
Abstract
Background: As part of the course requirement for a post-graduate acute care pediatric nurse practitioner program, a patient/family education project was presented using health literacy principles to support the materials developed. The project represents previously implemented materials for a newly developed pediatric colorectal program; this is a retrospective synthesis. Purpose: Understanding and including the population served when designing, implementing, and evaluating health information and services are imperative in emerging health literacy foci. Previously health literacy focused on patients and their skills or deficits that were then linked to health outcomes. Later the focus shifted to the clinician's rigor and skill in communication. New developments in health literacy shift the focus from skills, public, and staff to an emphasis on the interplay of the environment, which either limits or facilitates health literacy. Methods: Pediatric colorectal care gap analysis from 2018–2021 for the state where the program was created provides a needs assessment of the population of interest. A descriptive narrative of the process for designing, implementing, and evaluating health literate services is presented. Information on current literature and materials to integrate health literacy principles is explored. Conclusion: This article contributes to a need for more available literature on developing health literacy in pediatric colorectal program development and care. The findings challenge clinicians to incorporate health literacy best practice attributes in healthcare environments and monitor and use quality improvement methods that address health disparities.
Keywords
In the first quarter of 2018, the then President/Chief Operating Officer of a 309-licensed-bed, free-standing children's hospital in South Florida wanted to create a Pediatric Colorectal Center (PCRC) at the facility. This program would treat children with diagnoses such as anorectal malformations (ARM - birth prevalence of one in 3000 live births), Hirschsprung disease (HD – occurs in approximately one in 5,000 live births), fecal incontinence (FI – occurs in 75–90% of children admitted to hospitals with constipation; in patients with ARM it varies mainly on the type of malformation but can be as high as 60% and in approximately 40% of children after an HD pull-through; in spina bifida, FI varies by type but can affect about 60% of those afflicted), and idiopathic or functional constipation (prevalence of three to five percent in children aged four to 17 years, a most common cause of abdominal pain in pediatric ED visits, 10% of all pediatric office visits) (Ahmad et al., 2022; Dworschak et al., 2017; Freeman et al., 2017; Librizzi et al., 2017; Minneci et al., 2019; National Organization of Rare Diseases, 2017; Rajindrajith et al., 2021).
From October 2016 through July 2017, 867 ambulatory procedures at centers not specialized in pediatric colorectal care were performed in Florida. The total sum of these charges was $13,961,249 with a payer mix of 44% commercial insurance, 54% Medicaid or other governmental payers, and 2% considered to be other, self-pay, or non-payment (three out of 867) (B.G., personal communication, November 18, 2022). During that same timeframe, 1,504 discharges from inpatient (IP) stay for pediatric colorectal diagnoses generated cumulative charges of $66,234,452 in Florida. The payer mix for these patients was 35% Commercial, 59% Medicaid or other governmental payers, 5% self pay, and 1% considered other or non-payment. While the charges do not represent reimbursement, they showcase the market for patients ages 0–21 without a premier PCRC in Florida.
In May 2018, a pediatric surgeon, hospital administrator, and this author (a nurse practitioner [NP]) traveled to Nationwide Children's Hospital in Columbus, Ohio, to visit the Center for Colorectal and Pelvic Reconstruction (CCPR) that Dr. Marc Levitt, a world-renowned pediatric colorectal surgeon, and their team had created. The vision for the South Florida (SFL) team was a collaborative model to evaluate and manage this underserved patient population in Florida using a multi-disciplinary approach. Unfortunately, children across the country and beyond with these conditions often undergo secondary and additional procedures to correct the initial procedure (Ahmad et al., 2022; Bischoff et al., 2017; Wood et al., 2020). Many variables are related to this, including specialty surgical training and optimal outcomes (A-laish et al., 2020; Rentea et al., 2020; Vilanova-Sanchez et al., 2020). Fortunately, the SFL surgeon had formal training in pediatric colorectal surgery. The NP has treated patients with FI and constipation for the last ten years after attending the well-known colorectal course led by Dr. Alberto Peña and Dr. Levitt. Therefore, the SFL team had the opportunity to aid the children of South Florida further and beyond with this knowledge and skill set. The program was created to incorporate all facets across the care continuum, including but not limited to outpatient (OP), IP, surgical procedures, psychosocial care, multi-specialty care collaboration, research, family assessment, and care navigation. Children who require pediatric colorectal services are born or develop conditions that require lifelong medical management. They need ample resources for continuing care long past any surgical procedures.
