
Abstract
Early neurological deterioration (END) is associated with increased mortality and morbidity. Although several predictive factors have been reported, there are little data about the hemodynamic factors. Our aim was to determine the capacity of cerebral hemodynamic reserve (CHR) to predict END. We studied 100 hospitalized patients with a first ever ischemic stroke of the middle cerebral artery (MCA) within the first 24 hours of symptoms onset. END was defined as a drop of at least one point in the Canadian Stroke Scale between admission and 72 hours. The mean flow velocity (mV) in the MCA and the CHR were measured by means of transcranial Doppler within the first 24 hours of admission. The CHR was expressed as the percentage increase in the MCA mV divided by the absolute increase in the end-tidal CO2 pressure in mm Hg after carbogen inhalation. END was observed in 23 patients. Reduced values of the mV in the symptomatic MCA (P = 0.043) and of the CHR in the symptomatic hemisphere (P < 0.001) were significantly associated with END. A CHR of less than 2%/1 mm Hg was independently associated with END (OR 8.45, 95% CI 1.82–39.2) after adjusting for potential confounders. CHR impairment within the first 24 hours of acute ischemic stroke is associated with a higher risk of END. This technique may be useful in selecting patients requiring a more intensive management.
Keywords
Early neurological deterioration (END) has been reported in 26% to 43% of patients with acute ischemic stroke and is associated with increased mortality and morbidity rates (Castillo, 1999;Dávalos et al., 1999, 2001). Hemodynamic factors such as mean velocity (mV) of blood flow in the middle cerebral artery (MCA) measured by transcranial Doppler (TCD), cerebral blood flow (CBF) determined by positron emission tomography (PET) or single photon emission computed tomography (SPECT), and cerebral hemodynamic reserve (CHR) have been related to the final infarct volume and long-term outcome (Derdeyn et al., 1999;Giubilei et al., 1990;Kaps et al., 1992;Marchall et al., 1993;Rubin et al., 2000). However, only one study has investigated the influence of hemodynamic factors in deteriorating stroke. In a TCD study of 93 patients within the first 6 hours of hemispheric stroke, Toni et al. (1998) found that normal TCD study was an independent predictor of early improvement, whereas the absence of MCA flow in TCD examination was an independent predictor of END.
The CHR estimates the additional CBF that can reach the distal territory of a brain artery when circumstances require. This parameter depends particularly upon the presence of a proximal vessel stenosis, effective collateral circulation, and blood viscosity (Derdeyn et al., 1999). CHR is calculated by different methods depending on the vasodilator stimulus (CO2 inhalation, acetazolamide, apnoea) and the CBF measurement technique (PET, SPECT, TCD, Xenon-CT) that are used. TCD is used in the MCA territory assuming an equivalence in the increase of MCA mV and the increase in CBF (Chimowitz et al., 1993). A high correlation between changes in the MCA mV and CBF has been confirmed by PET studies, regarded as being of reference (Derdeyn et al., 1999).
In patients with carotid artery stenosis, a CHR under the normal values indicates the loss of autoregulation and the failure of collateral circulation and, hence, an increased risk of stroke (Chimowitz et al., 1993;Ringelstein et al., 1998). Despite the influence of CHR upon long-term outcome, no study has attempted to determine its value as a predictor of the early neurologic course in acute ischemic stroke. The aim of this study was to determine the capacity of CHR, evaluated by TCD in the acute phase of stroke, to predict END.
PATIENTS AND METHODS
Patients
We studied 100 patients from a total of 352 patients consecutively admitted between January 1999 and June 2001 with a first ever hemispheric ischemic stroke of less than 24 hours duration from the onset of symptoms. We excluded patients with lacunar infarction (n = 100), posterior circulation infarction (n = 38), lack of ultrasonographic temporal bone window (n = 44), and any factors such as internal carotid artery stenosis higher than 70%, noncontrollable blood pressure, anemia, infectious disease, previous lung disease, and lack of collaboration (n = 70) that interfere with the interpretation of CHR values. Patients with an intracranial hemorrhage (n = 79) or transient ischemic attack (n = 75) or admitted more than 24 hours from stroke onset were also excluded (n = 98). The protocol was approved by the Ethics Committee of our hospital, and informed consent was given by patients or their relatives.
