
Abstract
We investigated the use of self-administered pain-relieving manoeuvres on a sample of 400 patients with primary headaches—represented by an even distribution of migraine without aura (MO), migraine with aura (MA), episodic tension-type headache (TH), and cluster headache (CH)—consecutively seen at Padua and Parma Headache Centres. Manoeuvres on various regions of the head were used by 258 patients (65% of the cases). The most applied procedures were: compression (114 out of 382 manoeuvres; 30%), application of cold (27%), massage (25%) and application of heat (8%). A significant (P < 0.001) relationship was found between headache diagnoses and type of manoeuvre. In MO patients the application of cold (38% of the manoeuvres) and compression (36%), used mainly on the forehead and temples, prevailed; compression, mainly on the temples, was the most frequent procedure (44%) in MA patients. Massage on the temples and nape was the predominant manoeuvre (43%) in TH patients, whereas in the CH group, which more often required heterogeneous procedures, none of the above-mentioned manoeuvres was prevalent. Compression, as a diagnostic criterion for MO, had a sensitivity of 33% and a specificity of 86%; for the application of cold the figures were 36% and 84%, respectively. Massage had a sensitivity of 33% and a specificity of 80% for TH. The efficacy of the self-administered manoeuvres in reducing pain was scarce. Only 8% of the manoeuvres, in fact, resulted in a good or excellent pain control. Moreover, the efficacy of the manoeuvre was often momentary, wearing off when the manoeuvre stopped. In spite of this, 46% of the subjects used the manoeuvres constantly, at each attack.
Keywords
‘Oh Gods, Gods, why do you punish me? Yes, there’s no doubt, it's her, always her, the horrendous disease, invincible … migraine … there's no way of fleeing from her, I'll try not to move my head …'
The Roman governor of Judea Pontius Pilot had the instinct to get up and place one of his temple under a water stream. But he knew that with this he would not have obtained any relief …
Introduction
It is a common observation, by clinicians involved in the headache field, that many patients use some instinctive manoeuvres, of their own accord that tend to alleviate their suffering. These self-administered procedures have not been suggested by the physician or other therapist and are used constantly by some patients even if, for their limited efficacy, they at best result in supporting the pharmacological therapy.
Starting with our clinical experience, it seemed to us that this behavioural aspect of headache patients had never been adequately studied. We therefore investigated this phenomenon with three aims: (i) to evaluate its actual frequency; (ii) to examine its eventual value as an additional diagnostic criterion for migraine without aura and tension-type headache; and (iii) to verify its usefulness in alleviating the pain.
Patients and methods
Patients
Four hundred adult (18–65 years) patients suffering from primary headache were interviewed during a year at Padua and Parma Headache Centres. The sample was made up of 100 consecutive patients with migraine without aura (MO), 100 with migraine with aura (MA), 100 suffering from episodic tension-type headache (TH) and 100 with cluster headache (CH), diagnosed according to the criteria of the International Headache Society (1).
Two hundred and fifty-two patients (63%) were female, 148 (37%) were male. There was a female preponderance in the MO group (female 82%, male 18%), in the MA group (female 72%, male 28%) and in the TH group (female 74%, male 26%), while in the CH group the proportions were inverted (female 24%, male 76%). The mean age was 35.7 ± 10.2 years.
Questionnaire
All the patients answered a detailed questionnaire concerning the use of self-administered pain-relieving manoeuvres. The questionnaire was administered by two well-trained neurologists (PR, LF). The interobserver reliability was tested on a sub-sample of 20 patients (five for each diagnosis) and was satisfactory (kappa=0.84 for the use of manoeuvres).
The following information was collected:
Use of one or more manoeuvres, strictly self-administered.
If a manoeuvre was used:
Frequency of use of the manoeuvre, expressed as number of attacks during which the patient resorted to the manoeuvre (out of a total of 10).
Type of manoeuvre and location of application.
Efficacy. This parameter was defined on the basis of the manoeuvre's capacity to reduce pain, on a percentage basis, assuming a 100% pain before the application of the procedure.
Consistency of efficacy, evaluated by figuring the number of attacks out of 10 that the manoeuvre proved successful.
Duration of efficacy, defined as the minutes of persistence of the improvement from the end of the manoeuvre.