In August 2018, the SFL PCRC officially launched. Within five months of operation, the program achieved 340 IP days, 215 OP visits with ancillary testing at each visit, and 34 operating room procedures with a contribution margin of $445,577. One of the divisions within the CCPR (Nationwide) that the SFL team aimed to enhance further was the Bowel Management Program (BMP). Most PCRCs offer a monthly BMP, a coordinated plan of care executed in collaboration with the family over seven to nine days. The patients receive multiple OP ancillary tests such as abdominal X-rays, contrast enemas, and office visits to ensure results and goals are met: daily bowel movement with no soiling issues and abdominal X-ray demonstrating an empty colon. Approximately 10% of BMP patients require surgery; thus, such a program drives surgical volume – a point of interest to an administration considering creating such an offering. The SFL BMP (retention enema) program is an IP stay (only one dedicated full-time employee [NP], no dedicated case management, or insurance coverage for OP BMP supplies); the IP stay pays roughly $10,000 from Medicaid, and the variable costs are approximately $3,500, meaning a contribution margin of $6,500 per case. This does not include potential revenue from patients that may translate to surgical repair.
Needs Assessment
The patient-family education project was identified when the SFL PCRC was opened. The SFL PCRC leadership, marketing department, and administrative lead requested specific deliverables: an online service line webpage with a program welcome, appointment access portal, educational videos, patient education resources, 24/7 e-mail healthcare provider (HCP) accessibility for families, and diagnosis vignettes. Nursing specialty unit leadership (manager, director, and educator) and nurse deliverables included custom patient-family education, pre-operative checklist pathways, booklets, and specialty education (didactic and skills stations). The pediatric surgery attending staff and fellows deliverables included protocols for standardization of care (procedure, diagnosis-based, medical admission, specific colorectal radiographic studies, and sennosides and other BMP medications) and didactic and skills station simulations for the nine advanced practice providers (APP).
There needed to be educational materials for many of the procedures and services offered. The current SFL children's hospital website was reviewed to ensure materials were not already available. The Pediatric Colorectal and Pelvic Learning Consortium [PCPLC] (2022) [www.pcplc.org] member organizations’ websites were reviewed extensively, and the SFL NP contacted many PCPLC APP representatives. Although the APPs were willing to share their stories and help with questions, many of their patient-based resources were considered proprietary; Nationwide did provide their post-operative surgical protocols. Patient feedback from the last ten years was also reviewed: no designated webpage, clear HCP contact information, videos, pictographic information, and information resources outside HCP consultation. This extensive analysis, combined with the goals of the SFL PCRC leadership, yielded materials unique to the SFL program, and all of these deliverables were provided.
Review of the Literature
Two crucial paradigms related to pediatric colorectal care are health literacy (HL) and the burden of therapy. HL has two constructs, personal and organizational. Personal HL is defined as “the degree to which individuals can find, understand, and use information and services to inform health-related decisions (HRD) and actions for themselves and others” (Healthy People, 2020, para 5). Organizational HL is defined as “the degree to which organizations equitably enable individuals to find, understand, and use information and services to inform HRD and actions for themselves and others” (Healthy People, 2020, para 6). Personal HL is an essential coping strategy for patients and families with chronic illnesses (Mackey et al., 2016). Heijmans et al. (2015) reported an increased emphasis on individual self-management in chronic