Clinical evaluation
At admission, blood pressure and body temperature were recorded, and blood samples were taken to measure blood glucose and other parameters. Stroke severity was evaluated using the Canadian Stroke Scale (CSS) by an experienced neurologist specialized in cerebrovascular pathology. Following the TOAST criteria, stroke subtype was classified as large-vessel disease, cardioembolic, small-vessel disease, or cryptogenic (Adams et al., 1993).
Patients remained in the Stroke Unit for 72 hours and were continuously monitored in a semiintensive manner and treated in accordance with published guidelines (Adams et al., 1994). ECG, oxygen saturation by pulse oxymetry, respiratory, and cardiac frequency were continuously monitored, while noninvasive blood pressure, body temperature, capillary glucose levels, and swallowing function were determined several times a day. The CSS was evaluated every 4 hours by the nursing staff and every 12 hours by the neurologist. In the specific case of blood pressure, measurement was made using a Philips V24C device every hour during the first 24 hours, every 4 hours from 24 to 72 hours, and every 8 hours thereafter.
Following previously established criteria, END was defined as a drop of at least one point in the CSS from the first evaluation to 72 hours after symptoms onset, excluding the area of orientation (Castillo, 1999). Patients with fluctuating symptoms not showing CSS decline at 72 hours were not diagnosed as having END. When END occurred, blood pressure, body temperature, oxygen saturation, and capillary glucose were measured to exclude potential factors associated to deterioration. The modified Rankin scale (mRS) and the Barthel index (BI) were used to evaluate stroke outcome at 3 months. Scores of 95 and 100 on the BI and 0 to 2 on the mRS were considered to indicate a favorable outcome.
Cranial CT evaluation
A cranial computed tomography (CT) scan was performed in all patients upon admission to evaluate early signs of infarction in the MCA territory such as hypodensity of brain parenchyma (basal ganglia, cortex), and focal brain swelling (effacement of sulci, ventricular compression). A second CT study was performed between 48 and 72 hours of admission, or earlier when END was diagnosed, to detect potential hemorrhagic transformation and mass effect.
Transcranial Doppler evaluation
A first TCD study, recording the mV and the Gosling pulsatility index in the anterior cerebral artery (ACA), the middle cerebral artery (MCA), and the posterior cerebral artery (PCA) through the temporal window, was performed upon admission to the emergency department using a portable device with a 2-MHz probe (DWL Elektronische System GmbH). The CHR was evaluated within the first 24 hours of stroke onset once the patient had been admitted to the stroke unit using a Multidop X4 ultrasound device (DWL Elektronische System GmbH), storing the sonographic recording on a hard disk for off-line analysis. Extracranial continuous Doppler or color-coded duplex ultrasound of the internal, external, and common carotid arteries was performed with linear transducers (5–8 MHz). The peak systolic velocity of greater than or equal to 120 cm/s was the threshold for the diagnosis of a greater than 50% stenosis. Patients who were diagnosed as having severe internal carotid artery stenosis (≥70%), taking into account the peak systolic velocity in the jet of the stenosis, the peak systolic velocity in the most distal poststenotic ICA, intrastenotic and poststenotic turbulence in the ICA (spectral broadening), direction of the ophthalmic artery flow, the presence of collateral flow via communicating arteries of the circle of Willis, and the absolute asymmetry in flow velocity and pulsatility measured in the CCA and middle cerebral artery, were excluded from the study (de Bray and Glatt, 1995).