Analysis
The variables analysed were qualitative, ordinal and nominal. Some variables were recoded for a better management. In particular:
The frequencies of use of the manoeuvres were broken down into the following categories: rare (1–3 attacks out of 10), fairly frequent (4–6), regular (7–9), constant (10).
The manoeuvres used in combination were singularly inserted into their respective groups (‘compression’, ‘cold’, ‘massage’, ‘heat’, ‘other’), to avoid a spreading of the data.
The efficacy of the manoeuvres in reducing pain was recoded according to the following rates: none (0% of pain reduction), poor (1–25%), fair (26–50%), good (51–75%), excellent (76–100%).
The duration of efficacy was categorized as follows: momentary (cessation within 5 min from the end of the manoeuvre), brief (6–15 min), prolonged (16–180 min), persistent (the relief lasted up to the end of the attack).
The relationships among the variables were analysed using the chi-square test (nominal variables) and the Kruskal–Wallis test (nominal vs. ordinal variables).
The sensitivity and specificity of the most used manoeuvres were calculated to study their validity as an additional diagnostic criterion for MO and TH (considering the diagnosis of MO and TH made according to the criteria of the IHS as the ‘gold standard’).
Results
Use of manoeuvres
Of all the subjects interviewed, 258 patients (65%) resorted to one or more manoeuvres during headache attacks. With reference to the type of headache, 82% of the patients of the CH group used manoeuvres, making this the most numerous group; then followed groups MO (65%), TH (61%) and MA (50%). The percentage of procedures used varied in a significant manner with the type of headache (P < 0.001). There was not a significant difference in manoeuvre use in relation to gender or age.
Frequency of use
Among the 258 patients who used pain-relieving procedures, 119 subjects (46%) constantly used them, for each headache attack: 59% of the CH group, 54% of MA, 38% of TH and 34% of MO. Moreover, 11% resorted to these manoeuvres regularly (from seven to nine times out of 10); 23% used them fairly frequently (from four to six times out of 10), and the remaining 20% used them rarely (from one to three times out of 10). The relationship between the frequency of manoeuvre use and the type of headache was statistically significant (P < 0.005).
Type of manoeuvre (Fig. 1)

Type of manoeuvres used.
The manoeuvres used can be grouped into five typologies.
Compression. Performed with the hand, finger, with the aid of a solid object, against circumscribed points of the head, or with a handkerchief wrapped tightly around the head.
Application of cold. This consisted of applications that ranged from a cold hand, to a wet cloth, to an ice bag.
Massage. This was strictly self-administered (massage performed by a third party was excluded), consisted of a soft and superficial manipulation restricted to regions of the head and for the most part was performed using the fingers.
Application of heat. This was applied on ample zones of the head, the most common source was either scarves or foulards; in some cases, sources of dry heat were used, such as a radiator or hairdryer; in two cases, moist heat (hot shower) was used.
A group of a certain number of varied and sporadic manoeuvres, rendering further subdivision into groups impossible. They were used mainly by CH patients and were: motor activity, smoking cigarettes, hyperpnoea, eructation, self-induced vomiting, closing one nostril, blowing the nose, covering the painful ear, covering part of the head with a pillow, bending forward, and rotating the head to one side.
Sometimes a combination of the manoeuvres listed above were applied simultaneously. The most frequent combination was made up of compression plus cold, usually applied with a tight handkerchief, soaked in cold or icy water.
The manoeuvres amounted to 382, more than the total number of patients who used them (258 subjects). In fact, 93 patients (37 with CH, 26 with MO, 16 with TH, 14 with MA) used from two to five manoeuvres during headache attacks at separate times or simultaneously in combination. The most-used manoeuvre was compression (n = 114, 30%), for 22% of the cases applied in conjunction with other procedures. Next ranked were the application of cold (n = 102, 27%) and massage (n = 98, 25%). Consequently, heat occupied a much lower percentage (n = 31, 8%). Thirty-seven manoeuvres (10%) made up the ‘other’ category, as described above, consisting of a group too mixed and numerically under-represented to form distinct subgroups.
The most frequent simultaneous application of different procedures consisted of compression and cold (12 out of 31 cases); next were ranked massage and compression (nine cases).