disease, concluding that HL needs to be tailored to the patient's specific context, noting that high-order skills (communicative and critical) are more important than functional skills (reading, writing). Patients and families undergoing a BMP have lived the devastating effects of FI and have not responded to conventional therapies (Halleran et al., 2019; Nash et al., 2020; Reck-Burneo et al., 2018). Many have reduced adherence leading to increased use of healthcare resources, high healthcare costs, and morbidity and mortality (Librizzi et al., 2017; Mantel et al., 2019; Rollins et al., 2022). The Burden of Treatment Theory, proposed by minimally disruptive medicine scientists May et al. (2014), postulates that additional demands are placed on patients with chronic illness, creating a proactive “patient-hood” that requires increased accountability and self-actualization. A vital interaction exists between functional ability and individual, relational capacity (ability to garnish cooperation and coordination from others), and informational capital (May et al., 2014). Ryan et al. (2020), representing adults with ARM or parents of children with ARM, further expand on this by urging HCPs to understand that “colorectal diagnoses do not exist in a vacuum, and theoretical ‘best care’ often differs from the care that provides the best overall quality of life for the patient” (p. 5)—again emphasizing context across the complexity of individual needs and coping strategies. An additional burden facing this population is that the anatomical location of these conditions is considered private, layered with the associated stigma leading to shame, anxiety, and isolation (Ryan et al., 2020). The parents and caregivers of young or adolescent BMP patients tend to clamor for a social connection while the patient faces significant vulnerabilities, both trying to normalize the diagnosis (Tvedte et al., 2021). Parents often become their children's information sources (Bray & Sinha, 2017). Social media and online sources become the gateway of normalization, social support, comparison, patient empowerment, dissatisfaction with healthcare or HCPs, and referral networks (Perkins et al., 2021; Smailhodzic et al., 2016). Reppucci et al. (2022) identified 96 Instagram and 57 Twitter accounts and 94 Facebook pages or groups dedicated to pediatric colorectal information sharing. Support groups used Facebook (45.7%) as their primary platform, Instagram (74%) provided personal account story sharing, and Twitter (35.1%) was most used by HCP. Regrettably, information found in social media or internet sources is often not reviewed nor routinely adheres to standards of scientific methodology, hence the potential for misinformation (Reppucci et al., 2022; Ryan et al., 2020; Suarez-Lledo & Alvarez-Galvez, 2021). Therefore, developing HL-informed communication must prioritize the needs and variables of the pediatric colorectal population to ensure successful ongoing outcomes.
Description of Project and Goals
The project's intended audience is patients and families needing a BMP (retention enema, not a laxative trial, which is another component of a BMP). The BMP is an intense program that patients and families must understand and agree to for success. A BMP requires a daily, hourly dedicated commitment by the patient and family to perform the retention enemas to empty the colon and remain free of fecal soiling for 24 h. Because of the high financial yield of this program, patient education efforts were focused here first. The following were created based on this needs assessment: (a) a professional video demonstrating the retention enema procedure by the program NP (Nicklaus Children's Hospital, 2019), (b) a Microsoft PowerPoint (PPT) primer presenting the program, program members, goals, and demonstration of the procedure (a different format than video), dietary recommendations, admission details, and patient-family reporting procedure, (c) custom discharge education with frequently asked questions (FAQs), and (d) stool log with an example on the first sheet (Figure 1).
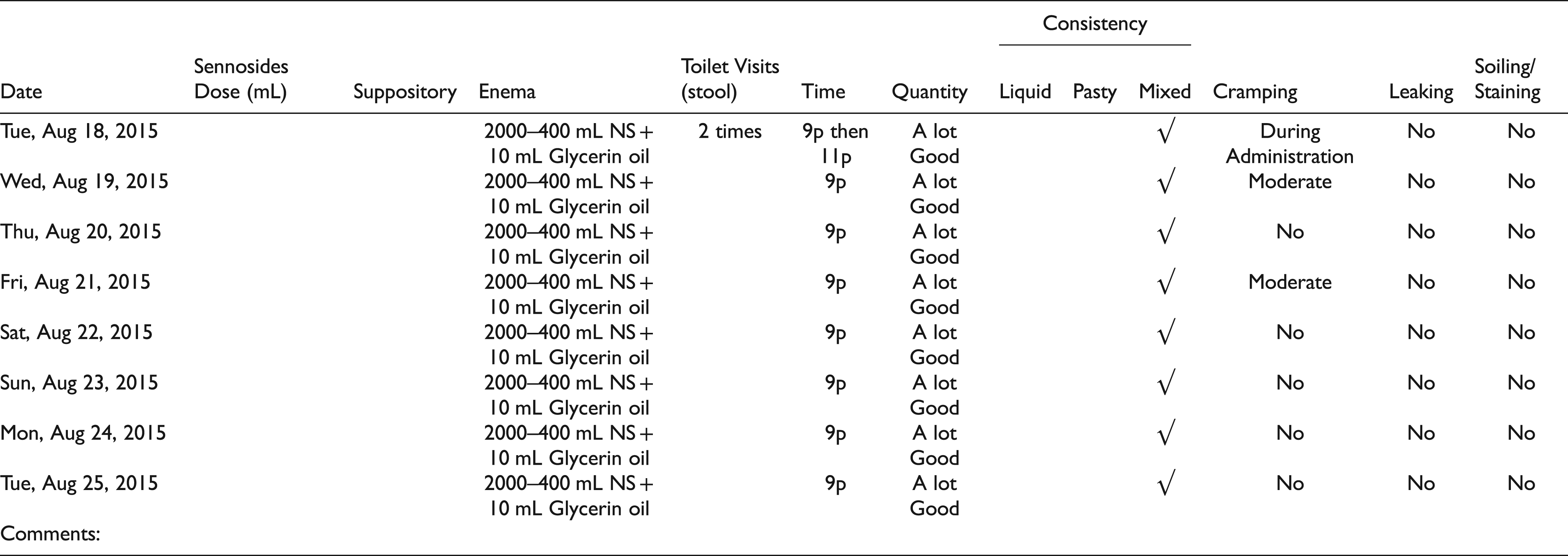
Daily/Weekly Stool Log.