MCA mV values lower than 32 cm/s were considered to be abnormal. This value represents the percentile 5 of a control group of 118 healthy subjects studied in our laboratory (Segura et al., 1999). The CHR study was performed using a headset, allowing simultaneous sounding of both MCAs through the temporal window and CO2 inhalation as the vasodilator stimulus after the method described by Bishop et al. (1986). The mV of both MCAs was continuously recorded at a depth of 50 mm, and the end-tidal CO2 (EtCO2) pressure in mm Hg was determined with a CO2 analyzer (Capnogard 1265, Novametrix Medical Systems, Inc., USA). The patient first breathed room air until a steady expiratory EtCO2 and a basal mV record of at least 15 cardiac cycles was obtained. The patient was then asked to inhale carbogen (a mixture of 95% oxygen and 5% of CO2) for 3 minutes through an anesthetic mask with the reservoir tightly fitted over the mouth and nose. EtCO2 and mV were continuously recorded for at least another 15 cardiac cycles. The CHR of each side was expressed as the percentage increase in mV occurring during the inhalation of carbogen divided by the absolute increase in EtCO2 (%/mm Hg). Abnormal CHR was established as a lower than 2% increase in mV for every mm Hg increase in the EtCO2. This value corresponds to the percentile 5 of the CHR value in a control group of 100 healthy subjects studied in our laboratory (Álvarez et al., 2002).
Statistical analyses
Proportions between groups were compared using the chi-square test. Continuous variables were expressed as mean and standard deviation or median and quartiles and were compared by the Student's t-test or the Mann-Whitney tests as appropriate. Logistic regression analysis using the enter approach was performed to determine the variables recorded upon admission that were independently associated with END (no = 0, yes = 1). Variables with values of P < 0.05 on univariate testing were included in this model.
RESULTS
