
Abstract
Objective
To evaluate the prevalence and characteristics of headache and its relationship with comorbidities and lifestyle in a teenage population.
Methods
This is a cross-sectional study. Data was collected from students aged 12–18 years from six different schools in Catalonia, Spain. They completed an anonymous questionnaire with demographic, lifestyle, medical data, presence of recurrent headaches and its features, and completed the Strengths and Difficulties Questionnaire. We defined probable migraine if headache presented ≥ 3 ICHD-3 beta criteria for migraine. An analysis was performed to evaluate headache characteristics and compare lifestyles between those with or without headache.
Results
1619 out of 1873 students completed the survey (response rate 86.4%). From these, 30.5% suffered from recurrent headache and 11.3% had migraine features; 32.9% of adolescents with headache had at least one episode per week and 44.1% showed some degree of headache-related disability measured by the PedMIDAS scale. In a univariate analysis, headache was significantly more frequent in girls (35.1% vs. 25.5%, p < 0.001), teenagers with poor sleeping habits (36.6% vs. 27.6%, p < 0.001), lower physical activity (p = 0.002), those who did not have breakfast (37.3 vs. 28.4%, p = 0.001), smokers (10.5% vs. 4.9%, p < 0.001) and caffeine overusers (30.9% vs. 24.7%, p = 0.009). Comorbidities significantly associated with headache were: allergies (38.8% vs. 29.3%, p = 0.007), other chronic pain disorders (44.7% vs. 27.6% p < 0.001), mental health problems (53.2% vs. 29.0%, p < 0.001) and worse SDQ scores (p < 0.001).
Conclusions
Headache is a common health problem among adolescents which impacts their quality of life. Headache is associated with presence of “unhealthy lifestyle” and other medical comorbidities. Educational initiatives should be started.
Introduction
Adolescence is the transition period from childhood to adulthood. Teenagers experience important physical, psychological and biological changes and live through a great amount of new and challenging experiences. Biologically, adolescence is considered a neurodevelopmental critical period where the brain has a heightened neuroplasticity to adapt its structure and function in response to environmental demands, experiences, and physiological changes (1). Hence, the impact of what happens to the brain during these years may result in neuroplastic changes with long-term consequences.
Headache is a common and disabling health problem that affects all ages. Despite the fact that adolescence is a crucial period of time in the natural history of some primary headaches, there is very little information about the prevalence and impact of headache in teenagers, where it seems to be a common health problem.
Headache is one of the most common neurological disorders in European adolescents, especially in females (2) with an estimated mean prevalence of 54.4% (9.1% for migraine) (3). Besides, headache causes substantial disability in young adults representing the world's seventh most significant cause of disability-adjusted life years (DALYs) in people between 10–14 years old (4). Suffering from headache is related to a poorer quality of life, the presence of attention difficulties and more absenteeism from school and other activities (5). Inconsistent with its high prevalence and headache-related disability, some studies point to a low utilisation of medical care resources by adolescents with headache (6).
Headache may also be associated with several comorbid neurological, psychiatric and cardiovascular conditions in adults (7). Likewise, in children and adolescents it has also been associated with depression and anxiety disorders, epilepsy, sleep disorders, attention deficit hyperactivity disorder and Tourette's syndrome (8). Moreover, some lifestyles are considered risk factors for suffering from headache (9).
The impact of headache in Spanish and European teenagers has not yet been properly evaluated. Our survey-based study done in our adolescent population wants to look into the prevalence of headache in this age group and the disability that it causes, and then analyse the presence of comorbidities and lifestyle it is associated with.
This is of vital importance as we believe that chronic headache disorders, specifically chronic migraine, could be minimised with educational strategies that should already start during the teenage years. Therefore, a better knowledge of the prevalence, impact and lifestyle of our adolescent headache sufferers might enable us to change the impact that headache and migraine have in adults. This is a strategy to promote education in teenagers and globally improve the quality of life of our adolescents and our future adults.
Methods
Study design: This is a cross-sectional observational study. Data was collected from May 2015 to April 2016. The sample size was calculated based on the previously estimated headache prevalence in adolescents (3). Assuming a prevalence of 54% in our population of adolescents, with a margin of error of 2.5%, a 95% confidence level and an expected non-response of 10%, a total of 1697 subjects had to be considered in the study to obtain at least 1527 completed questionnaires.