The goals are two-fold. The first is to educate and provide a platform of transparency for the patient and family to understand and ask questions regarding the program before agreeing to this challenging commitment (considering the burden of treatment). The secondary goal is that the materials are a briefing for education and query by those involved in the patient's care (nurses, HCP, child life, nutrition services, case management, and social work, to name a few). The materials are introduced at the OP visit or when the family decides to pursue the BMP. The materials are sent to the family via e-mail, text, or written format for an at-home review. For those patients and families that do not have access to view or read these materials, the information is provided via the GetWellNetwork® (2022) in the patient's room upon arrival. Once the family has reviewed all materials, the PCRC NP goes over the materials again, answers questions, and reviews the family's understanding. The NP then demonstrates the procedure (with the patient) while reviewing the FAQs in real-time; after the NP performs the retention enema, the NP sits with the family and patient again to review any questions or concerns. The following day the designated family member does a return demonstration, and again, FAQs are reviewed. This is repeated daily until discharge, usually two to three days post-return demonstration.
Objectives
The family member will demonstrate how to perform the retention enema procedure comfortably and successfully.
The family and patient will evaluate the program's success by using the daily log to document the goals of their individualized plan.
Improve patient and family quality of life by achieving individualized bowel management.
Describe the Brochure/Teaching Sheet
The rationale for the format selected was based on feedback over the years regarding no videos available on the retention enema procedure, both by parents and HCPs. The scoping review described above supported this family input. The project deliverables used principles of teach-back/
show-back methodology, a vital HL tool (Agency for Healthcare Research and Quality [AHRQ], 2020a), and other universal HL strategies: simplifying and organizing information, plain language and verbal counseling, demonstration, written information, pictographic and video instructions (Morrison et al., 2019). Different modalities were used to reinforce, supplement, and open the door to other conversations. The video demonstration by the NP was a priority item identified post this review. The marketing, biomedical, and legal departments did not require the video script in plain language. However, the NP used plain language and did not rush through to ensure the video script was easy to follow and allowed for real-time questions (allowing the recording to pause). A mannequin was used. The video was made available on the PCRC web page.
The PPT primer was developed to explain the admission and tests ordered, provide positioning pictographs, images of equipment, and constipating or non-constipating food choices. It served to provide dialogue for the patients and parents. The FAQs Microsoft Word document was used for discharge education and included HCP contact information. One type of serif font was used throughout, with larger same font headings, left justification, and bulleted lists; paragraphs were short, and the information was presented in chunks, with sufficient space to make the pages less dense and inviting to read (Covering Kids & Families, 2005). WebFX (2022), a readability tool found in the U.S. Department of Health and Human Services (HHS) HL Resources (2022), was used for both of these formats. The PPT had a Flesch Kincaid Grade level of 8.6, a Flesch Kincaid Reading Ease of 50.4, and a Simple Measure of Gobbledygook (SMOG) of 9.6. Flesch Kincaid Grade Level and Reading Ease are ideal for general use, and the target score is <8 and <60, respectively (Kincaid et al., 1975). The SMOG is the gold standard for HCR information, and the target score is <8 (McLaughlin, 1969). The AHRQ (2015) does warn about using readability scores such as the assumption that longer words and sentences are more complex than shorter comparisons, grade level does not measure suitability or the active role of the reader (such as maintaining attention and content organization) and using computerized readability scores may result in misleading results as the text must be prepared first.