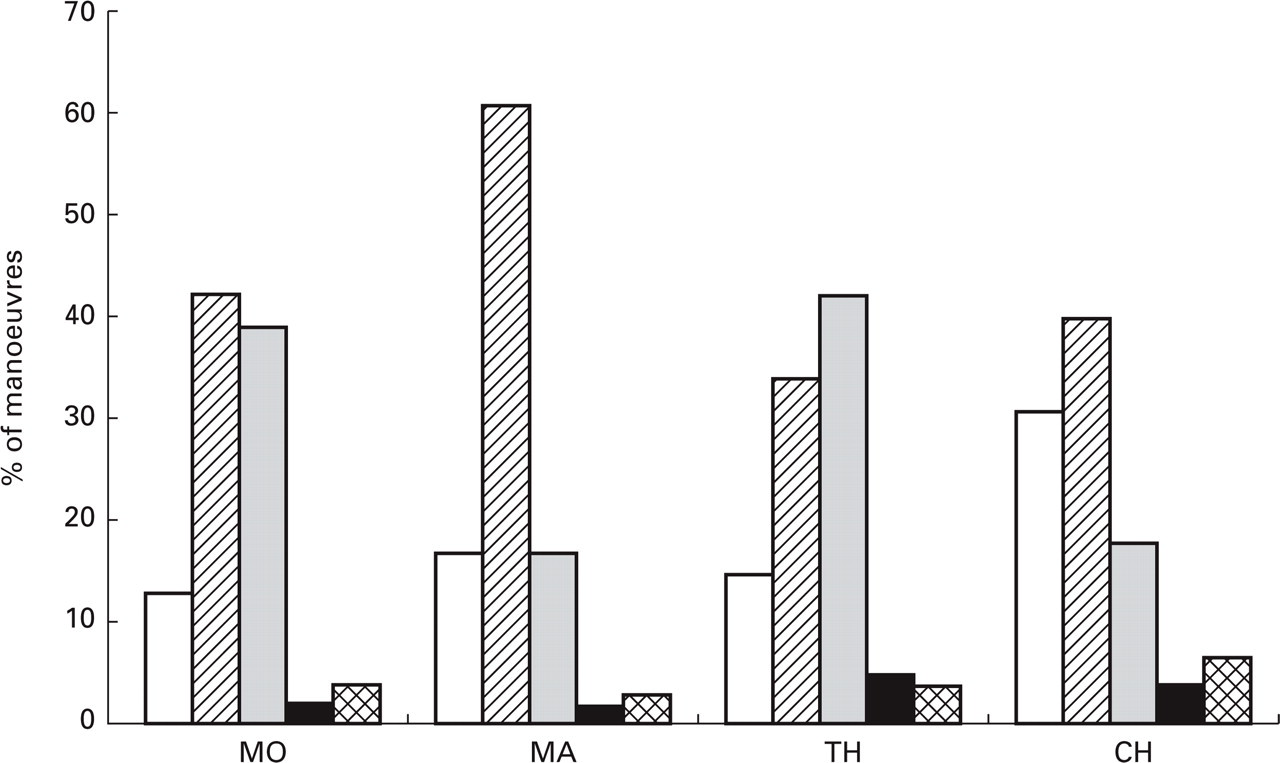
Type of manoeuvre according to the headache type (Fig. 2)

Type of manoeuvres used according to the headache type. The frequency of the different manoeuvres varied significantly (P < 0.001) between the headaches forms. MA vs. MO: P = n.s. MA vs. TH: P = 0.003. MA vs. CH: P = n.s. MO vs. TH: P = 0.0001. MO vs. CH: P = 0.0001. TH vs. CH: P = 0.01. MO=migraine without aura; MA=migraine with aura; TH=tension-type headache; CH=cluster headache.