END was detected in 23 patients, whereas 33 remained stable (three of them had transient fluctuations) and 44 improved. The median fall in the CSS score was 1.5 points (range 1–5). END occurred within the first 24 hours in 17 patients, between 24 and 48 hours in 4 patients, and between 48 and 72 hours in 2 patients. Associated factors of END were cerebral edema in 3 patients, hemorrhagic transformation in 1 patient, systemic complications in 6 patients (aspiration pneumonia in 2 cases and hypotension in 4 cases), and of unknown cause in 13 patients. Seven patients died, six after END, and all between days 4 and 14. There were no significant differences in the prevalence of these factors between END and non-END patients.
CHR was not evaluated in 13 of the 100 included patients; six patients had a decreased level of consciousness and an irregular respiratory pattern preventing an optimal level of hypercapnia, four patients had no flow in the MCA, and three patients developed END before the CHR study. No patients had neurologic deterioration during or immediately after CHR evaluation.
Table 1 summarizes risk factors and clinical and neuroradiologic characteristics at baseline in both groups. Older age, female gender, atrial fibrillation, history of arterial hypertension, lower CSS score at admission, and cardioembolic stroke subtype were significantly more frequent in patients with END than in those without.
Baseline clinical, biologic, and radiologic characteristics
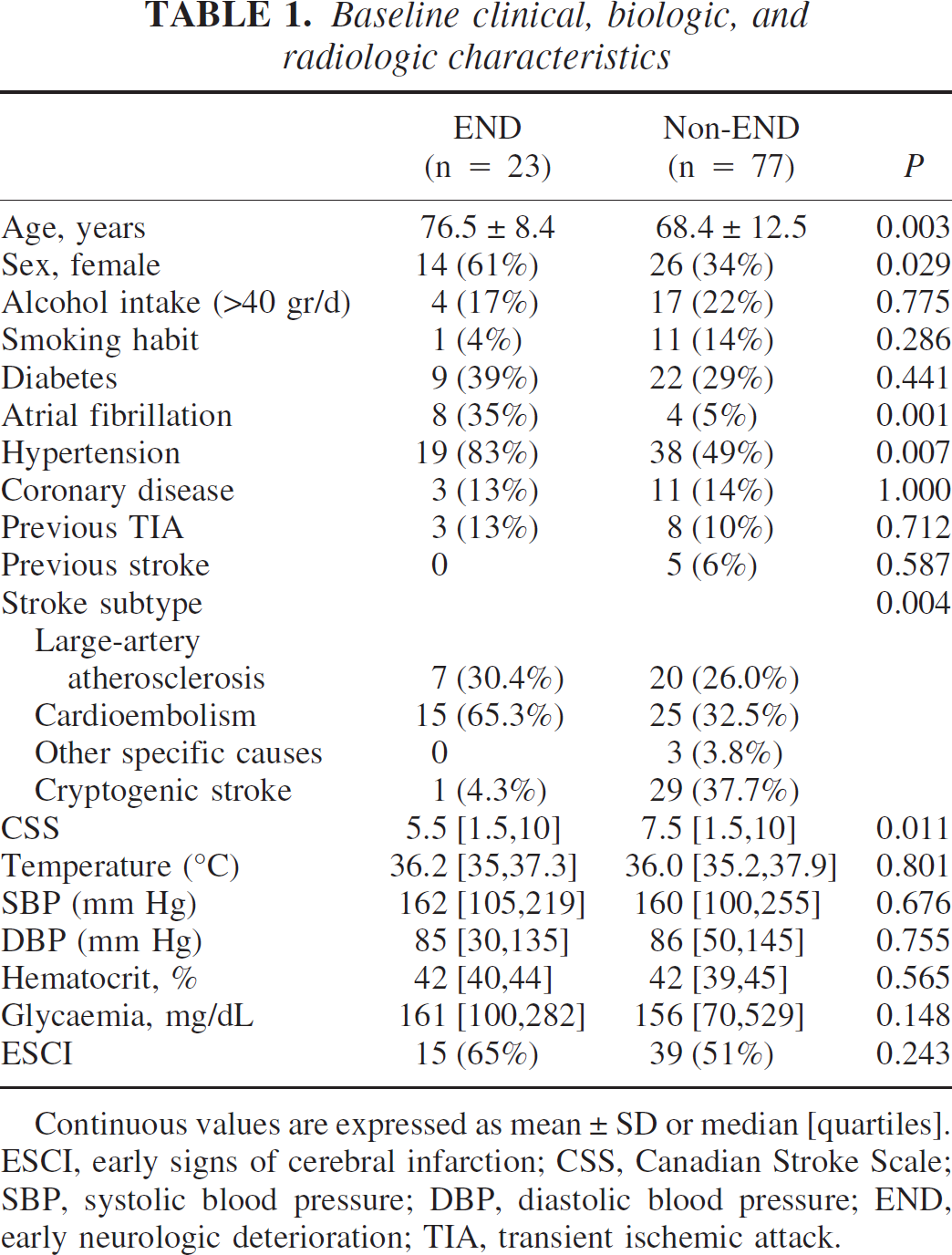
Continuous values are expressed as mean ± SD or median [quartiles]. ESCI, early signs of cerebral infarction; CSS, Canadian Stroke Scale; SBP, systolic blood pressure; DBP, diastolic blood pressure; END, early neurologic deterioration; TIA, transient ischemic attack.
The main results of the cerebral perfusion study are shown in Table 2. The median mV in the symptomatic MCA was significantly lower in the group with END than in the group without END, whereas the median values in the nonsymptomatic MCA were similar in both groups. The mV in the symptomatic MCA was lower than the normal reference value in 34 patients and equal or higher in 66 patients. Abnormal MCA mV values were significantly more frequent in patients with END than in those without END.