Process for Approval for Use Within the Clinical Setting
The organization did not require any review or approval of these materials or readability analysis. Because this was considered a new service line with an expert surgeon and NP, the materials were at their discretion. The NP had previous specialty organization experience with healthcare readability and had executed an extensive review of patient, population, and organizational needs; consequently, the education was tailored to meet these needs. Administrative endorsement at the time required a quick put-through. However, in retrospect, the lack of a formal review process undermines the principles of HL as it demonstrates a paternalistic view relying on the HCP's perception of patient HL (Griffeth et al., 2022; Morrison et al., 2019).
The starting marketing budget for this program was $4,000 per year. The costs for developing the materials were considered overhead costs related to the program NP, information technology nurses and deployment team, and marketing personnel's time for the video shoot and webpage upload. The video cost roughly $2,500, including one videographer who edited the video. The video took three hours, not including 1 h of set-up and take-down by the videographer. The total hours in the first three months of development were 100; after that, 5 to 10 h monthly were allocated to edits based on feedback. There were no printing costs associated with the PPT primer or stool log. The FAQs were part of the discharge instruction after-visit summary.
Evaluation of Project Pilot and Recommendations
Because a formal review of the project deliverables did not occur, specifically the PPT primer and discharge education FAQs, revisions came about based on user feedback. Users included patients, families, and HCPs, primarily nursing and APPs. The initial primer did not include diet information; however, the families needed to remember which foods to avoid or use, therefore this information added approximately five months after implementation. The FAQs did not require editing based on feedback. The video could not be edited; however, as of today, the video has 279,409 views on YouTube.
There were approximately 50 BMP (retention enema) patients from August 2018 through November 2021 who underwent BMP; during this period, there were no readmissions for this patient population. There was 100% adherence to the program while the patients were enrolled.
Based on lessons learned, a formal patient/parent consultation council to review materials pre- and post-implementation and ongoing should be considered, including representatives of the two predominant languages spoken in the area (Creole and Spanish). Bray and Sinha (2017) and Xie et al. (2021), for example, used parent consultation groups, readability and parent feedback (a sub-group with different levels of HCP experience), professional input and feedback, and a final review by the patient information officer (similar to an organizational patient advocacy council) in their development of patient-teaching materials. These efforts are considered HL-informed approaches (Reeves et al., 2021). Bray and Sinha (2017) further reviewed the advice received with scientific rigor to ensure the leaflet's accuracy. Efforts to have formal universal HL processes such as plain language and clear communication, teach-back method, demonstrating and drawing pictures, follow-up with patients, brown bag medicine review, and addressing language differences as described by Griffeth et al. (2022) are essential in future iterations or initiatives need to be incorporated. The focus of these projects needs to be patient-family-centric, establishing HL-informed and sensitive information and interventions that positively impact healthcare costs and, most importantly, improve patient outcomes. Organizational leaders must commit to ensuring that patients and families receive appropriate resources in these efforts.
From a marketing budget standpoint, many variables must be considered; only a few are enumerated here. These include the number and type of educational materials and the cost of printing (based on needs assessment), producing, and distributing the materials. The length and number of videos and complexity (for example, voiceovers, titles, music, actor/model or actual patients, patient or family testimonials, remuneration, if any, and legal clearance), the higher the cost. If a formal review of pre- and post-production is needed or planned, the cost of revisions must also be considered in budget planning.
Future endeavors such as those presented here will use a more formal approach to HL and access to several tools that support HL-informed initiatives, such as The Patient Education Materials Assessment Tool and User's Guide (AHRQ, 2020b), resources found in the Centers for Disease Control Clear Communication Index (2021), the Plain Language Action and Information Network (U.S. General Services Administration, 2022), and the HHS HL Resources (HHS, 2022). Thankfully, the PCRC NP did have some experience with HL and knowledge of the population's needs and was able to implement these in this project.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.