Participants: The study was conducted in six different high schools in Catalonia, Spain. In order to achieve a population representative sample, the educational sites were selected based on different criteria: Location (spread around the territory), environment (rural/urban) and educational system (private/public system). For all participants, parents or legal tutors were informed and provided informed consent. All students between the ages of 12 and 18 were requested to answer an anonymous survey. The students were provided with clear written instructions to fill the questionnaire, which was administered during school time.
Lifestyles and comorbidities: Questionnaires were designed with a closed-answer structure (yes-no or frequency range options) and were divided into different sections: Demographics, educational performance, daily routine activities, sleeping, exercise and eating habits as well as alcohol and nicotine consumption, medical comorbidities (from a list of the most common neurological and general medical conditions) and regular medication intake.
All participants completed the Strengths and Difficulties Questionnaire (SDQ), Catalan version 11–17 years old. The SDQ is a 25-item based behavioural screening questionnaire, divided into five scales: emotional symptoms (five items), conduct problems (five items), hyperactivity/inattention (five items), peer relationship problems (five items) and prosocial behaviour (five items). Together, the first four scales generate a general difficulties score, in which having a higher score indicates abnormality. In contrast, in the prosocial scale, higher scores are positive (10).
Headache features: We identified adolescents with headache as those who responded positively to this question: Do you suffer from recurrent headaches without an underlying cause as, for example, infection or trauma? (11). Students with headache were asked to complete the last part of the questionnaire with headache features, frequency, headache-related disability (Pediatric Migraine Disability Assessment Scale, PedMIDAS), positive headache family history, medical consultation, and their diagnosis.
We adhered to the criteria for probable migraine of the International Classification of Headache Disorders (3rd edition – beta version) (12) and classified as probable migraine those students with headache and at least three of the follow migraine characteristics: Unilateral pain, headache that interfered with normal activities (moderate-severe intensity), headache worsening with physical activity, photophobia, phonophobia, nausea or vomiting or the presence of neurological symptoms suggesting aura.
Statistical analysis: Descriptive and frequency statistical analysis were undertaken and comparisons were made using SPSS statistical package, version 17.0 for Windows. Statistical significance for intergroup differences was assessed by Pearson's chi-square or Fisher's exact test for dichotomous and nominal variables, linear trend chi-square test for ordinal variables and Student's t-test for continuous variables. Correlations with scales were assessed with Spearman's rank correlation coefficient. Odds ratios (OR) with their respective 95% confidence interval were calculated to establish the individual risk of headache conferred by each one of the significant variables related to headache. Variables associated in the bivariate analysis were entered into an adjusted multivariate logistic regression model to identify factors independently associated with the presence of recurrent headaches in adolescents. The goodness-of-fit of the model was assessed by Hosmer and Lemeshow test. A p-value < 0.05 was considered to be statistically significant.
Ethics: Participation in the study was voluntary. Parents and students were informed beforehand and signed a written statement of consent. The study was approved by the Vall d'Hebron Hospital Ethics Committee (PR(AG)228/2015).
Results
The questionnaire was responded to by 1619 students. This represents 86.4% of the total number of students surveyed. The mean age was 14.4 ± 1.8 years (12–18) and 51.9% were female; 90.4% of students were born in Spain.
A total of 30.5% (494/1619) of students suffered from recurrent headaches and 11.4% (184/1619) fulfilled probable migraine criteria.
Demographics and lifestyle.

p<0.05.
Headache features
From the total number of adolescents with headache, 25.1% described unilateral pain, 30.4% had symptoms suggesting aura (25.5% visual) and 37.2% had headache with photophobia, 56.1% had phonophobia and 14.4% had nausea or vomiting. In 35.4%, headache worsened with exercise. The majority of teenagers suffered from at least one episode of headache per month, 32.9% related one episode of headache per week and 4.5% had daily headache (see Figure 1). In all, 44.1% of adolescents with headache have some degree of headache related disability measured with the PedMIDAS scale (see Figure 2) that showed a positive significant correlation with headache frequency (R = 0.288, p < 0.001).
Headache frequency distribution. PedMIDAS scale categories distribution.

