
Abstract
There are considerable variations in the size and the origin of internal carotid arteries (ICAs) of New Zealand white rabbits. A simple test that could correctly identify the ICA could facilitate intracarotid delivery of drugs and embolic material for research in these animals. Five conventional methods for identifying the ICA proved inferior to a novel retinal discoloration test (RDT). A positive RDT implies a change in color of the retinal reflex after injection of 0.2 mL of indigo-carmine blue (ICB). We conclude that RDT is a useful test for correctly identifying and isolating the ICA in this animal species.
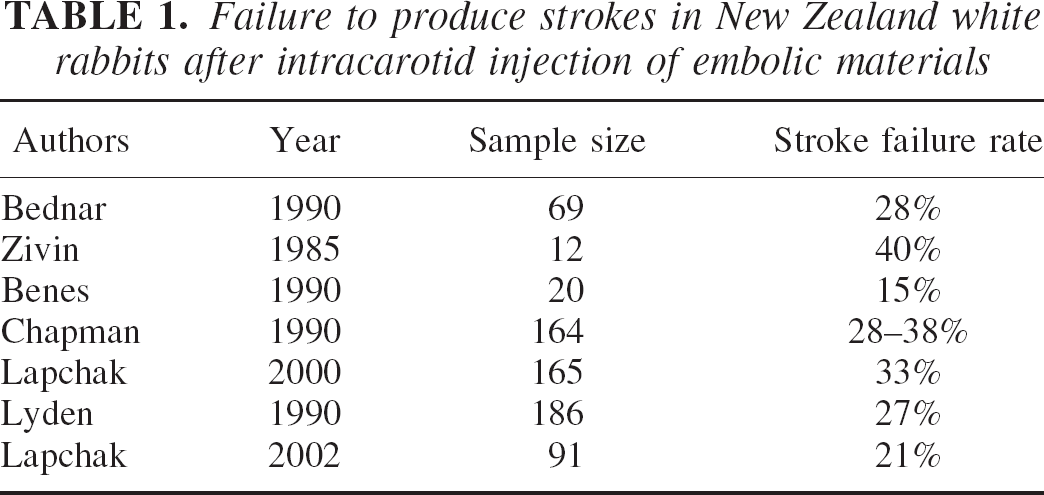
Because of their primate-like separation of intra- and extracranial arterial supply, rabbits provide a convenient model for stroke-related research (Edvinsson et al., 1993). However, this animal species shows significant differences in response to intracarotid drugs. Some investigators have reported a 100% increase in cortical after intracarotid adenosine, whereas others failed to observe any effect of the drug (Heistad et al., 1981; Puiroud et al., 1988). Similarly, there is an approximate 25% to 30% failure rate to produce infarction after intracarotid injection of embolic materials (Table 1). Investigators who use this animal species have used several means for identifying the internal carotid artery (ICA) (Table 2). Considerable variations in the size and the origin of these vessels have been reported in literature (Lee et al., 1994; Scremin et al., 1982). Such variations make it difficult to correctly identify the vessel and isolate its branches. Arguably, cerebral angiography remains the best minimally invasive technique that can reliably identify the ICA. However, access to small animal fluoroscopy is only available to some investigators, and even when it can be undertaken, interpretation of the angiograms may be difficult in laboratory settings. As many as 10% of rabbit cerebral angiograms could not be interpreted in one study (Lyden et al., 1990). Therefore, we investigated the possibility of developing a simple test to correctly identify the vessel.
Failure to produce strokes in New Zealand white rabbits after intracarotid injection of embolic materials
Methods used to identify the internal carotid artery
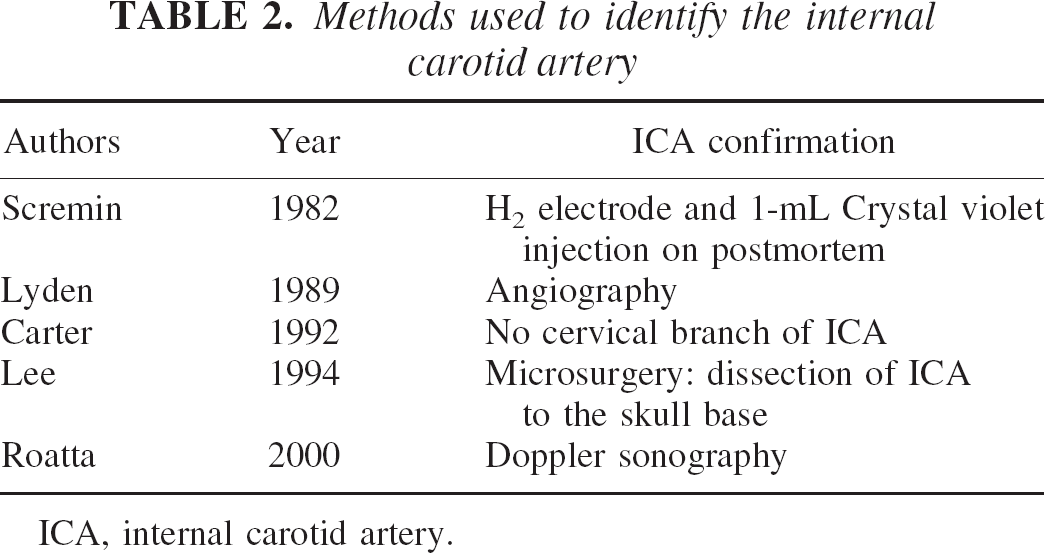
ICA, internal carotid artery.
