
Abstract
Introduction
Cluster headache is a rare primary headache syndrome with well-defined diagnostic criteria (1). A major concern to the clinician is the exclusion of secondary cluster-like head pain which may be amenable to specific therapy. Atypical clinical signs and symptoms which suggest symptomatic cluster headache include absence of typical periodicity, presence of background headache between the episodic exacerbation, refractory pain, presence of neurological signs other than miosis or ptosis (2, 3).
We present a patient with cluster-like headache, responding to ergotaminic preparations, and related to a central cervical spinal cord cavity and an Arnold–Chiari type I malformation.
Case report
The patient, a 36-year-old female, complained of recurrent headache of 6 months’ duration. The pain was localized in the right frontal and supraorbitary area and internal nasal border, was described as very intense and excruciating in quality, and lasted about 20–30 min. It was accompanied by tearing, facial oedematous sensation and on occasions a slight right eyelid drooping was noted. Nasal obstruction, secretion, and conjunctival injection were not noted.
The pain recurred irregularly two to three times per day, but did not appear during the night. During the pain attack, the patient felt the need to sit still, since movements worsened the pain. Although it usually appeared spontaneously, she was able to precipitate the pain by putting her head in a low-down position. The pain did not respond to regular analgesics such as aspirin (600 mg) or paracetamol (1000 mg), but she noted a quick response to oral ergotaminic-caffeine preparations (1.0 mg dihydroergotamine, 80 mg caffeine). Although the patient was not a regular drinker, after moderate alcoholic ingestion the pain recurred more frequently. Prophylactic treatment with oral indomethacin 25 mg/8 h was ineffective. After treatment with methyl-prednisolone 48 mg/day (10 days) and a 1-month taper, she noted some improvement in pain threshold, and the pain attacks were more tolerable. The neurological examination was normal.
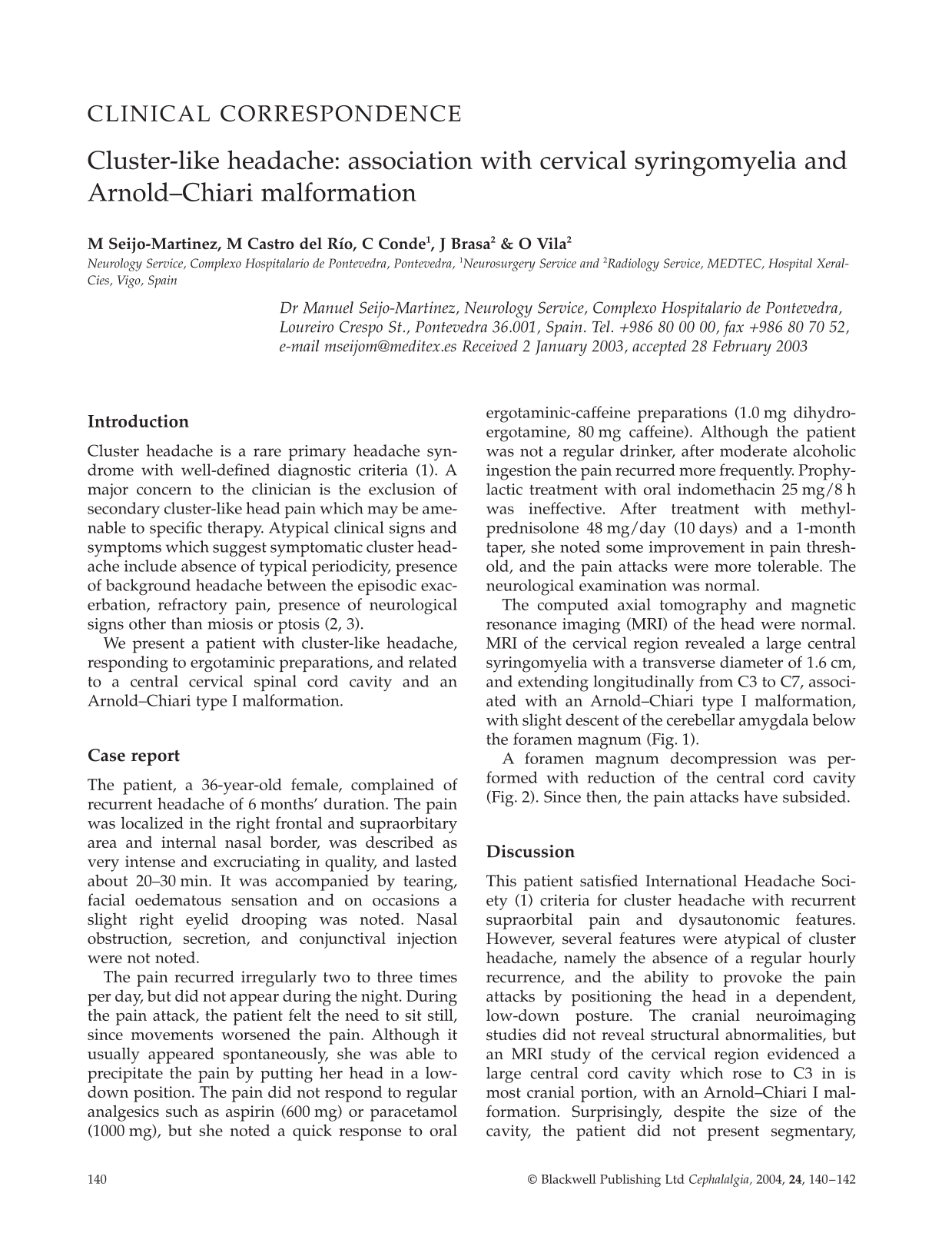
The computed axial tomography and magnetic resonance imaging (MRI) of the head were normal. MRI of the cervical region revealed a large central syringomyelia with a transverse diameter of 1.6 cm, and extending longitudinally from C3 to C7, associated with an Arnold–Chiari type I malformation, with slight descent of the cerebellar amygdala below the foramen magnum (Fig. 1).