In relation to use of medical care, 37.7% of the participants with recurrent headache had previously consulted a medical specialist about headache. In all, 8.1% of students with headache were aware of the previous diagnosis of migraine, but 73.7% did not know their headache diagnosis.
Lifestyle
Regarding lifestyle habits and their relationship with headache (see Table 1) students with headache showed a significantly higher mean BMI (20.2 ± 3.3 vs.19.8 ± 3.2, p = 0.022) but no statistical differences were found between the frequency of being overweight or obese. Fewer adolescents with headache had breakfast before going to school (70.2% vs. 77.9%, p = 0.001) but we did not find any other differences regarding eating habits.
Despite the fact that 69.3% of adolescents reported regular sleeping habits and slept a mean of 7.7 ± 1.1 hours a day, only 30.3% thought that their sleep was restful enough. In all, 28.4% indicated that they suffered from insomnia and 35.2% referred to daytime sleepiness. Poorer sleeping habits were significantly associated with headache. Students with headache had shorter sleep time (7.6 ± 1.1 vs. 7.9 ± 1.1 hours, p < 0.01) and more frequently had non-regular sleeping habits, insomnia, daytime sleepiness and unrestful sleep (p < 0.001), even when adjusted by sleep time.
Adolescents spent a mean of 3.5 ± 2.3 hours a day on sedentary activities and 13.2% did not do any exercise. On the other hand, 54.8% of students practised sports or gymnastics regularly. Again, teenagers with headache spent more time on sedentary activities (3.8 ± 2.4 vs. 3.4 ± 2.3 hours, p < 0.001) and practised exercise or sports less frequently (p = 0.002).
In all, 6.4% of our sample were smokers, 1.2% consumed alcohol at least many times per week and 26.3% took caffeine regularly. Tobacco and caffeine use was more common in the headache group (tobacco: 10.5% vs. 4.9%, p < 0.001; caffeine: 30.9% vs. 24.7%, p = 0.009). There were no significant differences in alcohol consumption.
Comorbidities
Comorbidities and medication.
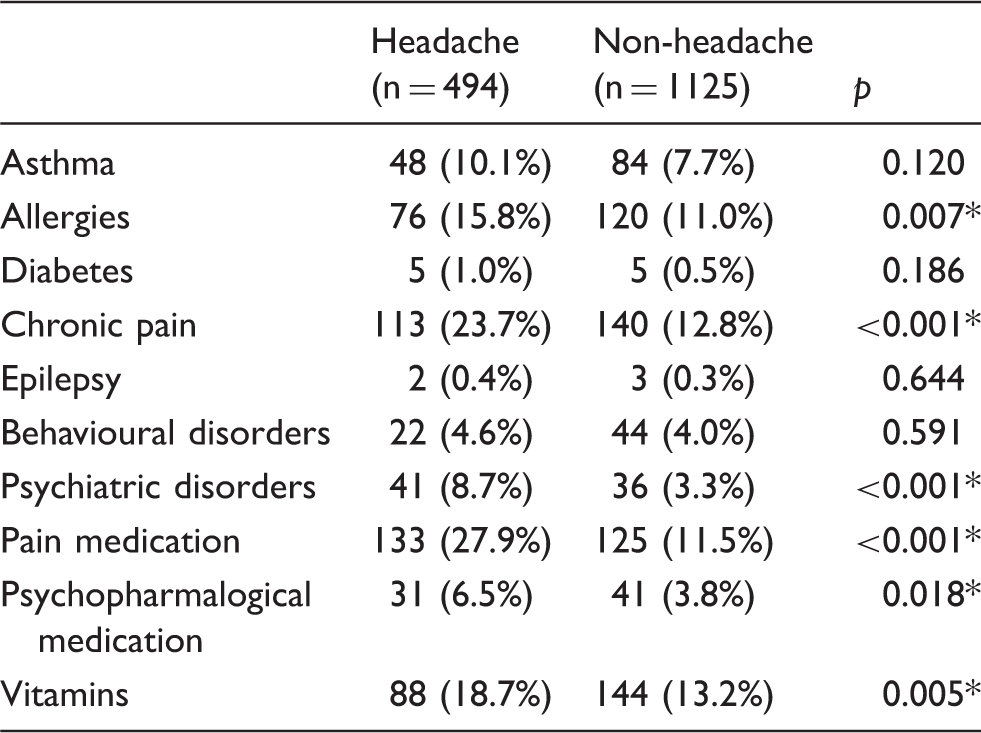
p < 0.05.