The internal ophthalmic artery of the rabbit is the first intracranial branch of the ICA that supplies the retina (Scremin et al., 1982). We hypothesized that when the ICA was correctly identified and isolated, infusion of a small volume (0.2 mL) of dye, such as indigo carmine-blue (ICB, C16H8N2Na2O2S2, Sigma Chemical Co., St. Louis, MO, U.S.A.), would result in a change in pupillary reflex from red to blue because of discoloration of the retina. The discoloration of the iris alone or a change in pupillary reflex along with staining of the periorbital tissue would not be considered a positive retinal discoloration test (RDT) because the iris and the periorbital tissue are also supplied by the external carotid (Scremin et al., 1982). We evaluated the outcome of six tests, including the RDT, against a gold standard test. The gold standard was defined as the staining of the cortical arteries as observed directly through a cranial window by 0.2 mL of the dye or occurrence of transient electrocerebral (EEG) silence with 0.2 mL of intracarotid 1% propofol (Diprivan 1%, Astra Zeneca Pharmaceuticals LP, Willington, DE, U.S.A.), an intravenous anesthetic agent.
MATERIALS AND METHODS
The experiments were performed as a part of an Institutional Animal Care and Use Committee approved protocol, which aimed to investigate the effects of intracarotid vasodilators and anesthetic drugs on cerebral blood flow. The New Zealand White rabbits (2.0 to 5.2 lb) were anesthetized with intramuscular ketamine (50 mg/kg). Subsequently, anesthesia was maintained with 1% propofol infusion of 2 to 5 mL/h. After infiltration of the incision site with local anesthetic agent, 0.5% bupivacaine with 1:200,000 epinephrine, the animals underwent a tracheotomy, femoral arterial cannulation, and neck dissection. The right common carotid arteries (CCAs) of rabbits were cannulated with a 20-cm long P-50 catheter. Putative ICA was identified and isolated by ligating all other cervical branches of the CCA. After isolating the vessel, a small paget of gel foam dipped in 0.25% bupivacaine was placed around the artery to prevent vasospasm caused by surgical trauma. The animals were then placed prone, and a craniotomy was performed to expose the dura matter. In experiments requiring cranial window placement, the dura matter was incised, and a cranial window was placed over the right temporal region. The skull anterior to the coronal suture was gently exposed, and two Laser Doppler probes (Probe 407, for Periflux System, Perimed AB, Stockholm, Sweden) were placed over both frontal lobes and secured in plastic retainers that were stuck to the skull with glue.
We evaluated six characteristics that have been used to identify the ICA based upon the anatomic description of the vessel:
Was the ICA the first major branch of the CCA? Was the diameter at least 50% the size of the diameter of the CCA? Was there a significant distal arterial branch arising from the putative ICA? Did the putative ICA bleed back, which would suggest anatomic continuity with the circle of Willis? Did the ipsilateral laser Doppler cerebral blood flow increase more than 5% by injection of 0.2 mL of saline? Was there a change in color of the pupil with 0.2 mL of ICB, that is, a positive RDT?
We selected ICB because the dye has been used in ex vivo brain slice studies for staining the vascular endothelium and does not seem to affect the vascular reactivity (Harkin et al., 1997). For intracarotid injection, a 0.5% solution of ICB in normal saline was prepared and filtered through a 20 μm filter to remove any particulate matter.
As the gold standard, we considered the identification of the ICA to be true positive when the cortical vessels discolored with the same volume of the dye as observed through the cranial window. Alternately, the experiments did not require craniotomy if there was transient (approximate 10 seconds) EEG silence with 0.2 mL of intracarotid propofol. If color change or EEG silence was not evident with a 0.2 mL bolus, additional bolus of 0.4 mL drug was injected. A note was made when additional bolus was required. Table 3 describes what were considered to be true and false positive/negative tests. Statistical evaluation was performed using SAS program. The association was assessed by chi-square analysis with continuity correction. The gold standard test was considered negative when 0.4 mL of dye or propofol was used to achieve the change in retinal reflex or EEG silence. These animals underwent further neck exploration to identify an alternate vessel or exclude additional vessels.