There was a highly significant relationship between the type of headache and the type of manoeuvre (P < 0.001). In MO patients the most-used manoeuvres were application of cold (38% of the manoeuvres) and compression (36%); then followed massage (21%) and, used to a much lesser extent, application of heat (2%) and other procedures (3%). Out of 65 MO patients using manoeuvres, 53 (81.5%) utilized application of cold and/or compression. In the MA group, compression was by far the most used manoeuvre (44% of the manoeuvres); out of 50 patients using manoeuvres, 28 (56%) applied compression. Next came application of cold (23% of the manoeuvres), massage (20%), application of heat (7%), and other (6%). In the TH group massage clearly led (43% of the manoeuvres; 33 out of 61 patients using manoeuvres); then, used to a much lesser extent, were cold application (20%), compression (17%), and heat application and other manoeuvres used equally (10%). In the CH group the leading manoeuvre was compression (28% of the manoeuvres), followed by cold application (24%), massage (21%), and heat application (11%). We noted that the heterogeneous manoeuvres were used the most (16%) by patients with this type of headache.
Site of application
The sites of application (n = 472) outnumbered the manoeuvres (n = 382), since some manoeuvres were applied in more than one region. The sites of application can be put into 11 groups, reported in Table 1. The manoeuvres were administered almost exclusively to regions of the head; only in a minority of the cases (n = 26; 5.5%) did they involve extracranial areas and, mostly, did not have a precise localization. These are manoeuvres such as physical exercise, motor restlessness, smoking, hot shower, self-induced vomiting, hyperpnea, and closing of one nostril. Some sites were utilized simultaneously, in groups of two or three, during a single manoeuvre. The most-used groupings were forehead-temple and temple-orbit.
Sites of application of the manoeuvres according to the headache type

Site of application according to the headache type (Table 1)
In the MO group the most frequent location was the temple (41%), followed by forehead (31%), neck/nape (11%) and vertex (8%). In the MA group as well the principal locations were the temple (32%) and the forehead (30%), followed by the orbit (16%) and the neck/nape (6%). In the TH group, the locations on the temple prevailed (41%), followed by those on the neck/nape (24%) and on the forehead (19%). In the CH group, three locations had about the same frequency: orbit, temple and the forehead. As far as the groupings of the above-mentioned manoeuvres are concerned, the most frequent combination (forehead plus temple) was present in 12% of the MA group, 9% of MO, 8% of TH and 3% of CH group. The excessive spreading of the data did not allow a statistical analysis of the relationship between the headache type and the sites of application of the manoeuvres.
Sensitivity and specificity of the most used manoeuvres in MO and TH
The manoeuvres that were evaluated were compression and application of cold for MO and massage for TH, of course including even those patients that did not use any manoeuvre. The sensitivity of compression for the diagnosis of MO was 0.33, while the specificity was 0.86; for the application of cold the figures were 0.36 and 0.84, respectively. The sensitivity of massage for the diagnosis of TH was 0.33 with a specificity of 0.80.
Efficacy of the manoeuvres
Of all the manoeuvres performed, 304 out of 382 (80%) presented a certain efficacy, while the remaining 78 (20%) were completely ineffective. The effective portion, however, was largely represented by manoeuvres that had only a poor (165 manoeuvres; 43%) or fair (108 manoeuvres; 29%) ability to reduce the initial pain. Only 31 manoeuvres (8%) exerted a good (12 manoeuvres; 3%) or excellent (19 manoeuvres; 5%) result. Considering the most effective manoeuvre performed by each patient, 35 out of 258 patients (13%) applied only completely ineffective manoeuvres, while 25 patients (10%) were ‘responders’, reaching a good or excellent pain control. Quite surprisingly, some patients continued to perform completely ineffective manoeuvres together with highly effective ones.
Efficacy of the manoeuvres according to the headache type (Fig. 3)
Efficacy of the manoeuvres according to the headache type. The percentage of completely ineffective manoeuvres was higher in CH than in the other three groups (P = 0.03). MO=migraine without aura; MA=migraine with aura; TH=tension-type headache; CH=cluster headache. None=0% of pain reduction; poor=1–25% of pain reduction; fair=26–50% of pain reduction; good=51–75% of pain reduction; excellent=76–100% of pain reduction.