When we tried to screen for behavioural disorders with the SDQ scale in all of the participants, 8.0% had an abnormal score in emotional symptoms and behavioural problems, 16.9% in hyperactivity, 2.0% had relationship problems and 3.2% prosocial behaviour. A total of 5.6% of adolescents showed abnormal scores in the SDQ total scale. Figure 3 shows the SDQ scores and compares adolescents who suffer from headache and those who do not. Headache was significantly associated with abnormal scores in emotional, hyperactivity, conduct and relationship problems sub-scales and total score (p < 0.001).
SDQ scores comparison between adolescents with and without headache showing (a) Emotional scale (b) conduct problems scale (c) hyperactivity scale (d) peer relationship scale (e) pro-social scale (f) total scale.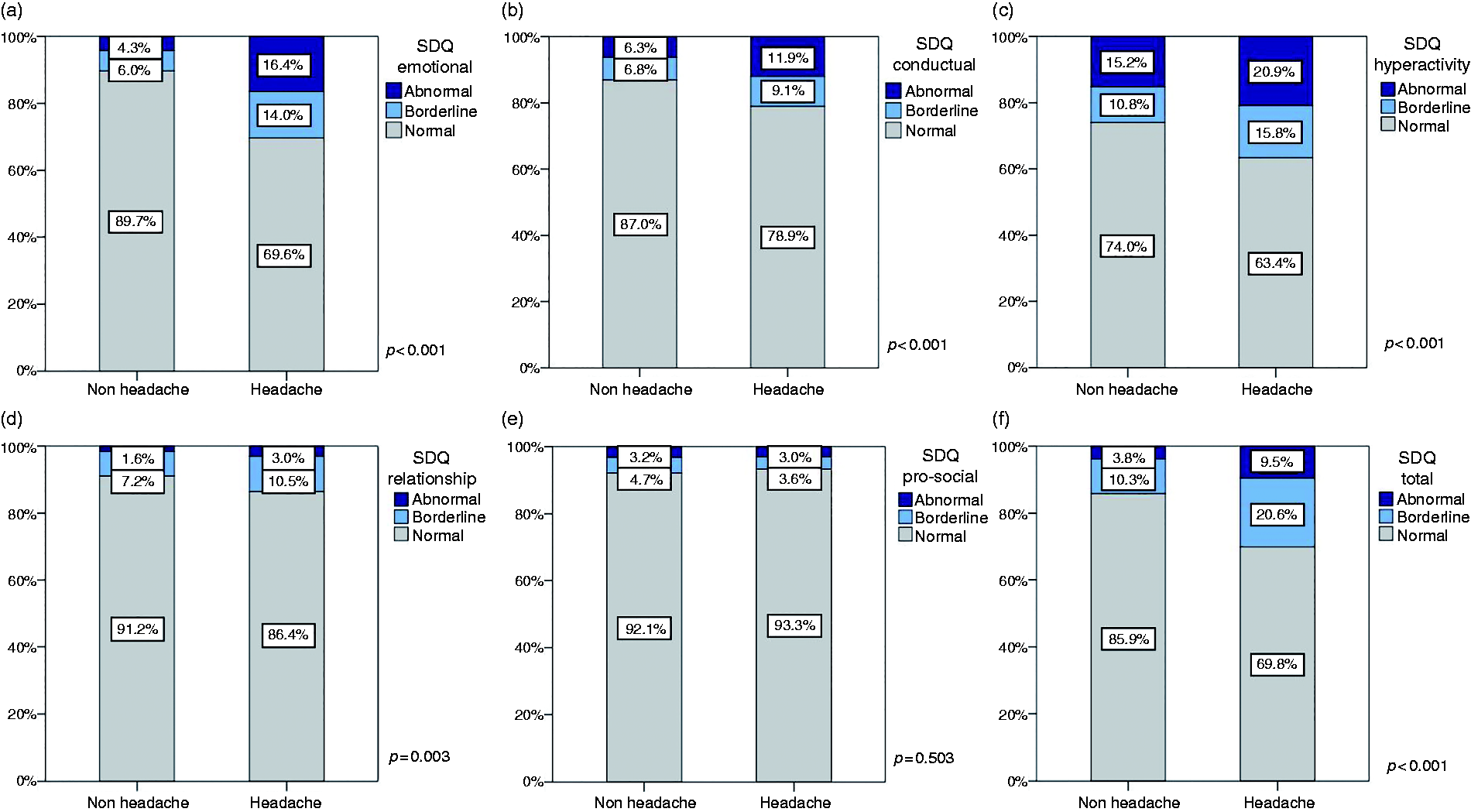
Headache risk factors
Lifestyle and comorbidities individual odds ratios for headache.