Definitions
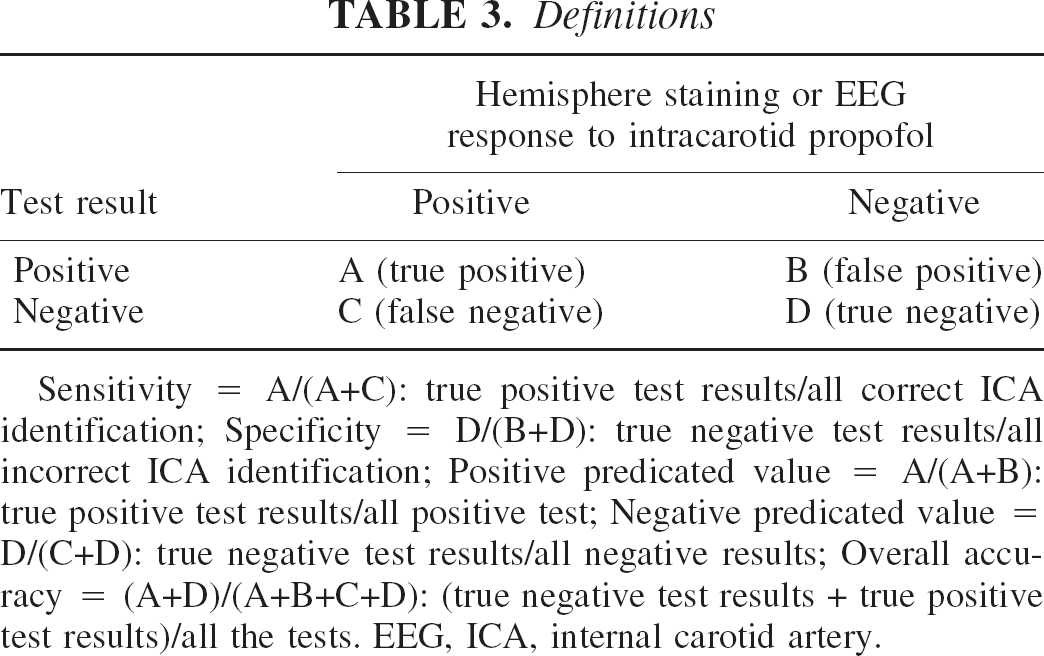
Sensitivity = A/(A+C): true positive test results/all correct ICA identification; Specificity = D/(B+D): true negative test results/all incorrect ICA identification; Positive predicated value = A/(A+B): true positive test results/all positive test; Negative predicated value = D/(C+D): true negative test results/all negative results; Overall accuracy = (A+D)/(A+B+C+D): (true negative test results + true positive test results)/all the tests. EEG, ICA, internal carotid artery.
RESULTS
A total of 69 putative ICA were evaluated in 56 New Zealand white rabbits. Cortical vessels were directly observed in 13 rabbits. In the remaining 43 rabbits, changes in EEG recordings served as the gold standard. During the study, we consistently observed considerable variations in the origin, size, and branching of the ICA. During dissection, it was difficult to differentiate the ICA from three other arteries: high cervical branches, occipital artery, and the sphenopalatine artery. As shown in Table 4, the ICA was not always the first significant branch of the common carotid artery. Arterial branching was evident at the origin of putative ICA. Often the diameter of the ICA was not greater than 50% of the common carotid artery (P = 0.88). Frequently, the ICA was much smaller than the occipital arteries, the sphenopalatine arteries, and other branches of the external carotid artery. The positive predictive value of the RDT test was 58/62 (93%). The RDT emerged to be the most reliable of all these tests with the highest specificity and overall accuracy.