The percentage of completely ineffective manoeuvres was similar in MO (13%), MA (17%) and TH (15%) groups, while it was higher in CH (31%) (P = 0.03). Nevertheless, in the CH group the manoeuvres that resulted in a good or excellent result were more frequent (11%) compared with MO (6%), MA (5%) or TH (9%), even though the difference was not statistically significant. Considering the most effective manoeuvre performed by each patient, 21% of the CH patients applied only completely ineffective manoeuvres compared with 6% of MO, 12% of MA and 13% of TH patients (P = n.s.). Conversely, 15% of the CH patients obtained a good or excellent result, compared with 8% of MO, 4% of MA and 10% of the TH patients (P = n.s.). The complete disappearance of pain was obtained by five CH patients and by one patient in each other category.
Efficacy of the manoeuvres according to the type of manoeuvre
Considering the type of manoeuvre, the percentage of those that presented some efficacy is the following: compression (85%), heat application (77%), cold application (75%), massage (74%), other (74%); in the simultaneous application of two manoeuvres the percentage of efficacy increased to 94% (P = n.s.). A good or excellent result, however, was obtained only in 9% of the compression manoeuvres, in 6% of the heat application, in 6% of massage and in 4% of cold application. The best results were obtained by the heterogeneous group of manoeuvres that provided a pain relief greater than 50% in 24% of the cases (P = 0.005), followed by the simultaneous association of manoeuvres (13%).
Most effective manoeuvres according to the headache type
Taking into account only the manoeuvres capable of bringing about a reduction of pain greater than 50% (8% of all the manoeuvres), in the MO and MA groups no manoeuvre was remarkably effective, except for the two out of three ‘other’ manoeuvres performed by MO patients. In the TH group, the most effective manoeuvres were compression (3/14; 21%) and ‘other’ (2/8; 25%). In the CH group, finally, the most effective manoeuvres were ‘other’ (5/22; 23%), compression (5/36; 14%) and application of heat (2/17; 12%).
Duration of well-being
Out of 304 manoeuvres with some efficacy, 153 (50%) provided only a momentary benefit that wore off immediately when the manoeuvre was stopped or within the first 5 min. A brief (6–15 min), prolonged (16–180 min) or persistent (till the end of the attack) relief was reported in 15%, 12% and 23% of the cases, respectively.
Consistency of efficacy
One hundred and ninety-six out of 304 effective manoeuvres (65%) invariably showed their proper efficacy every time they were used, while the remaining 108 (35%) had a less consistent efficacy, ranging from one to nine out of 10 attacks. The consistency of efficacy was higher in the CH and MA groups, in which 79% and 70% of the manoeuvres were always effective, respectively, compared with the MO (52%) and TH (55%) groups (P < 0.0001).
Discussion
There are many reports concerning the use of non-pharmacological treatments in patients affected by primary headaches. In particular, a remarkable space is occupied by local treatments that can be partially self-administered by headache sufferers, such as compression on regions of the head and/or neck (2–6), cold applications (7–13) or cold packs on the head (10, 14) and massage (15–18). Nevertheless, the literature concerning exclusively self-administered pain-relieving manoeuvres is scarce, even if the first descriptions are very old. Already in Egyptian papyri, in fact, the use of bandaging one's head to alleviate headache is reported (19) and in a monograph of the beginning of the 19th century, the author, suffering from migraine, describes the manoeuvres of compression that he used on precise points of the head during the attack (20).
Compression is the best documented manoeuvre in the literature. Following the pioneering study of Graham and Wolff (2) on the relationship between migraine and the dilation of extracranial vessels, other authors (3, 4) evaluated the effect of compression on the branches of the superficial temporal artery and/or common carotid artery, singling out subgroups of patients according to the response from one or another manoeuvre. Lipton (5) reported the possibility of blocking the algic phase of a MA attack by digital massage of the superficial temporal arteries during visual aura in a small group of patients.