p < 0.05.
Multivariate analysis. Factors independently associated with headache.

p < 0.05.
Migraine versus other headaches
In our sample, 494 adolescents had recurrent headaches. From these, 184 had migraine features (40.1%). Compared with other headaches, the presence of a headache family history was significantly more frequent amongst probable migraineurs (81.9% vs. 67.5%, p = 0.002). Adolescents with probable migraine had more frequent attacks (p = 0.072, see Figure 4) and higher headache-related disability (p < 0.001, see Figure 5). In relation to use of medical care, 50.8% of students with probable migraine had previously consulted a medical specialist, which is significantly higher than in the other headache group (32.3%, p < 0.001).
Headache frequency in adolescents with probable migraine compared with other headaches. Disability (PedMIDAS) in adolescents with probable migraine compared with other headaches.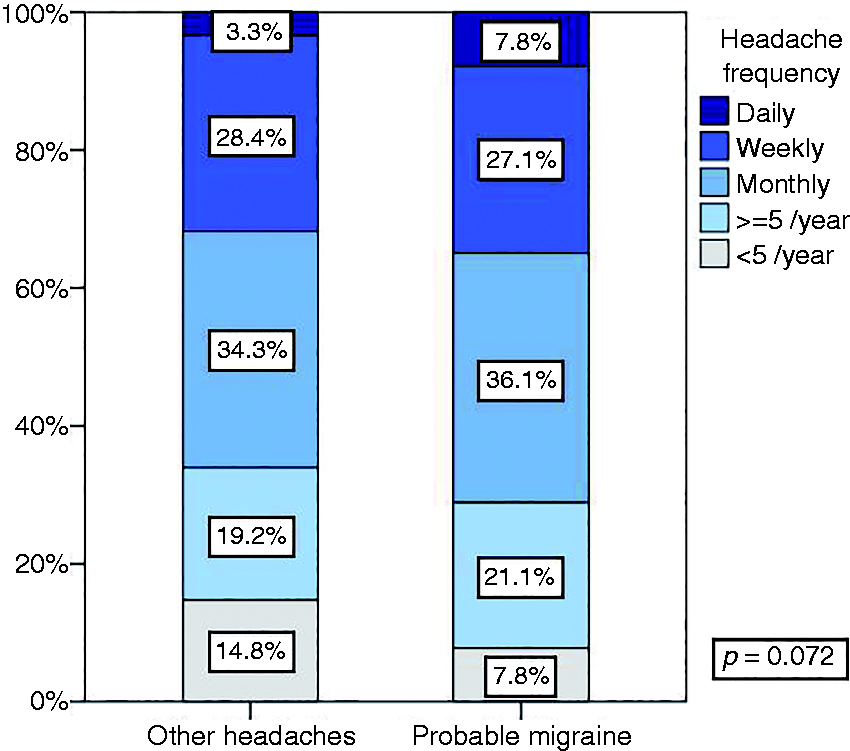

They also presented non-regular sleeping habits more often (p = 0.013) but no significant differences were found related to physical activity or dietary habits.
Teenagers with probable migraine did not differ from the rest in relation to headache comorbidities, but more adolescents with probable migraine had abnormal scores for emotional SDQ (p < 0.001), hyperactivity (p = 0.001), conduct problems (p = 0.001) and total score (p < 0.001).
Age subgroup analysis
As adolescence is not homogenous, in order to better describe possible differences related to age we divided students into age subgroups: 12–13 years old (565), 14–15 years old (545) and 16–18 years old (509). Headache and migraine prevalence increased with age and were significantly more frequent in students between 16 and 18. Headache prevalence was 25.5%, 30.1% and 35.5% respectively (p < 0.001) and probable migraine prevalence was 9.0%, 12.3% and 13.0% (p = 0.04).