Cerebral hemodynamic parameters by TCD upon admission
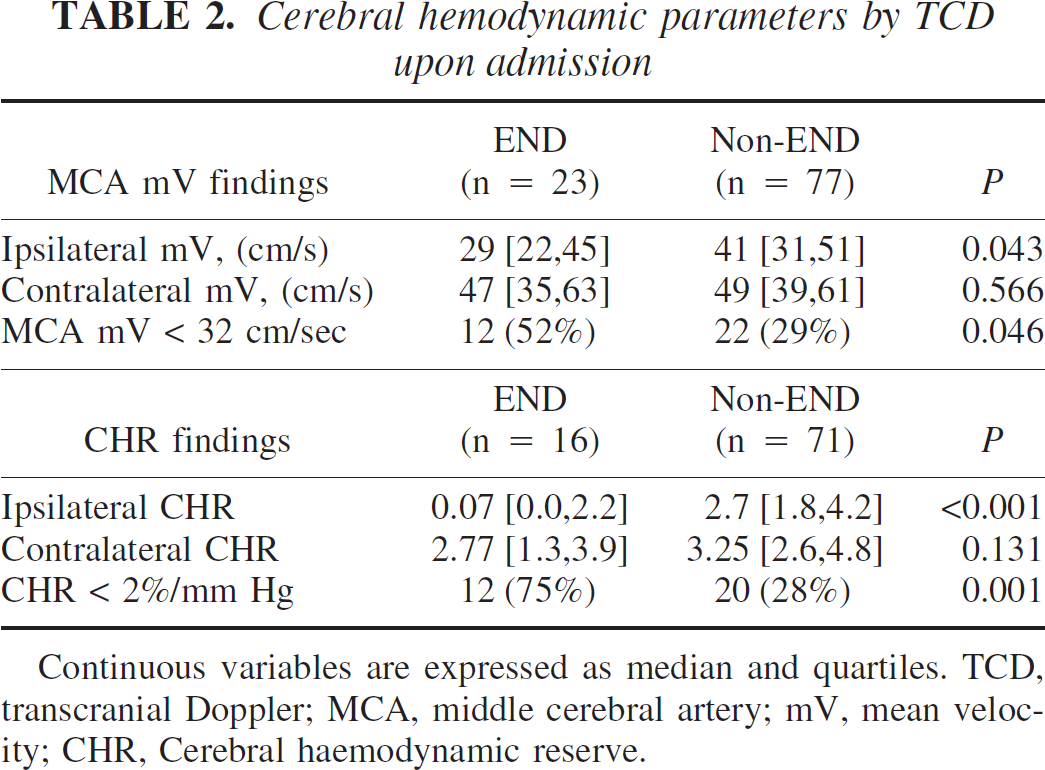
Continuous variables are expressed as median and quartiles. TCD, transcranial Doppler; MCA, middle cerebral artery; mV, mean velocity; CHR, Cerebral haemodynamic reserve.
Median values of ipsilateral CHR were better in cryptogenic stroke (3.4% [1.8,4.5]/1 mm Hg) than in large-artery atherotrombotic (2.6% [0.0,2.9]/1 mm Hg) and cardioembolic stroke (2.1% [0.6,3.5]/1 mm Hg) (P < 0.01). The median ipsilateral CHR was lower in the END group than in the non-END group (Table 2). Thirty-two patients (36.8%) had an abnormal CHR when set against the reference value of healthy controls. Abnormal CHR was significantly more frequent in patients with END than in those without END (Table 2). The sensitivity, specificity, positive predictive value, and negative predictive value of a CHR less than 2%/mm Hg for END were 73%, 74%, 38%, and 93%, respectively.
Logistic regression analysis showed that history of arterial hypertension and CHR of less than 2%/1 mm Hg within the first 24 hours of stroke onset were the only independent predictive factors of END (OR 8.45, 95% CI 1.82–39.2), after adjusting for significant variables in the univariate analysis. There was no interaction between the two variables (Table 3).
