results of the current study do not confirm previous findings indicating autonomic dysfunction at the cardiac level in migraineurs during headache-free periods, because of the difference between the current and the aforementioned studies in analysing the ECG, they also do not necessarily contradict them.
Because the duration of time since the last migraine attack and that until the next one has not been recorded in this study, the influence of either of these attacks on the results cannot be excluded. However, during the explanation of the study procedure, none of the migraine patients reported a recent attack in the past 48 h. Moreover, although not reported here, the current investigation also consisted of the measurement of two migraine attacks. The measurement in the headache-free period always preceded the ictal measurements. The time elapsed between the interictal and the first ictal measurement varied between 1 week and 4 months. Consequently, the influence of the prodromes of an imminent attack is unlikely as well. As is the influence of a headache on the recorded data: only one patient developed a headache during the evening, scoring 6.7 on a 10-centimeter visual analoque scale.
Finally, adjusments for conducting a large number of statistical tests are recommended to avoid rejecting the null hypothesis too readily. Therefore, the multiple comparisons made in this study without a corresponding correction of alpha might be a cause of concern, that is one or more of the statistical significant differences between the experimental groups reported here might be non-significant, i.e. the hypothesis of no difference is true. This especially holds for those findings with a P-value close to the α. Alternatively, as Rothman (1990 (44)) has pointed out, scientists making adjustments for multiple comparisons may penalize themselves by missing possibly important findings.
In summary, during a substantial part of an interictal day, migraineurs were significantly less physically active than healthy controls. Moreover, when active, the motility of their body was reduced. They also subjectively reported a lower level of realizable activity and of vigour and a higher level of sleepiness. These phenomena might be conceptualized as consequences of a migraine-specific CNS functioning. Alternatively, they may be interpreted as acquired habits to anticipate and/or avoid a migraine attack; particularly with reference to the overt, physical behaviour. Despite the various studies indicating an interictal autonomic impairment, the results of this study did not confirm this position based on heart rate evaluations.
The observed migraine-specific interictal phenomena constitute an important part of the individual and collective impact of migraine. Migraine leads both objectively and subjectively to a limitation in physical activities, also outside attacks. This may result in a reduction of the productivity at work, in school, and in other roles, and consequently in an increase of the indirect costs to society. If so, the interictal behavioural and psychological characteristics migraine patients exhibit, contribute to the individual, as well as to the collective burden of migraine, confirming the chronic impact of this disease.
Footnotes
Acknowledgements
The study was supported by a research grant from GlaxoSmithKline BV; Zeist, the Netherlands.