The multivariate logistic regression analysis showed that, in younger students (12–13 years old), factors independently associated with headache were being female (OR = 1.681 [1.065–2.653], p = 0.026), higher caffeine intake (OR = 1.797 [1.053–3.068], p = 0.032), comorbid chronic pain (OR = 2.048 [1.186–3.537], p = 0.010) and psychiatric disorders (OR = 6.076 [1.771–20.849], p = 0.004), as well as having abnormal scores in the conduct problems SDQ scale (OR = 4.111 [1.713–9.864], p = 0.002). On the other hand, between 14–15 years old students that showed a higher risk of headache were those with insomnia (OR = 1.749 [1.116–2.741], p = 0.015), sedentary habits (OR = 1.146 [1.046–1.256], p = 0.004), comorbidity with other chronic pain syndromes (OR = 1.843 [1.078–3.151], p = 0.025) and abnormal emotional SDQ scores (OR = 3.685 [1.793–7.575], p < 0.001). Finally, between 16–18 years old, the adolescents with a higher risk of headache were smokers (OR = 2.184 [1.424–3.350], p < 0.001) with insomnia (OR = 1.878 [1.012–3.483], p = 0.046) and abnormal emotional SDQ scores (OR = 3.484 [1.738–6.971], p < 0.001).
Discussion
This is the first population-based study in Catalonia and Spain trying to better describe the prevalence and features of headache in an adolescent population as well as to assess its relationship with other medical comorbidities and lifestyles. These are our findings.
First, headache is a frequent and disabling health problem among adolescents. In our sample, 30.5% of the responders reported suffering from recurrent headaches and 11.4% overall showed migraine features. Headache and probable migraine prevalence seem to increase with age. More than half of the teenagers with headache who participated in the study reported at least one attack per month and 4.5% had daily headache. Although we have little epidemiological data about headache in adolescents, headache prevalence in our sample does not differ from prevalence in survey-based studies in southern European countries (13,14), and probable migraine prevalence is similar to the migraine prevalence for adults in Spain (15). Headache in our adolescents is also associated with disability. In all, 44.1% of our adolescents with headache reported headache-related disability (PedMIDAS score grade II or more). In the line with previous data, our study also shows that headache frequency and disability scores are substantially higher in those students suffering from migraine compared to other headaches (6,16,17).
Previous studies have compared adolescents with other types of chronic pain and headache, showing the latter have the lowest quality of life and largest school absenteeism rate even when reporting lower pain frequency (18). This may be because, apart from physical limitations, headache interferes with their ability to concentrate and creates anxiety for the sufferer and his/her family. Thus, the quality of life in children and adolescents with headache is similar to that seen in other illnesses such as cancer or arthritis (19). Although the economic costs of headache during adolescence are unknown, our study points to a higher utilisation of health-care services and medication use, especially in those with probable migraine, which adds to parents' work absence. Indeed, headache in adolescence also implies important economic costs.
Given the burden, both educational and appropriate therapeutic strategies should be offered and available, and programs should be started to undertake early detection of students at risk.
Second, headache during adolescence is also significantly related to “unhealthy lifestyles”. Headache was significantly more frequent in females and teenagers with poor sleeping habits, lower physical activity, those who did not have breakfast, had a higher BMI, smokers, and caffeine overusers. These modifiable headache risk factors are especially relevant in older adolescents (14–18 years old).
In our sample, non-regular sleeping habits, unrestful sleep, insomnia and daytime sleepiness were significantly more frequent in headache sufferers. It has been reported that children and adolescents who suffer from headache usually have higher rates of sleep disorders such as insufficient sleep, restless sleep and daytime sleepiness. These sleep difficulties could act as cause, trigger or could lead to headache chronification (20). Although sleeping problems are more frequent in adolescents with headache, they also occur in the general adolescent population. Teenagers experience biological and behavioral changes (i.e. use of technology or caffeine) and also have looser supervision by parents, which may lead to unscheduled sleeping routines (21).
Lower physical activity and higher BMI were also significantly associated with headache in our study (9). Although adolescents with headache may avoid doing exercise because it might trigger attacks, physical activity can also be helpful in preventing headache by increasing endorphin levels and general well-being, as well as contributing to a reduction in overweight (22).