Comparison of tests used to identify the internal carotid artery of New Zealand white rabbits
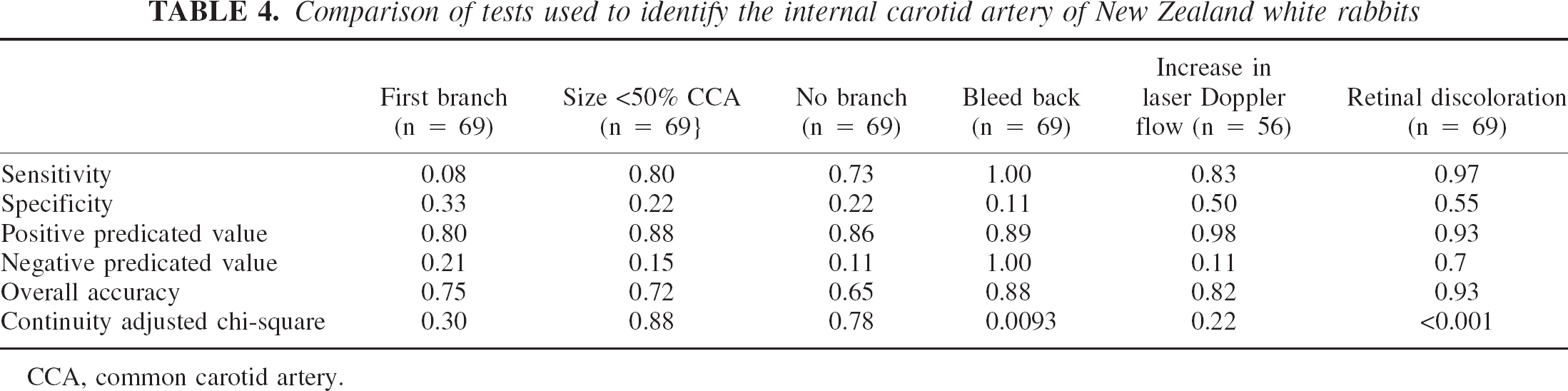
CCA, common carotid artery.
DISCUSSION
Relative isolation of intra- and extracranial circulation, a relatively large body and brain size, and the possibility of genetically engineered experimental animals all make rabbits attractive for stroke-related research (Fan and Watanabe, 2000; Lee, 1994). However, a significant problem with intracarotid research is the inability to reliably identify the ICA of these animals. Considerable variations in the cervical anatomy of these animal species have been reported in literature. Table 1 provides some examples of stroke Okay
It has been recommended that, because of anatomic variations, correct identification of the ICA may not be possible unless the arteries are dissected up to the skull base. This perhaps is the ideal approach because the basic anatomic branching of the common carotid can vary a great deal (Lee et al., 1994). For example, Scremin and colleagues (1982) have stated that the ICA has no branches after its origin, whereas Lee and others (1994) describe that the rabbit ICA often arises with the occipital artery from a common trunk. These arteries could originate either proximally or distally from the common carotid artery. A distally branching pattern runs contrary to the assertions by Scremin and colleagues (1982) and makes it difficult to correctly identify the vessel without extensive dissection.
Before using the RDT, we had difficulty in eliciting consistent pharmacologic effects of intracarotid drugs in this animal species. None of the previously described tests proved to be sufficiently accurate for correctly identifying the ICA. In this animal species, the RDT has helped us in several ways in identifying the vessel. First, the RTD provides a convenient tool to reliably identify the ICA without the need for fluoroscopy or extensive neck dissection. Second, injection of the dye also aids us in visualizing the arterial anatomy. This helps us to identify small high cervical branches and isolate them during dissection. Third, a positive RDT also helps to standardize the volume of challenge drug. Like propofol, with a positive RDT, we expect to see some pharmacologic response with 0.2 mL bolus of a challenge drug.
ICB has been extensively used in human subjects during surgery to define vascular anatomy (Crawford et al., 1980; Fujita et al., 1995; Tani et al., 2001; Taylor et al., 1987). There are conflicting data regarding the effects of this drug on the vascular endothelium. On one hand, there is evidence that NO-mediated vasodilation is active after ICB exposure. However, there is also evidence that NO-mediated response may be obtunded by ICB (Burleson et al., 1981; Harkin et al., 1997). Furthermore, severe allergic and idiosyncratic reactions may occur after the injection of the dye, although we did not encounter such problems in our animals (Gousse et al., 2000; Hammann, 1989). In theory, if there are concerns about any pharmacologic interference by ICB, then an investigator may elicit the RDT with another dye that is compatible with their experimental protocol (Burleson et al., 1981).
CONCLUSION
We believe that the RDT provides a useful tool to correctly identify the ICA of the rabbit. For the test to be optimally used, meticulous attention should be paid to the volume of the dye that is injected and its distribution in the periorbital tissue. The test can be an important tool to standardize intracarotid drug studies with drugs or embolic material in this animal species.
Footnotes
Acknowledgments
The authors thank the following staff members of Columbia University: Jodi Wagman, Administrative Assistant in the Department of Anesthesiology, for help in preparing the manuscript, and Richard Arrington, BA, Cert. AT, Manager of Anesthesiology Services, for help with technical aspects of the experiments.