Some mention of the use of thermal applications, whether cold or hot, in the treatment of migraine can be found as early as the 19th century (7, 21). In the light of these observations and personal clinical experience, some authors have worked up particular devices that use, separately or in combination, compression, cold or heat to alleviate migraine. Among these, it is worth mentioning the ‘Head-Band’ (6), an elastic band secured around the head with Velcro and firm rubber discs inserted under the band, used to apply local pressure over the area of maximum pain. The author reported a reduction of pain from 50% to 100% in 55 attacks out of 69 (23 patients). The association between intense cold and moderate compression are the basis of the ‘CHAMP-Cold-Wrap’ (11), an elastic bandage equipped with an ice-pack, effective in 29 out of 45 patients (65%) affected by migraine with or without aura or mixed headache. Only in 16 patients (36%), however, was the pain relief greater than 50%. Another device is the ‘Cold-Comfort’ (9), that uses a frozen gel pack applied not on the head, as with the previous devices, but to the lower extremities. It was reported to be effective in 80% of the migraineurs and in 71% of all the patients studied (migraine, cluster headache, mixed headache). The most complicated device is the ‘Migra-lief’ (10) in which a compression band on the vertex, heat or cold on the head, shoulders, abdomen or feet can be alternatively used according to the patient's need. The device was effective in 15 out of 20 migraine patients, and in six out of seven tension-type headache patients.
Notwithstanding these interesting observations— carried out, however, in open trials on a limited number of subjects—the spontaneous use of self-administered manoeuvres was the object of only one study (6), that considered 100 patients affected by MA or MO (no distinction was made), without mentioning if the criteria of the International Headache Society (1) were used for the diagnosis. Ninety-two out of 100 patients reported use of self-administered manoeuvres, 78 of which consisted of compression performed on the temples (90%), the forehead (5%) or the suboccipital region (5%).
The present study is, to our knowledge, the first one devoted to evaluate, in a large sample of patients suffering from all the main forms of primary headache (MO, MA, TH, CH) the spontaneous application of self-administered pain-relieving manoeuvres, trying moreover to quantify their use, frequency of usage and efficacy. Our investigation has some limitations. First of all, it was carried out on patients referring to tertiary centres, not representative of the general population of headache sufferers. Therefore, the generalizability of our results is limited. Secondly, we did not pick up the data prospectively. It is well known that recall bias may occur in retrospective studies, rendering some data not too precise. More reliable results could be obtained by a prospective study using daily diaries. We found that most patients (258/400; 65%) resorted to one or more manoeuvres. Not surprisingly, the patients who more frequently resorted to one or more manoeuvres (82%, with a mean of 1.4 manoeuvres per patient) were those with CH, in whom the pain is more severe and often unbearable. On the contrary, the patients with MA, in whom the pain is often less bothering than the aura, were those who less frequently resorted to the manoeuvres (50%, with a mean of 0.7 manoeuvres per patient).
The major part of the manoeuvres assessed (382 in total) can be grouped into four clear typologies: compression (30%), application of cold (27%), massage (25%), and application of heat (8%). A fifth group gathers 10% of miscellaneous manoeuvres, too marginally represented to form their own subdivisions. Of all the manoeuvres, 8% were performed in simultaneous combination.
The type of headache from which the patients suffered was significantly (P < 0.001) related to the type of manoeuvre they chose. In the MO group there was a frequent use of cold application (38% of the manoeuvres) and of compression (36%), performed mainly on the forehead and the temples (72% of the sites of application), even though their efficacy was scarce. Patients with TH clearly preferred massage (43% of the manoeuvres), which they used in most cases on the temples (41% of the sites of application) and on the neck/nape (24%). These two regions were the most involved in the TH group, regardless of the type of manoeuvre; the neck/nape, in particular, was by far preferred by TH patients compared with the other headache groups. Massage, although much used, nevertheless did not have an efficacy higher than the other manoeuvres. The patients affected by MO and TH therefore seemed to instinctively resort to different manoeuvres, independently of their efficacy. The sensitivity of the most used manoeuvres (compression and application of cold for MO and massage for TH), however, is too low to allow their utilization as a diagnostic criterion, since most cases of both headache types would not be detected. Their good specificity (0.86 for compression and 0.84 for application of cold in MO; 0.80 for massage in TH), instead, could be of some utility in confirming a diagnosis in the cases (not uncommon in the clinical practice) in which the differentiation between MO and TH is difficult.