Adjusted odds ratios of END for clinical and hemodynamic variables upon admission
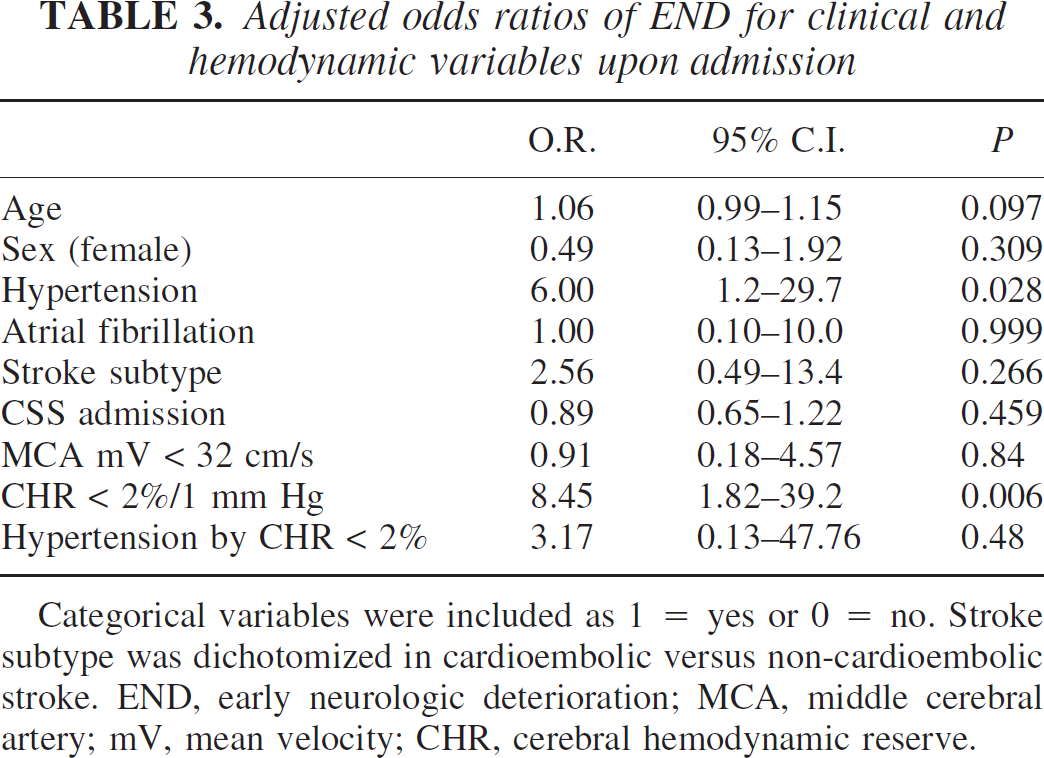
Categorical variables were included as 1 = yes or 0 = no. Stroke subtype was dichotomized in cardioembolic versus non-cardioembolic stroke. END, early neurologic deterioration; MCA, middle cerebral artery; mV, mean velocity; CHR, cerebral hemodynamic reserve.
At 3 months, 24.6% of patients had a favorable outcome (mRankin ≤ 2 and BI > 90) with CHR less than 2%/1 mm Hg and with normal CHR in 75.4% of those (P = 0.001).
DISCUSSION
A better knowledge of the early clinical course is essential for the use of emergent therapies in patients with acute ischemic stroke.
The present study shows that a CHR of less than 2%/1 mm Hg within 24 hours of stroke onset results in an increase of approximately eightfold in the likelihood of subsequent END. Our sample seems to be representative of patients suffering from acute MCA hemispheric stroke, as rates of progression and associated factors were similar to previously reported ones (Castillo, 1999;Dávalos et al., 1999, 2001;Serena et al., 2003). Patients with transient ischemic attack (TIA), lacunar infarction, and stroke arriving at the hospital more than 24 hours after stroke were excluded from our population, and hence these results cannot be applied to a general stroke population.
The analysis of flow patency by TCD has recently been evaluated in detail and validated in acute cerebral ischemia with the result that MCA recanalization has been shown to be the main prognostic factor and predictor of good outcome (Akopov and Whitman, 2002;Alexandrov et al., 1999;Demchuk et al., 2000). However, neurologic and hemodynamic worsening can occur in patients with normal TCD pattern at admission. The clinical significance of these findings remains unclear, but thrombus propagation or loading of a new embolus next to the initial occlusion have been suggested (Akopov and Whitman, 2002;Toni et al., 1998). The results of the present study suggest that impaired CHR may be a further contributing factor to early clinical deterioration.