Magnetic resonance imaging T1-weighted image. Cervical syringomyelia, extending from C3 to C7. Arnold–Chiari type I malformation.
A foramen magnum decompression was performed with reduction of the central cord cavity (Fig. 2). Since then, the pain attacks have subsided.

Magnetic resonance imaging T1-weighted image. Post-foramen magnum decompression. Extensive reduction of the central cord cavity.
Discussion
This patient satisfied International Headache Society (1) criteria for cluster headache with recurrent supraorbital pain and dysautonomic features. However, several features were atypical of cluster headache, namely the absence of a regular hourly recurrence, and the ability to provoke the pain attacks by positioning the head in a dependent, low-down posture. The cranial neuroimaging studies did not reveal structural abnormalities, but an MRI study of the cervical region evidenced a large central cord cavity which rose to C3 in is most cranial portion, with an Arnold–Chiari I malformation. Surprisingly, despite the size of the cavity, the patient did not present segmentary, long tract motor-sensory signs or sphincter dysfunction.
We believe that the central cervical cord lesion was responsible for the recurrent cranial pain, for the following reasons:
There was a high clinical suspicion for a secondary cluster headache.
The topographic, characteristic onion-skin distribution of the spinal nucleus of V was consistent with the location of the pain. The spinal nucleus is divided in three subnuclei (oralis, interpolaris and caudalis), and there is a somatotopical arrangement with the perioral area represented in the rostral part of the subnucleus and the more lateral regions of the face more caudally (4).
The patient could provoke the pain attacks with simple postural-mechanical manoeuvres. This symptom is highly suspicious of the presence of underlying structural disease, especially mass lesions. Arnold–Chiari I malformations are frequently associated with syringomyelia, and may cause Valsalva manoeuvre or effort-induced headache; however, the headache is characteristically suboccipital or occipital, and bilaterally irradiates to frontotemporal regions (5). In our patient the pain was not precipitated by coughing or straining, but specifically by placing the head in a low-down position. Although patients with Arnold–Chiari I malformation present headache which varies with postural changes, it is not always precipitated by this manoeuvre. In addition, the descent of the cerebellar amygdala below the foramen magnum was of low magnitude in our patient.
The trigeminal-autonomic cephalalgias (6), which include cluster headache, paroxysmal hemicranias, SUNCT and hemicrania continua, are a group of recurrent primary headaches of brief duration, sharing a common pathophysiological mechanism, namely the activation of the trigeminal nerve and cranial parasympathetic outflow through the trigeminal–autonomic reflex. We speculate that, in the present case, discrete dilatations of the cord cavity induced a mechanical irritation of the upper cervical segments and consequent activation of the more caudal portions of the spinal trigeminal nucleus, which may descend to C2–C3 level. The pain attacks responded to dihydroergotamine. Various extra-axial cervical lesions have been associated with cluster-like headache, including cervical trauma (7) and meningiomas (8), possibly by activation of the trigeminal–autonomic reflex. Recent reports indicate that medullary infarcts may present as a cluster-like attack (9, 10). A novel therapeutic option, which may have been useful in this patient, is greater occipital nerve blockade. This technique offers a good–moderate response in most patients, is well tolerated and free of adverse effects (11).
This case indicates that when the suspicion of a secondary cluster head is firm, exclusion of lesions in the trigeminal nucleus caudalis by cervical cord imaging may be warranted.