In MA patients, the manoeuvre most frequently used was compression (44% of the manoeuvres), despite its inefficacy. The temples (32% of the sites of application) and the forehead (30%) represented the preferred site for manipulation in these patients. Among the CH patients, there was a slight preference for compression (28% of the manoeuvres) over application of cold (24%) and massage (21%). It is worth noting, however, that these patients often (16%) reported using the unusual manoeuvres labelled ‘other’. The most frequent were: motor activity, hyperpnoea, lateral rotation of the head, covering one ear, and closing the nostril ipsilateral to the painful side. Five patients, moreover, compressed the carotid artery ipsilateral to the pain, in the laterocervical region, even if such a manoeuvre was totally ineffective. The sites of application of the manoeuvres mostly corresponded to the painful area, considering that temple, forehead and orbit accounted for 64% of the total sites.
The efficacy of the manoeuvres was scanty—most manoeuvres had only a poor or fair effect—and often momentary. Nevertheless, more than half of the patients applied them regularly or constantly. Moreover, 47% of the completely ineffective manoeuvres were applied constantly. Therefore, it is clear that such manoeuvres were not used on a rational basis, but for a quasi-instinctive need to touch the painful region. Also, the choice of one manoeuvre over another neither reflected a perspicacious trial-and-error experience of different manoeuvres, then selecting the most effective, nor an imitation of expedients recommended by other people. Even though the patients interviewed were not able to indicate why one manoeuvre was chosen over another, it can be hypothesized that they felt particular and almost unconscious ‘sensations’, repeating themselves from attack to attack, that guided them in the choice of a particular manoeuvre.
Compression, for example, especially when applied on the temples (probably in correspondence to the frontal branch of the superficial temporal artery) or in the laterocervical region (on the common carotid artery), could be dictated by the need to oppose a vasodilation and/or a painful throbbing. In fact, beginning with the historical observation of Graham and Wolff (2), vascular compression was repeatedly used in migraineurs for either speculative or therapeutic purposes (3, 4). When applied in connection with pericranial or cervico-nuchal muscles, it could be consequent to the perception of a hypertonus or muscular spasm, even if deep pressure on the musculature can actually increase the tonus.
Application of cold is sought after during the attack, most likely following a sensation of cutaneous heat. Areas of increased dispersion of heat have in fact been documented by thermography in CH patients and in subgroups of migraineurs (4, 22). Moreover, Iversen et al. (23) demonstrated, by using a high frequency ultrasound, that the lumen of the superficial temporal artery was wider on the painful than on the non-painful side during a migraine attack, thus suggesting a local vasodilatory response. A vasoconstrictive action has for a long time been attributed to the cold, mediated, according to some authors (24), by the sympathetic system, and followed by a reactive vasodilation. It is thought, moreover, that moderate cold slows the speed of conduction of the nerve fibres (25). This effect, acting on the fusal fibres, could contribute to reduce the muscle spasm by a reflex pathway (26). If applied at extreme temperatures (< 0°C), the cold could also have an analgesic action by the presynaptic block of nociceptive afferences, according to the gate control mechanism (27–29).
Heat, instead, can give a sensation of well-being in the conditions of cutaneous vasoconstriction, this too observed by thermography in migraineurs (4, 22, 30). Furthermore, a generalized vasoconstriction (except for the superficial temporal artery of the affected side) was noted in migraine patients during a painful attack, by means of a high-resolution ultrasound machine (23). If applied on muscular masses, heat determines a superficial vasodilation, accompanied by a reduction in temperature in the deeper layers which could contribute to the pain relief (31).
A superficial and soft massage is capable of relieving muscular tenderness, probably through the activation of a reflex of muscle tonus reduction (32). Moreover, in some cases it can reduce the oedema of the pericranial and cervical musculature, with consequent reduction of the pressure on pain-generating structures (33). It is less likely that in the brief self-administered massage there is a plasmatic increase of β-endorphins, as hypothesized for the connective tissue massage (34).
The headache relief reported by some patients after hyperpnoea, as after smoking, can be linked to the vasoconstrictive effect on the microcirculation (35).
In the covering of the painful area there is probably a generic protective action with respect to external stimuli (air, light, noise).
Self-induced vomiting in some cases, as already noted by Blau (36), is capable of resolving a migraine attack, for reasons that are not quite clear, among which perhaps are mechanisms of alimentary intolerance (37).
However, in all the four groups of headache patients studied, there remains, beyond any possible interpretation, an almost ritual component, that nourishes the use of the manoeuvres, so much so that the frequency of use does not necessarily correlate with the measure of pain relief obtained.