Communities have developed physical activity programmes for child and adolescents fundamentally to prevent obesity, cardiovascular risk factors and osteoarticular disorders. Exercise may improve headache but also anxiety and depression symptoms, social development and avoidance of tobacco, alcohol and drugs, which can have an effect on headache (23). Hence, headache prevention should be another target of parental and school-based educational programmes centred around sleep hygiene and physical activity.
Finally, headache has previously been associated with cardiovascular and atopic disease as well as other neurological or psychiatric disorders such as depression, anxiety, epilepsy, sleep disorders, attention deficit hyperactivity disorder and Tourette's syndrome (24). In our study, adolescents with headache also suffered from other medical conditions such as allergy, other chronic pain disorders, and mental health problems. Regarding psychological comorbidities, we used the SDQ scale to screen comorbid psychological conditions. SDQ has proved to be a useful tool in the initial assessment of psychopathology in children with recurrent headaches (25) and adolescents with headache presented worse scores in total SDQ, specifically in emotional, conduct symptoms, hyperactivity and peer relationships. Numerous studies have been focused on the relationship between headache and anxiety-depression disorders in children and adolescents. The nature of this relationship is still not clear. There is an increased risk of anxiety disorder in adolescents with migraine compared to those without migraine (26), but on the other hand headache is the most frequent somatic symptom in adolescents suffering from anxiety, depression and behavioural disorders (27).
Medical and especially psychiatric comorbidities increase the burden of disease in young people with headache, so use of holistic approaches should be considered, taking into consideration comorbid conditions as well.
The strengths of our study are the large sample size and high participation rate. The study also has limitations that should be considered when interpreting the findings. Headache and probable migraine diagnosis was made based on the survey. Although we used closed questions with easy examples to try to characterise headache features well, this may lead to the possibility of over or underestimating headache and migraine prevalence. The use of self-reported information might not be reliable for some aspects such as, for example, alcohol consumption, but the fact that it was an anonymous questionnaire was intended to minimise this bias. The study was performed in six different schools around the country in order to have a very heterogeneous sample; however, there was less participation from rural areas and from students that, after secondary mandatory schooling (16 years old), did not continue with their formal studies.
Conclusions
Headache is a common health problem among adolescents. Adolescents suffering from recurrent headache have frequent attacks that impact on their quality of life, just like adults. During adolescence, headache is associated with non-regular sleeping and eating habits, low physical activity, smoking and caffeine use as well as other medical comorbidities such as allergy, other chronic pain disorders, and mental health problems.
It is essential to educate teenagers on healthier lifestyles and good sleeping habits, and raise awareness of the impact of headache and migraine during adolescence as it is when lifestyle habits are adopted.
We would recommend that educational programmes for teenagers should be encouraged with the support of the International Headache Society. These initiatives would be the first preventive treatment to avoid the increase of headache frequency and the impact of headache in the development of teenagers. We believe this could lead to a healthier adulthood, minimising headache chronification and increasing wellbeing.
Footnotes
Contributors
PPR and MTF made substantial contributions to conception and study design. MTF, CVS, SA and JBG worked on acquisition of data. MQL and VJG contributed to analysis and interpretation of data. MTF wrote the first draft. PPR, AM and JAS critically revised and finally approved the version to be published. All authors fully comply with and approve the version to be published.
Article highlights
Headache is a frequent and disabling health problem among adolescents that is significantly related to “unhealthy lifestyles”.
Adolescents with headache also suffer from other medical conditions that reduce their quality of life.
Headache, especially migraine, is associated with emotional, conduct, hyperactivity and peer-relationship symptoms that are correlated with disability.
It is essential to educate teenagers on healthier lifestyles and raise awareness of the impact of headache and migraine during adolescence, as this will lead to controlled headache in adulthood.
Acknowledgements
The authors would like to acknowledge the students and teaching team from IES Josep Brugulat, Banyoles, Girona; IES Llavaneres, St Andreu de Llavaneres, Barcelona; IES Laia L'Arquera, Mataró, Barcelona; Col·legi Salesians, Mataró, Barcelona; Oak House School, Barcelona; and IES Berenguer d'Entença Hospitalet de l'Infant, Tarragona.