To the best of our knowledge, the present study is the first to associate CHR impairment with END. Although current knowledge does not allow us to identify the specific mechanism of END, and our study was not designed to analyze these mechanisms, this association may be the result of a decrease in CBF and collateral circulation insufficiency. Experimental studies have reported that a progressive decrease in CBF of between 50 and 20 mL/100 g/min is initially associated with arterial vasodilatation to maintain a constant cerebral blood volume and later with an increase in the cerebral oxygen extraction fraction. When CBF is less than 20 mL/100 g/min, the cerebral metabolic rate of oxygen decreases and the oxidative metabolism is reduced. This area is still potentially viable if the CBF is restored, but infarct occurs if the CBF drops to 10 mL/100 mg/min, and the symptoms become irreversible (Lee et al., 2000). Although the velocity in the MCA does not directly correlate with absolute values of cerebral blood flow (CBF), changes in velocity do correlate with changes in CBF when the MCA has a constant diameter. Vasomotor reactivity enables constant CBF maintenance over a wide range of systemic blood pressure by varying the diameter of the intracerebral arterioles. Maximal dilatation of the intra-cerebral arterioles, however, leads to decreased cerebral perfusion pressure and a corresponding reduction in CBF. If the CBF is maintained through MCA or by collaterals distal to the arterioles of the MCA, it cannot be determined by TCD. However, not knowing the mechanism of the cerebral flow does not affect the TCD results. Impaired CHR at stroke onset probably indicates that the vasodilator compensatory mechanisms are exhausted and consequently that there is a high risk of recruitment of the oligemic ischemic tissue into infarction. In contrast, normal CHR may suggest recanalization or competent collateral blood flow preventing the growth of the infarcted area. It is interesting to note that we found that when CHR was normal 93% of patients remained stable or improved.
The reduction of the regional CBF in MCA territorial infarctions makes the compensatory collateral blood flow essential to the maintenance of CHR. In the present study, atherothrombotic and cardioembolic strokes had similar CHR, although the former had a lower END rate. Previous occlusive disease of the cerebral or precerebral arteries in patients with atherothrombotic stroke might promote the progressive development of a competent collateral network and consequently result in a lower rate of progression when stroke occurs in atherothrombotic than in cardioembolic stroke. In the present study, patients with cryptogenic stroke had a better CHR than those with large-artery atherothrombotic and cardioembolic stroke, which explains the almost complete absence of END in this subgroup. We are unable to offer a conclusive explanation for this finding, although the higher proportion of younger people, lower prevalence of classical stroke risk factors, lower stroke severity at admission, and smaller infarct volume in patients with cryptogenic stroke in our series may well contribute to a better CHR.
Other TCD data had less predictive value. Although there was a significant association between the presence of an MCA mV less than 32 cm/s and the progression of neurologic symptoms in the univariate analysis, the multivariate analysis showed that CHR was the only hemodynamic independent predictor of END and that mean velocity was not a significant factor after adjusting for confounding factors. The characteristics of our study should be taken into account in interpreting this result. Although MCA occlusion has been associated with both END (Toni et al., 1998) and poor outcome (Akopov and Whitman, 2002) within 6 hours of stroke onset, CHR measurement is not possible in these circumstances and so has only been calculated in patients where MCA blood flow is detected.
This study has some further limitations. Patients with lack of collaboration or absent temporal bone window could not be included, although this is also a limitation in clinical practice. Flow grade changes have not been evaluated by serial TCD, and we have no direct information about collateral flow. Furthermore, the fact that most patients were studied more than 6 hours after the onset of symptoms means that many patients probably recanalyzed before examination. It is likely that with a shorter temporal window, of say 6 hours, only flow patency would be of clinical relevance as it has been shown that partial or total occlusion is a strong prognostic factor (TIBI classification) (Akopov and Whitman, 2002;Toni et al., 1998), and this has been found to occur during this period as often as in 60% to 80% of patients with nonlacunar MCA cerebral infarction (Molina et al., 2001). The partial or total occlusion of the MCA would also prevent the performance of CHR studies. The present study suggests that it is the CHR rather than the TIBI pattern or MCA mean velocity that should be given the greatest attention after immediate acute management.
CONCLUSION
We find that the study of CHR by TCD and CO2 in the first 24 hours of MCA stroke is a powerful predictive tool of early neurologic deterioration. This examination is safe, cheap, and easy to perform in day-to-day clinical practice and requires only equipment that is widely available. These findings may also be useful in the design of future clinical trials and in improving the criteria for selecting those patients requiring a more intensive management through such options as intensive Stroke Unit monitoring and revascularization therapy.
Footnotes
Acknowledgment
The authors thank Dr. María García (Biostatistics Unit, Hospital Universitari Doctor Josep Trueta, Girona, Spain) for her comments on the design and interpretation of the statistical analysis.